3086
FIRE and MATLAB for Free-Breathing Segmented LGE – A Novel Sequence and Reconstruction Approach for Selecting and Correcting Data by Respiration1Siemens Healthineers, Durham, NC, United States, 2Duke Cardiovascular MR Center, Duke University, Durham, NC, United States, 3Siemens Healthineers, Chicago, IL, United States, 4Duke Cardiovascular MR Center, Duke University Hospital, Durham, NC, United States, 5Siemens Healthineers, Princeton, NJ, United States
Synopsis
Keywords: Image Reconstruction, Motion Correction, Reordering
We introduce a free breathing segmented LGE technique combining a new acquisition, reordering and reconstruction scheme. The on-scanner reconstruction uses MATLAB and FIRE. The method produces image quality (IQ) and SNR otherwise only obtainable with breath held segmented interleaved LGE. In 27 patients, we show that IQ is superior to free breathing segmented interleaved LGE with multiple averages. SNR is higher compared to averaged motion corrected single shots when matching spatial and temporal resolution, the number of used measurements per image, and the readout type. Being a segmented technique, temporal and spatial resolution limitations of single shots do not apply.
INTRODUCTION
Patients with heart failure or reduced pulmonary function would benefit from the high image quality (IQ) of breath held (BH) segmented interleaved (SEGINT) GRE LGE [1] but frequently cannot hold their breath. Free-breathing (FB) SEGINT LGE with multiple averages usually produces nondiagnostic, blurry images with ghosting artifacts. FB averaged motion corrected (MOCO) single shots (AVGMOCO) have limited temporal or spatial resolution, poorer SNR, or reduced T1-contrast. Thus, no FB LGE sequence with similar high IQ to BH SEGINT exists. We aimed to design such a sequence and an accompanying image reconstruction (IRECON) prototyped in MATLAB (MathWorks, Natick, MA, USA) and FIRE (Framework for Image Reconstruction Environments) [2].METHODS
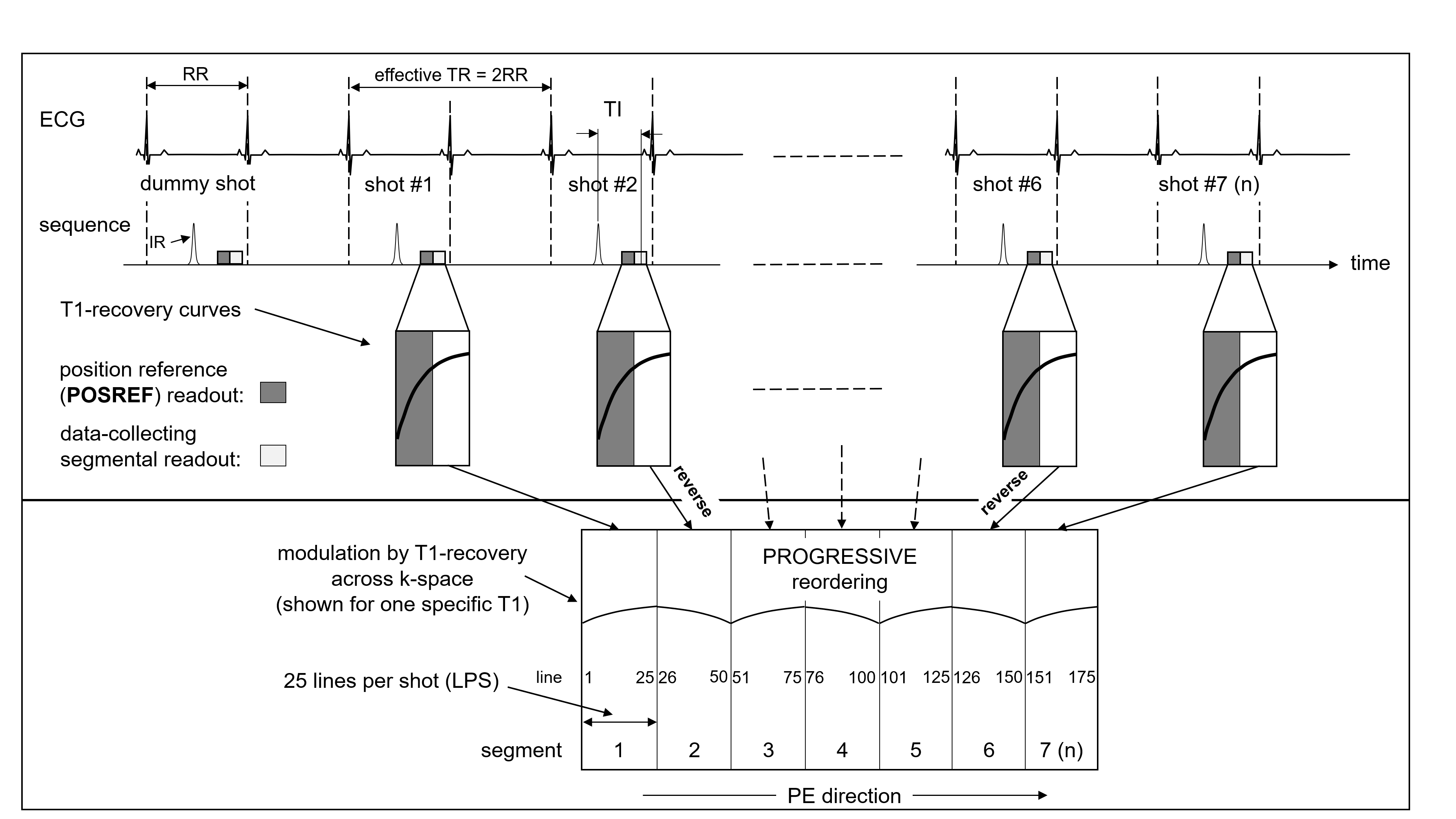
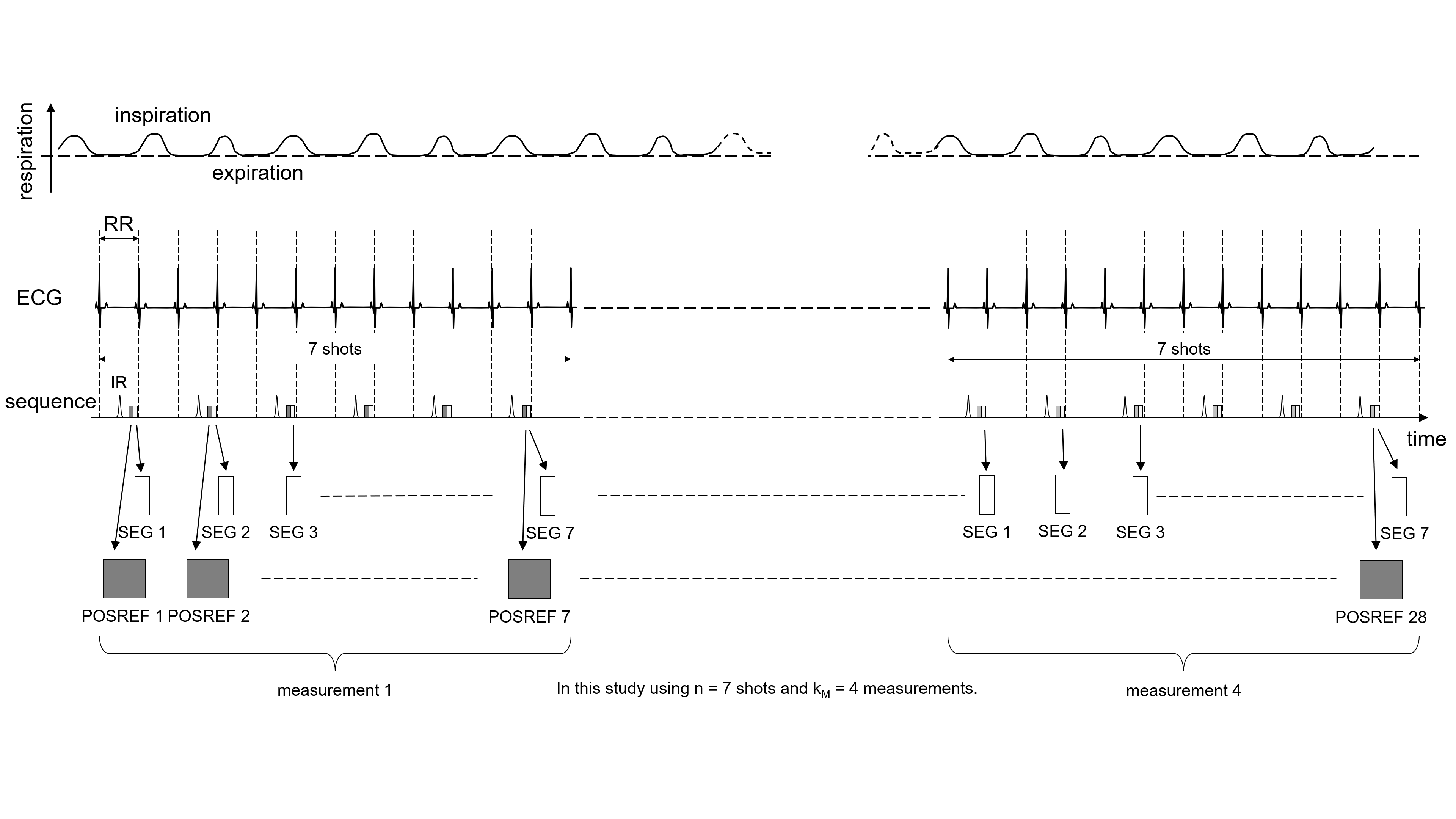
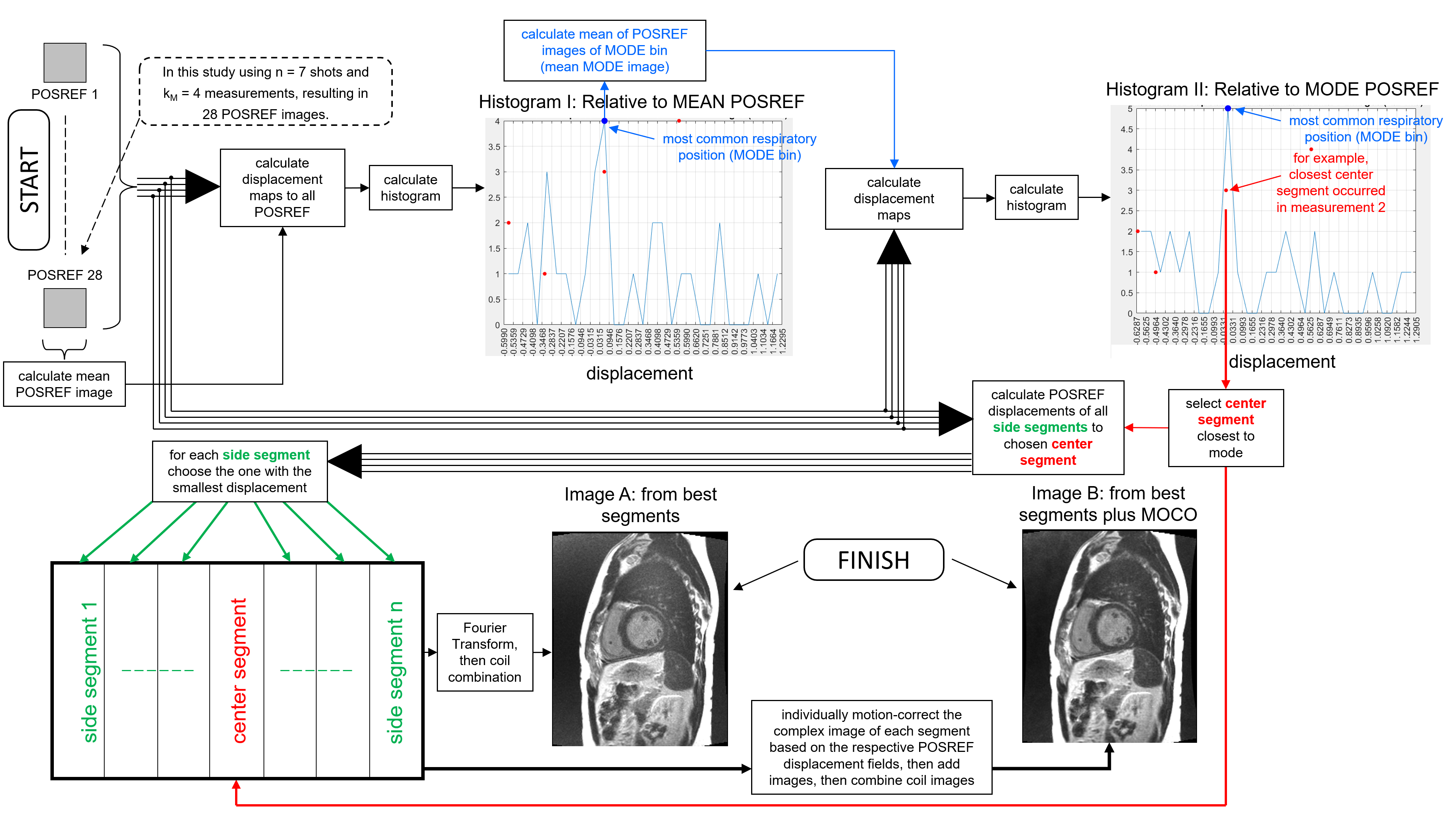
