3098
Accelerated acquisition and DL reconstruction to enable single shot fast spin echo (SSFSE) imaging of diagnostic quality using single coil
Sudhanya Chatterjee1, Florintina C1, Rohan Patil1, Sajith Rajamani1, Rajagopalan Sundaresan1, Uday Patil1, Preetham Shankapal1, Suresh Emmanuel Joel1, Ramesh Venkatesan1, and Harsh Agarwal1
1GE Healthcare, Bangalore, India
1GE Healthcare, Bangalore, India
Synopsis
Keywords: Image Reconstruction, Image Reconstruction, artificial intelligence, abdomen, SSFSE
Single shot fast spin echo (SSFSE) is a popular imaging approach for acquisition of high-resolution MR images in motion sensitive areas such as abdomen. In certain clinical settings, use of multiple coils setup for acquisition is not feasible (such as abdominal scans for obese subjects in non-wide bore MRI scanners). SSFSE imaging with single coil using the popular partial Fourier approach only presents risk of excessive blurring in the images. In this study we present a method to enable SSFSE T2 imaging using single coil. Proposed method is evaluated on prospectively accelerated data.Introduction
SSFSE is commonly used in acquiring 2D high resolution MR images of motion-sensitive anatomies such as 2D T2w MRI of abdomen. SSFSE involves acquiring all the phase encoding lines in k-space together. Therefore, we have a long echo train post a 90-degree excitation pulse where the signal decays with T2 over this long echo train. Since in abdominal imaging common anatomy such as liver has short T2 (60-90msec), excessive blurring of short T2 structures is observed if total readout time post excitation pulse is long. Therefore, fast MRI methods are used to reduce the number of phase encoding k-space lines thus reducing total readout time in SSFSE acquisition. Partial Fourier (PF) MRI and parallel imaging (PI) fast MRI techniques are commonly used in multi-coil setups [1,2].Obesity is common cause of multiple of diseases leading to abdominal MRI. Use of multi-coil setup for obese patient in non-wide bore commercial MRI systems is challenging, thus requiring single channel body coil acquisition. PI cannot be used with single channel coil and PF imaging alone does not reduce the number of phase encoding lines sufficiently to obtain clinically acceptable image quality. In such scenarios additional acceleration is required with PF factors. In this work we present a method to obtain SSFSE T2 images using single coil of diagnostic quality.
Method
The proposed method consists of an k-space subsampling strategy and corresponding DL-based image reconstruction method.k-space undersampling
Echo train length (ETL) for abdomen SSFSE T2 acquisition needs to be chosen so-as-to avoid excessive T2-blurring in the data. This is critical while we are using single coil (leading to higher echo-spacing). In such scenarios, even aggressive levels of PF factors are not sufficient to avoid excessive T2-blurring in the acquired data. Hence, additional undersampling is done post the PF step. Steps in k-space undersampling:
- PF to be acquired is determined by the echo-spacing and desired TE. Minimum of 12 lines around center of k-space determine the minimum desired TE.
- Alternate k-space lines in remaining k-space in positive half of the k-space is marked for acquisition. This determines the maximum acceleration or minimum ETL with body coil.
- Depending on the desired ETL/acceleration factor, missing k-space locations near the center of k-space in positive half is marked for acquisition.
DL-based reconstruction
Reconstruction is performed using unrolled algorithm-based DL reconstruction [3]. Objective is to learn MR reconstruction for images acquired on single coil using provided scheme of undersampling i.e., remove undersampling aliasing effect and perform PF reconstruction for single coil MRI data. We used model-based method for DL reconstruction [4]. As shown in [4], the expression of recursive problem solution for single channel MRI can be computed analytically.
In-house data was used for model training. Retrospectively undersampled data was used to train the DL method with the corresponding fully-sampled data as the ground truth. Mean absolute error and structural similarity index measure were used as loss function for training.
Data acquisition for prospective evaluation
Three volunteers were scanned at 1.5T commercial MRI scanner (GE Healthcare) using 12-channel body array coil. Informed consent was obtained from two volunteers in the IRB approved study. Patients were scanned using SSFSE with FOV=38.0cmx30.4cm (rectangular FOV), Matrix size=256x192, slice thickness=7mm, slice-gap=1mm, number of slices=24, TE=80msec.
