3087
Super-resolution reconstruction of time-resolved four-dimensional computed tomography (TR-4DCT) with multiple breaths based on TR-4DMRI1Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Radiology, University of Kentucky, Lexington, KY, United States
Synopsis
Keywords: Image Reconstruction, Radiotherapy, time-resolved 4DMRI, time-resolved 4DCT, multi-breathing cycles
This study has demonstrated that the feasibility to reconstruct multiple-breath TR-4DCT via the super-resolution reconstruction framework through either CT4D→(MRBH→MRFB) or (CT4D←MRBH)→ MRFB deformable image registration. Using TR-4DCT, potential dosimetry consequences in radiotherapy of lung, liver, and pancreatic patients due to patient breathing irregularities can be readily assessed.Purpose
Severe respiratory-induced tumor motion irregularities have been reported recently as a potential cause of suboptimal radiotherapy treatment in free breathing (FB). One standard of care in patient motion management is using respiratory-correlated (RC) four-dimensional computed tomography (4DCT) [1] to simulate patient breathing motion. However, a snapshot single-breath 4DCT with binning artifacts causing large variation in tumor delineation [2] may not represent 20-minute respiratory motion during radiotherapy, leading to sub-optimal treatments. The purpose of our study is to develop a novel multi-breath time-resolved (TR) 4DCT using the super-resolution reconstruction framework with time-resolved 4D magnetic resonance imaging (TR-4DMRI) [3-5] as guidance for patient breathing irregularity assessment.Methods
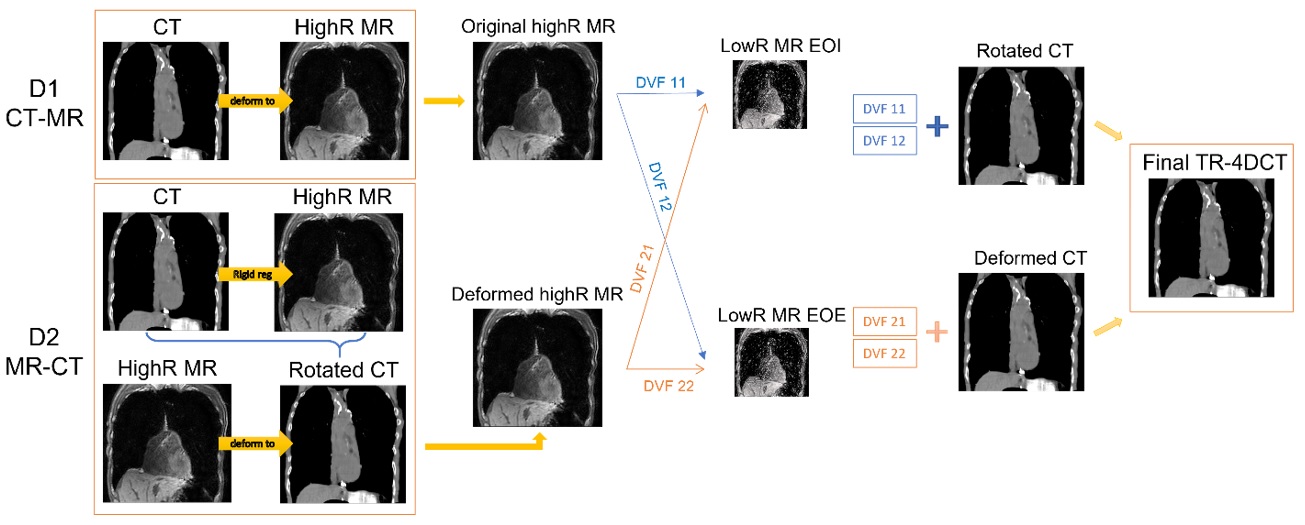
Six lung cancer patients participated in the IRB-approved protocol and scanned both MRI and CT images on the same day of patient simulation. For each patient, 80 low-resolution (lowR) (5x5x5mm3) free-breathing (FB) 3D cine MR images in 40s (2Hz) and a high-resolution (highR) (2x2x2mm3) 3D breath-hold (BH) T1w MR image were acquired in an MR session. The clinical high-resolution CT/4DCT scans were acquired within 2-3 hours from the MR session. For each patient, one highR CT image from 4DCT with minimal binning artifacts and closest diaphragm match to the highR