Previously developed for motion-robustness and compatibility with inversion recovery, we modified the PROGRESSIVE (Partially Reversed ReOrdering for GeneRal SupprESSion of Motion Induced Variable Errors) sequence [3] to utilize each segment’s leading magnetic conditioning to acquire position reference (POSREF) images (Figure 1). 7 segments formed one k-space and each of these was acquired four times during FB (Figure 2, 28 segments in total). IRECON assessed the respiratory phase in each of the 28 segments by its POSREF image and combined the optimally-positioned 7 segments (25 contiguous lines per segment) into an image. An optional segment-specific non-rigid MOCO [4] further enhanced IQ.In 27 patients, the segmented PROGRESSIVE LGE with IRECON (SEGPROG), the SEGINT, and the AVGMOCO GRE sequences were all run free breathing. Temporal and spatial resolution were matched along with the number of used measurements per image. IRECON was implemented in MATLAB and integrated into the FIRE works-in-progress-package (Siemens Healthineers). All image reconstructions were performed on a 3T clinical MR scanner (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany). IRECON used a non-rigid MOCO for deriving average pixel displacement of every POSREF image relative to a comparison POSREF. IRECON determined the most common respiratory phase by means of two displacement histograms (Figure 3). To create the final LGE image, Image A, IRECON assembled a full k-space using the center segment with the smallest displacement to the most common POSREF, and the side segments with POSREF images closest to the center segment’s POSREF. IRECON created a second LGE image, Image B, by “MOCOing” each complex side segment image to the POSREF of the center segment, and then adding these “MOCOed” images.
IQ (3=excellent, 2=good, 1=moderate, 0=nondiagnostic) and ghosting (GHO, 1=present, 0=absent) were scored by a blinded observer. IQ was compared by ANOVA with repeated measurements and Bonferroni correction. SNR was calculated in the blood pool and myocardium and techniques were compared similarly. The ratio of myocardium to blood SNR was assessed.