For each volunteer, SSFSE T2-w datasets were acquired with acceleration factors (R) of 1.80, 2.05 and 2.25. ETL for acquisition with R of 1.8, 2.05 and 2.25 were 82, 70 and 64 respectively. Acquisition times for SSFSE T2-w with R of 1.8, 2.05 and 2.25 were 15 seconds, 13 seconds, and 12 seconds respectively.
Results
Reconstructions for prospective data acquired on single coil with R of 1.80, 2.05 and 2.25, are shown in Figure-2 and Figure-3. Reconstructions for accelerated SSFSE T2 scans with AI-based IQ enhancement is shown in Figure-4. Prospective data from three volunteers were used to evaluate performance of the proposed method. AI-based IQ enhancement was performed for all images post undersampled MRI reconstruction using DL. These images were rated based on the Likert scale shown in Figure-5 by a senior radiologist with more than 30 years of experience. Across three levels of acceleration for three volunteers, images received a rating of 7. In two out of the three subjects, radiologist preferred data acquired with R of 2.05 to the others.Discussion and Conclusion
In this work we demonstrated feasibility of obtaining SSFSE T2-w images of abdomen using single coil. This is useful in clinical scenarios where subjects cannot be scanned using surface coils. Prospectively acquired accelerated SSFSE T2 scans in three subjects (at three different levels of acceleration) were rated consistently as ‘good’ by a senior radiologist (refer to description in Figure-5 for rating 7). In a couple of cases, radiologist preferring R=2.05 reconstructed images to lower levels of acceleration suggest that by reducing ETL of the SSFSE scan (thus reducing T2-blurring) combined with DL-based reconstruction is an effective strategy to acquire SSFSE T2-w scans using single coil with diagnostic image quality.In future studies we shall evaluate the proposed method on larger volunteer population and for higher levels of acceleration.
Acknowledgements
No acknowledgement found.References
- Chen F, Taviani V, Malkiel I, Cheng JY, Tamir JI, Shaikh J, Chang ST, Hardy CJ, Pauly JM, Vasanawala SS. Variable-Density Single-Shot Fast Spin-Echo MRI with Deep Learning Reconstruction by Using Variational Networks. Radiology. 2018 Nov;289(2):366-373. doi: 10.1148/radiol.2018180445. Epub 2018 Jul 24. PMID: 30040039; PMCID: PMC6209075
- Shanbhogue, K., Tong, A., Smereka, P. et al. Accelerated single-shot T2-weighted fat-suppressed (FS) MRI of the liver with deep learning–based image reconstruction: qualitative and quantitative comparison of image quality with conventional T2-weighted FS sequence. Eur Radiol 31, 8447–8457 (2021). https://doi.org/10.1007/s00330-021-08008-3
- Liang, Dong, Jing Cheng, Ziwen Ke, and Leslie Ying. "Deep magnetic resonance image reconstruction: Inverse problems meet neural networks." IEEE Signal Processing Magazine 37, no. 1 (2020): 141-151.
- Aggarwal, Hemant K., Merry P. Mani, and Mathews Jacob. "MoDL: Model-based deep learning architecture for inverse problems." IEEE transactions on medical imaging 38, no. 2 (2018): 394-405.