MRI image was selected using rigid image registration. In this super-resolution approach, two deformable image registration (DIR) methods were applied in two reconstruction directions: D1: CT4D→(MRBH→MRFB) and D2: (CT4D←MRBH)→ MRFB. First, a mutual-information-based B-spline DIR was used to register highR CT to highR MR images (CT4D→MRBH or CT4D←MRBH) to establish the CT-MR voxel correspondence. Second, an intensity-based Daemon DIR was applied for MRBH→MRFB, in which the original highR MR was used in D1 while the deformed highR MR was used in D2. The deformation vector fields (DVFs) obtained from each DIR were combined to apply to the highR CT to create TR-4DCT. Figure 1 shows the workflow for both D1 and D2 reconstructions. A digital 4DCAT phantom ‘XCAT’ with 2.5mm diaphragmatic motions and three synthetic spherical to mimic tumors with diameters of 2cm, 3cm and 4cm was used to test the feasibility using the same workflow.Results
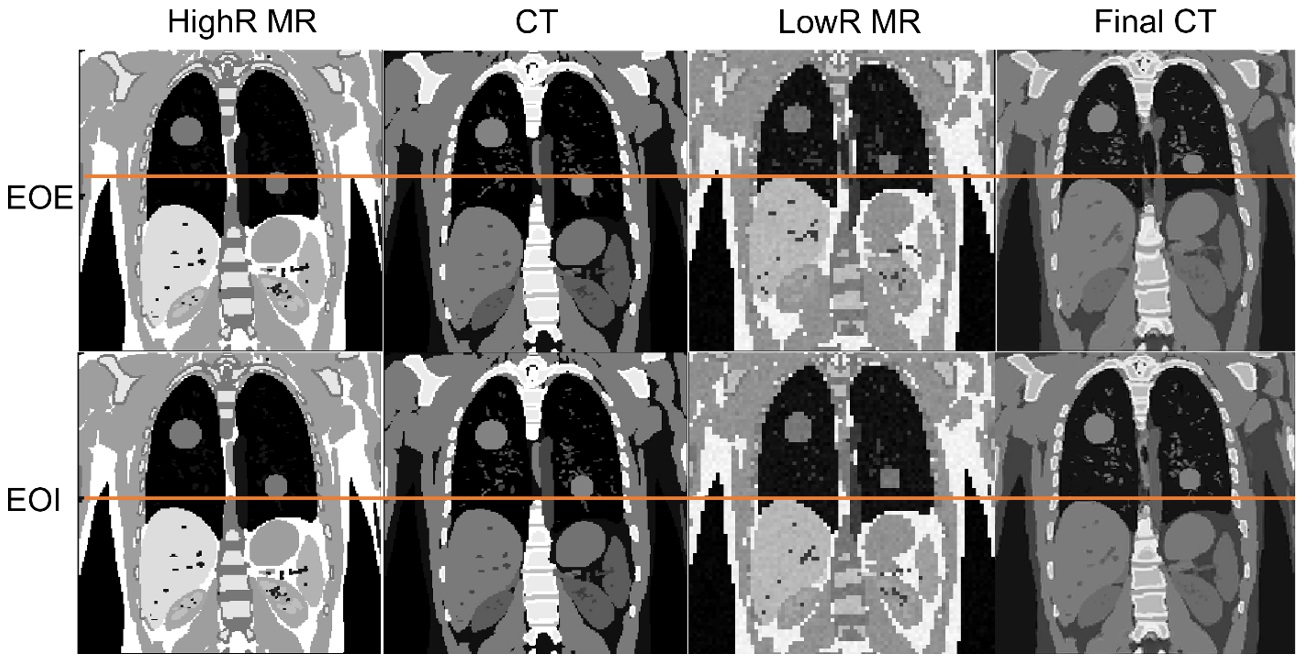
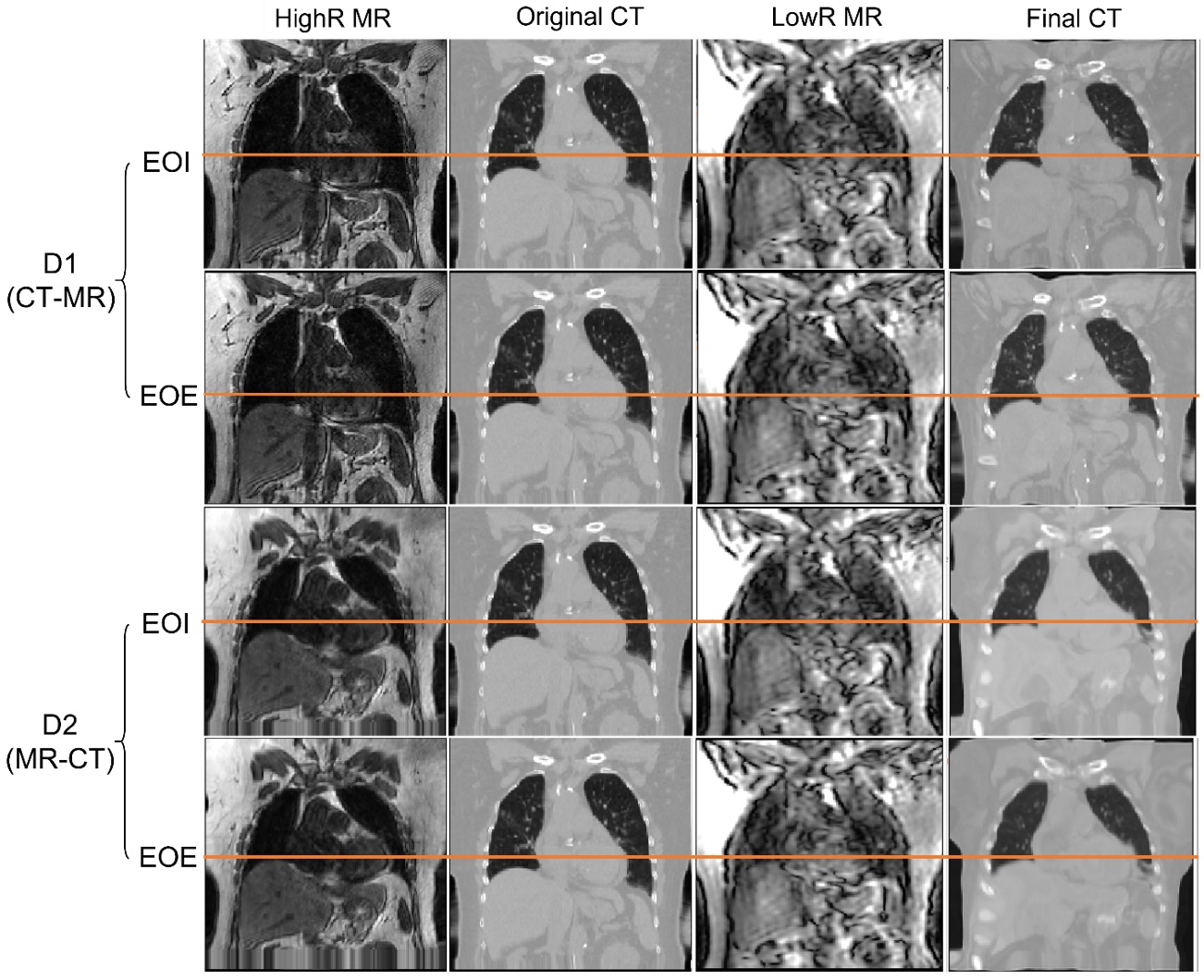
The diaphragm match is acceptable between the reconstructed TR-4DCT and 3D cine MRI for both D1 and D2. Figure 2 shows the alignment of the diaphragm between lowR MR and TR-4DCT as well as the preservation of tumor size and shape in the reconstructed TR-4DCT images of the digital phantom at the EOE and EOI. The intermediate breathing stage data are not shown. Figure 3 shows an image quality example of reconstructed TR-4DCT with Hounsfield Unit in high spatial resolution. The high temporal resolution (2Hz) is embedded in the FB data.Discussion
In this study, we extended the super-resolution framework for multi-modality DIR to reconstruct TR-4DCT images with multi-breathing cycles, without additional x-ray imaging dose. For the lung cancer patients in our study, CT image contrast has its advantage as it can well differentiate the tumor from surrounding normal lung tissues and the Hounsfield Unit is ready for dosimetry computation. Furthermore, additional advantage of this TR-4DCT technique includes that it removes binning motion artifacts on 4DCT [6-7], avoiding potential problem in respiratory gating or tumor-tracking for radiotherapy planning and