RESULTS
SEGPROG Image A IQ was better than SEGINT (2.1±0.6 vs 1.1±0.8, p<0.001), and similar to AVGMOCO IQ (2.0±0.6, p>0.05). GHO was absent in all SEGPROG and AVGMOCO but present in 61% of SEGINT images.SEGINT and PROGINT SNR were similar in blood (45.6±8.0 vs 32.2±3.6, p>0.05) and myocardium (12.9±8.0 vs 13.5±2.6, p>0.05), but lower for AVGMOCO (blood 14.1±7.1, p<0.05, myocardium 6.5±6.6, p<0.05). The myocardium to blood SNR ratio was lowest for SEGINT but similar for all techniques (SEGINT 0.3±0.2, PROGINT 0.5±0.2, AVGMOCO 0.4±0.2, p>0.05 for all).
In patient 1 (Figure 4), the SEGINT image is blurred and nondiagnostic. Severe ghosting results from the sensitivity of INT reordering to motion. The AVGMOCO image has no ghosting artifacts but low SNR. SEGPROG image A using IRECON looks like a BH image, has higher SNR than the AVGMOCO, no ghosting artifacts, and good myocardium to blood contrast. The segment based MOCO slightly improves papillary muscle sharpness (image B). The images of patient 2 tell a similar story.
DISCUSSION
This is the first description of IRECON combined with the PROGRESSIVE sequence, modified for self-navigation, together enabling FB, artifact-free, 2D segmented LGE. Combining self-navigation with INT reordering and IRECON would result in noticeable ghosting of the chest wall. Only combining IRECON with PROGRESSIVE can produce high IQ, with or without MOCO. INT, PROGRESSIVE, and single shots are the only suitable methods for sampling inversion-prepared 2D data without creating k-space modulation artifacts, and of these only PROGRESSIVE is both segmented and motion robust. Interestingly, the non-rigid MOCO applied in IRECON (image B) is possible only with PROGRESSIVE, due to its contiguous k-space coverage during each shot.While not statistically different, SEGPROG blood SNR was numerically lower than for SEGINT. This was expected since PROGSEG includes the REFPOS acquisitions that cause some signal saturation. In the future, IRECON will use more of the measured data to increase SNR, by averaging “MOCOed” segments below a displacement threshold.
In this initial implementation, the PROGSEG sequence ran four times as long (measurements=4) as AVGMOCO, because it does not use parallel imaging, whereas AVGMOCO has threefold acceleration. Adding parallel imaging will allow identification of an optimal mix of IQ, SNR, and speed.
CONCLUSION
We present a promising approach to FB, 2D segmented LGE, only possible because two recent developments, PROGRESSIVE and IRECON, work in tandem. Since it is a segmented technique, temporal and spatial resolution limitations of single shots do not apply. Our findings suggest that it will be possible to acquire images with the same quality and SNR as obtainable with BH SEGINT, but FB.Acknowledgements
No acknowledgement found.References
[1] Simonetti O, Kim R, et al. An Improved MR Imaging Technique for the Visualization of Myocardial Infarction. Radiology 2001; 218:215–223.
[2] Chow K, Kellman P, Xue H. Prototyping Image Reconstruction and Analysis with FIRE. Proc. SCMR. Virtual Scientific Sessions; 2021. p. 838972.
[3] Rehwald W, Rojas R, Mena N, Motion Robust Segmented Delayed Enhancement MRI by PROGRESSIVE (Partially Reversed ReOrdering for GeneRal SupprESSion of Motion Induced Variable Errors). Proc. Intl. Soc. Mag. Reson. Med. 30 (2022); abstract 4924.
[4] Xue H, Shah S, Greiser A, et al. Motion Correction for Myocardial T1 Mapping Using Image Registration with Synthetic Image Estimation. Magn Reson Med 67:1644–1655, 2012.