Figures
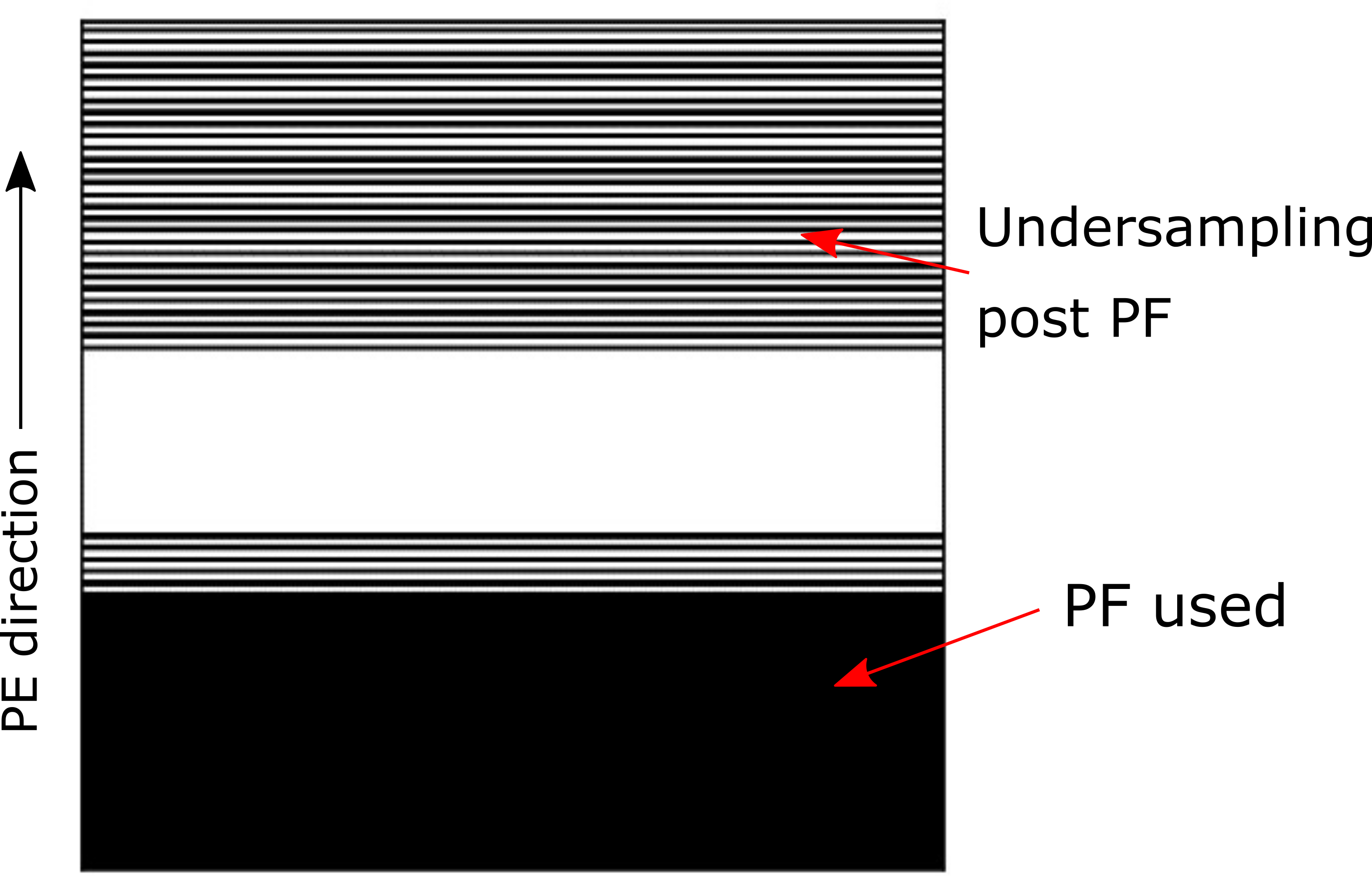
An
example of undersampling scheme used in the proposed method. Undersampling is
performed beyond standard PF factor. The acceleration factor for the above
specs of acquisition is R=2.25.