delivery. Moreover, the availability of TR-4DCT without extra imaging radiation would facilitate clinical motion assessment, treatment planning, and dosimetry assessment of the plan delivery. An ongoing study focuses on further evaluation of the image quality using local voxel intensity correlation, difference in center of mass, volume ratio, dice similarity index, and mean-distance-to-agreement around the tumors, at the diaphragm on the TR-4DCT.Conclusion
Multi-breathing-cycle TR-4DCT images are reconstructed and evaluated with CT-like tumor and tissue contrasts in Hounsfield Units. Clinically, TR-4DCT has potential for breathing irregularity assessment and dosimetry evaluation in radiotherapy.Acknowledgements
This research is in part supported by the MSK Cancer Center Support Grant/Core Grant (P30 CA008748).References
[1] Dhont, J., et al. The long- and short-term variability of breathing induced tumor motion in lung and liver over the course of a radiotherapy treatment. Radiother Oncol. 126(2):339-46 (2018).
[2] Li, G., et al, A. A novel four-dimensional radiotherapy planning strategy from a tumor-tracking beam's eye view. Physics in medicine and biology. 57(22):7579-98 (2012).
[3] Li, G., et al. Novel Super-Resolution Approach to Time-Resolved Volumetric 4-Dimensional Magnetic Resonance Imaging With High Spatiotemporal Resolution for Multi-Breathing Cycle Motion Assessment. Int J Radiat Oncol Biol Phys. 98(2):454-62 (2017).
[4] Li, G., et al. Introduction of a pseudo demons force to enhance deformation range for robust reconstruction of super-resolution time-resolved 4DMRI. Med Phys. 45(11):5197-207 (2018).
[5] Nie, X., et al. Enhanced super-resolution reconstruction of T1w time-resolved 4DMRI in low-contrast tissue using 2-step hybrid deformable image registration. J Appl Clin Med Phys. 21(10):25-39 (2020).
[6] Yamamoto, T., et al. Retrospective analysis of artifacts in four-dimensional CT images of 50 abdominal and thoracic radiotherapy patients. Int J Radiat Oncol Biol Phys. 72(4):1250-8 (2008).
[7] Yuan, A., et al. A Novel Respiratory Motion Perturbation Model Adaptable to Patient Breathing Irregularities. Int J Radiat Oncol Biol Phys. 96(5):1087-96 (2016).
Figures