Figures
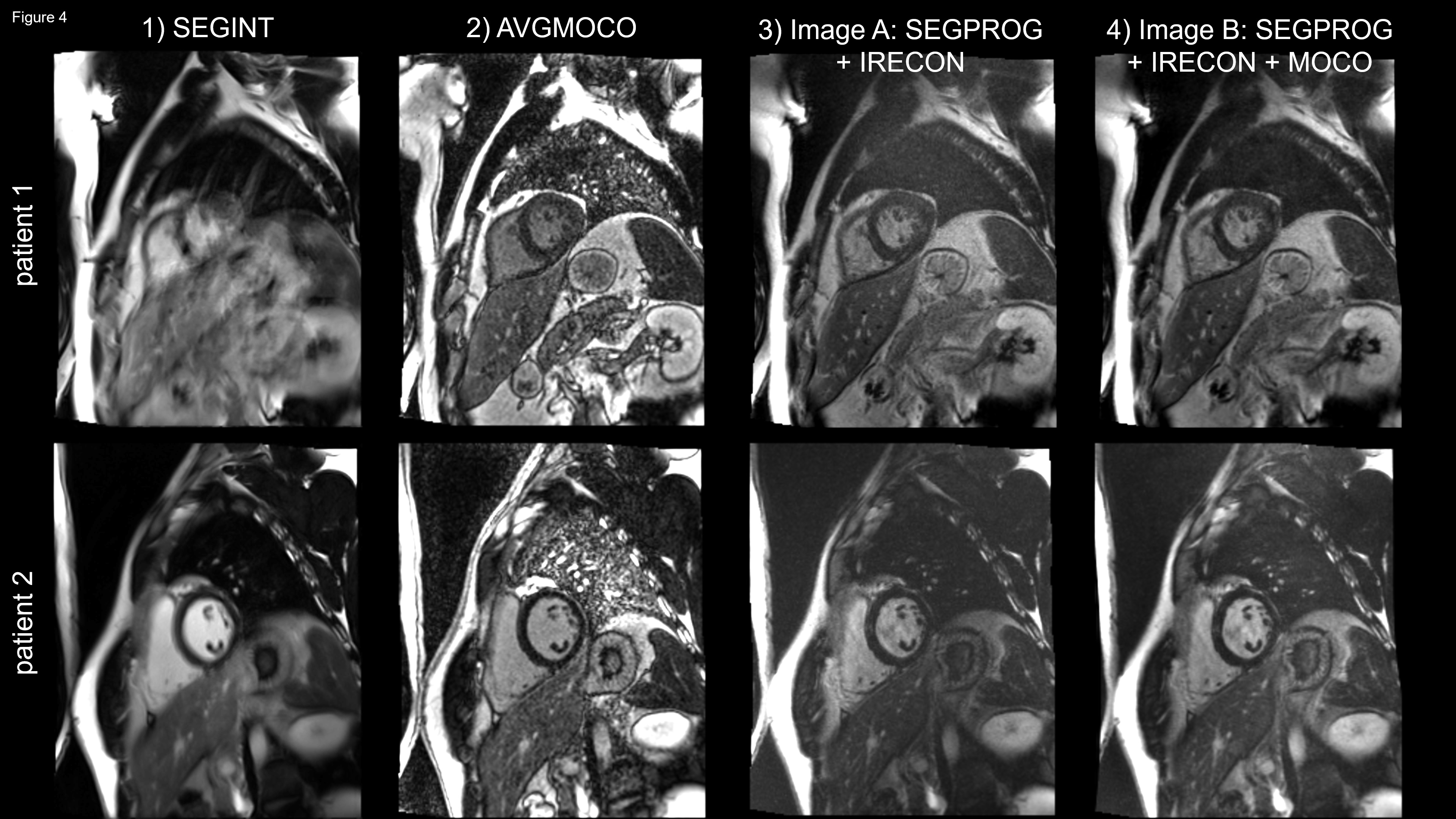
Upper row: mid-ventricular short-axis slice of a cardiac patient. 1) The SEGINT image is nondiagnostic. Breathing causes blurring and ghosting of the chest wall. 2) The AVGMOCO image has no artifacts but low SNR, due to matching spatial and temporal resolution and used shots per image to SEGPROG. 3) SEGPROG is FB but looks like a BH image, has higher IQ and SNR than AVGMOCO, no ghosting, and good myocardium to blood contrast. 4) The segment based MOCO slightly increases the sharpness of the papillary muscles.
Lower row: example similar to the above except that the SNR is higher, for all images.