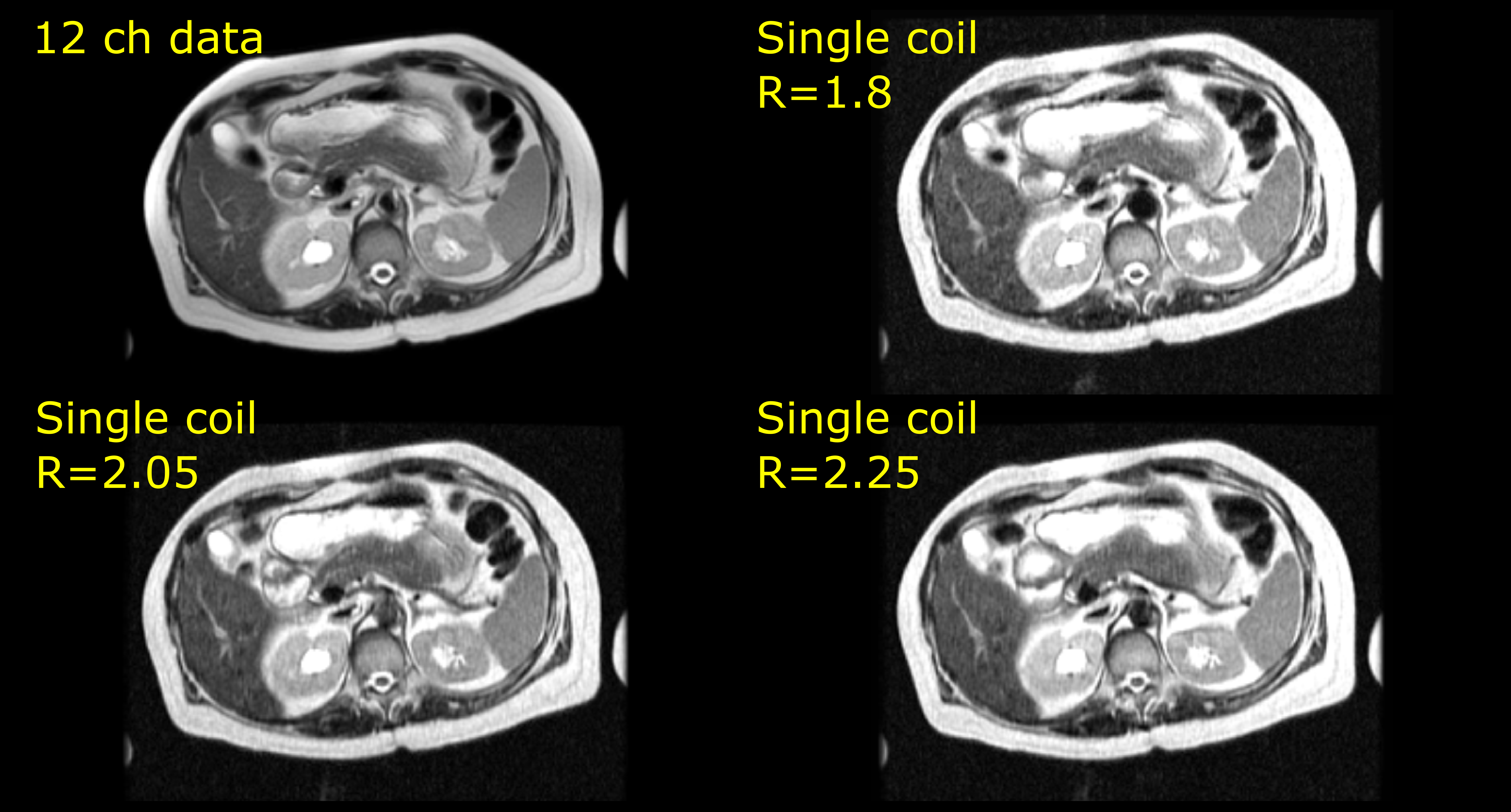
Reconstruction
for prospectively acquired accelerated data are shown here. (Top left) data
acquired with 12 channels (ETL=67), (Top right) Single coil DL reconstructed
data acquired at R=1.8 (ETL=82), (Bottom left) Single coil DL reconstructed
data acquired at R=2.05 (ETL=70), (Bottom right) Single coil DL reconstructed
data acquired at R=2.25 (ETL=64).
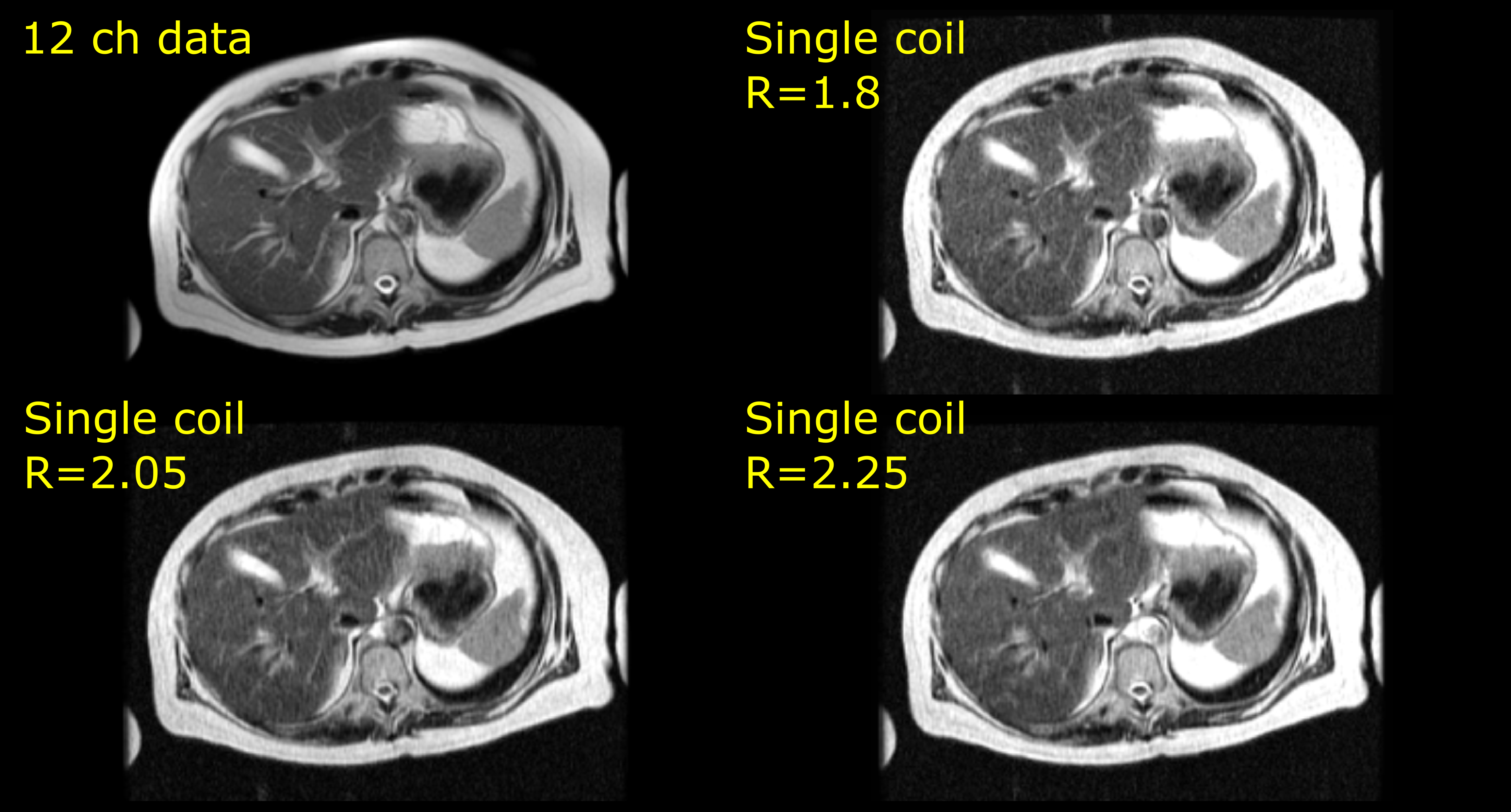
Reconstruction
for prospectively acquired accelerated data are shown here. (Top left) data
acquired with 12 channels (ETL=67), (Top right) Single coil DL reconstructed
data acquired at R=1.8 (ETL=82), (Bottom left) Single coil DL reconstructed
data acquired at R=2.05 (ETL=70), (Bottom right) Single coil DL reconstructed
data acquired at R=2.25 (ETL=64).
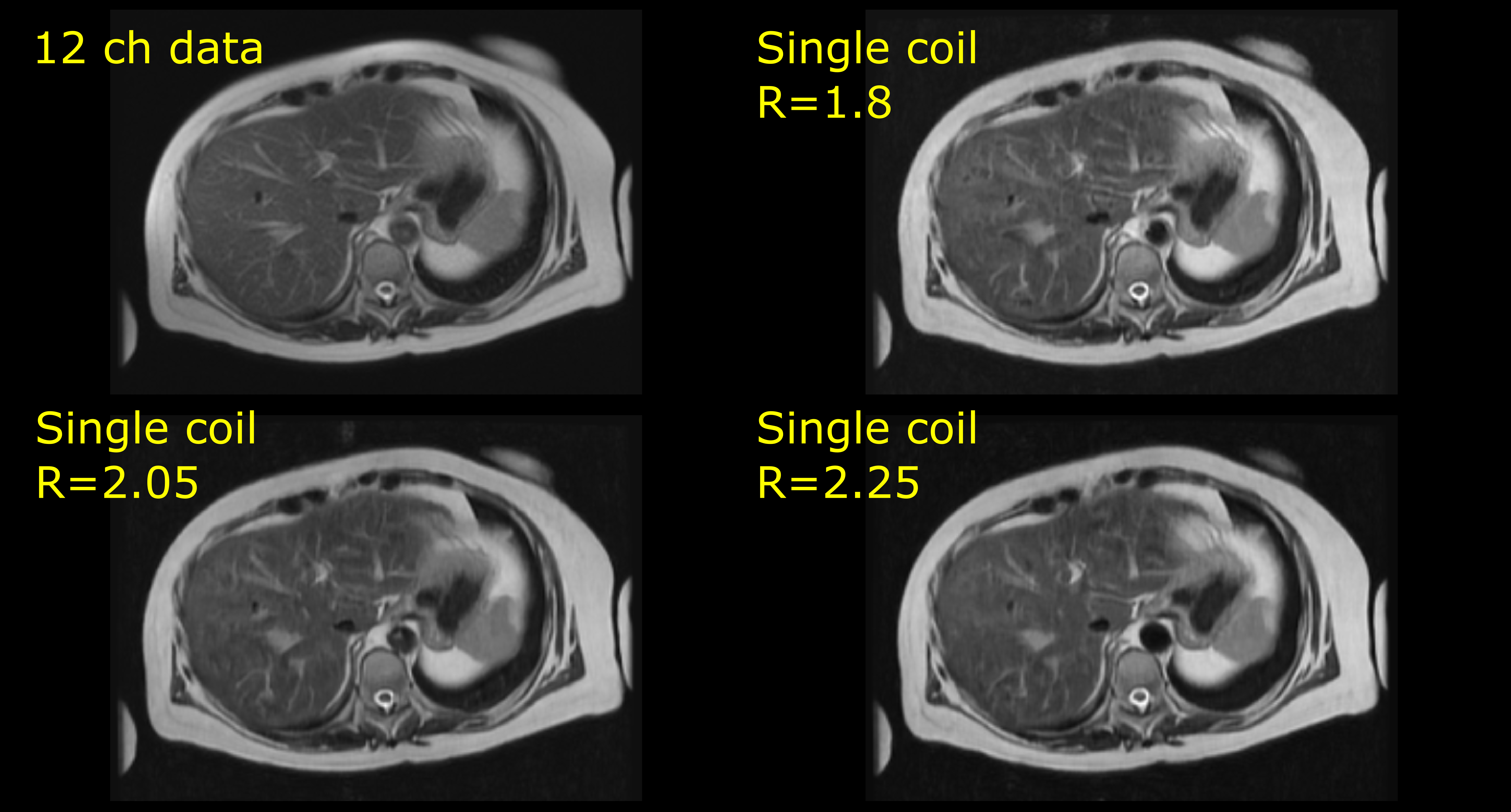
Reconstructions
with AI based IQ enhancement for prospectively acquired accelerated data are
shown here. (Top left) data acquired with 12 channels (ETL=67), (Top right)
Single coil DL reconstructed data acquired at R=1.8 (ETL=82), (Bottom left)
Single coil DL reconstructed data acquired at R=2.05 (ETL=70), (Bottom right)
Single coil DL reconstructed data acquired at R=2.25 (ETL=64).
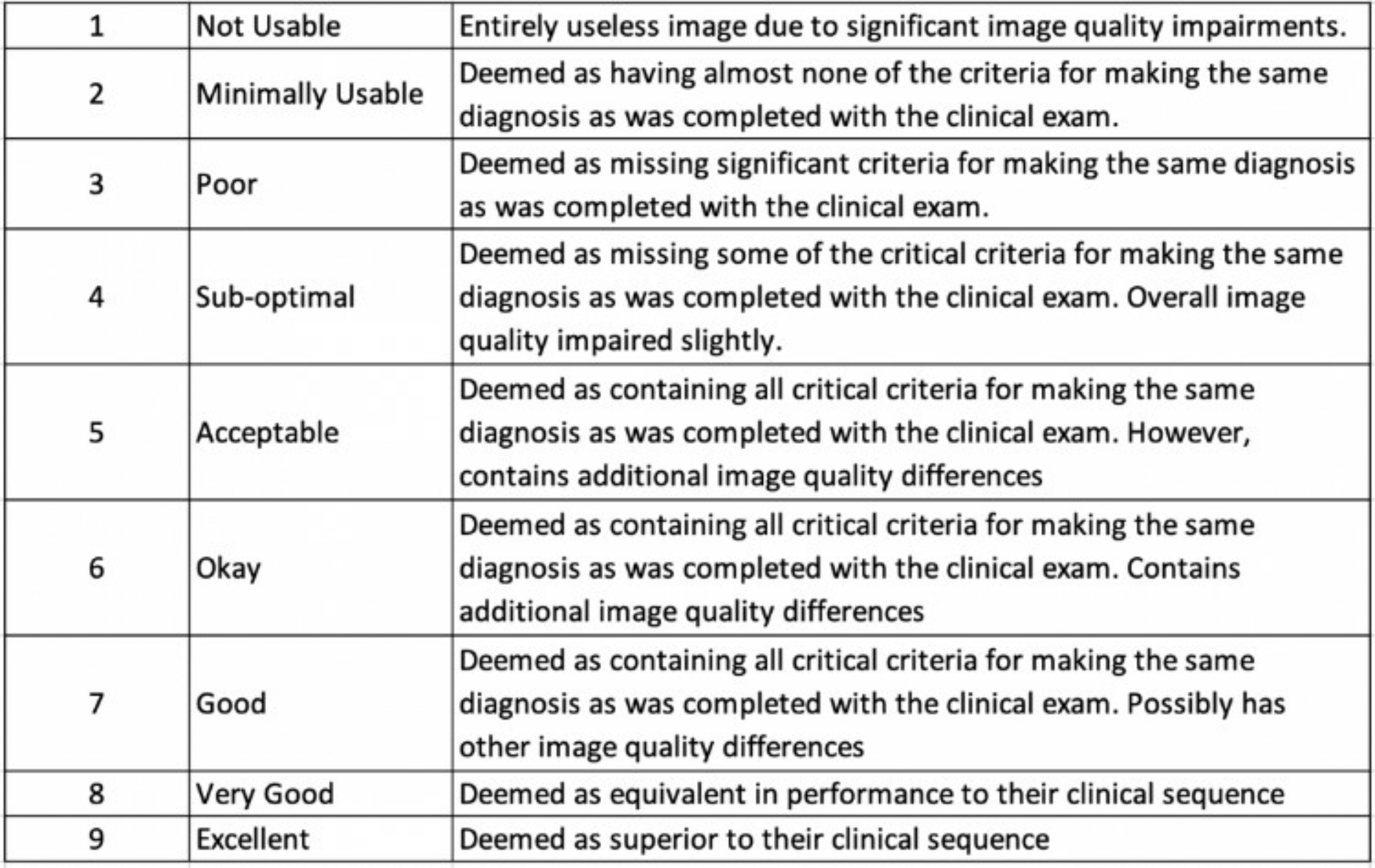
Likert
scale used to assess quality of reconstructed MR images.
DOI: https://doi.org/10.58530/2023/3098