3066
Association between 3D Geometry of Vertebrobasilar Arteries and Basilar Artery Atherosclerosis: An MRI Study1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, China, 2Department of Radiology, Beijing Geriatric Hospital, Beijing, China, 3Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
Synopsis
Keywords: Data Analysis, Atherosclerosis
Geometry of VBA has been proved to be associated with the presence of BA plaques, yet relative studies are lack of 3D information due to methodological difficulties. We proposed a semi-automated algorithm for quantitative measurement, which can evaluate local diameter, local curvature and angles between vessels directly in 3D space. We used the proposed algorithm to measure the 3D geometric metrics and found significant association between VBA geometry and the presence of BA plaques. Normalized diameter variation of BA and BA & PCA-R angle projected to lateral view were also associated with the presence of BA plaques independently.Purpose
It has been shown that geometric changes in vertebrobasilar arteries (VBA) may alter intravascular hemodynamics that exacerbate the initiation and progression of BA atherosclerotic plaques1. However, geometric features of VBA have been mainly measured artificially in 2D projection planes due to the lack of effective tools, which limits the acquirement of parameters containing more 3D information. Therefore, this study aims to investigate the association between 3D geometric characteristics of VBA and the presence of BA plaques.Methods
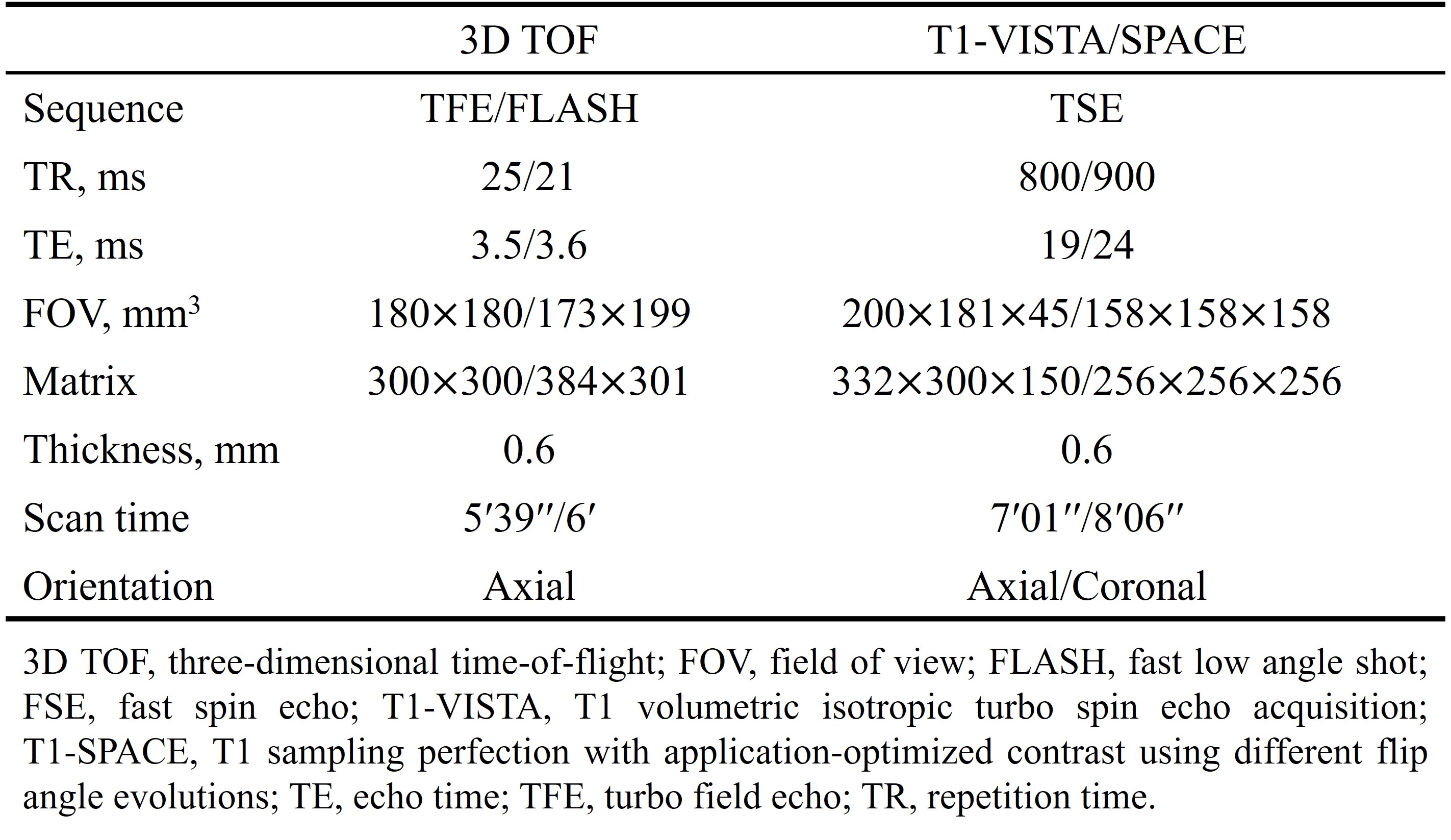
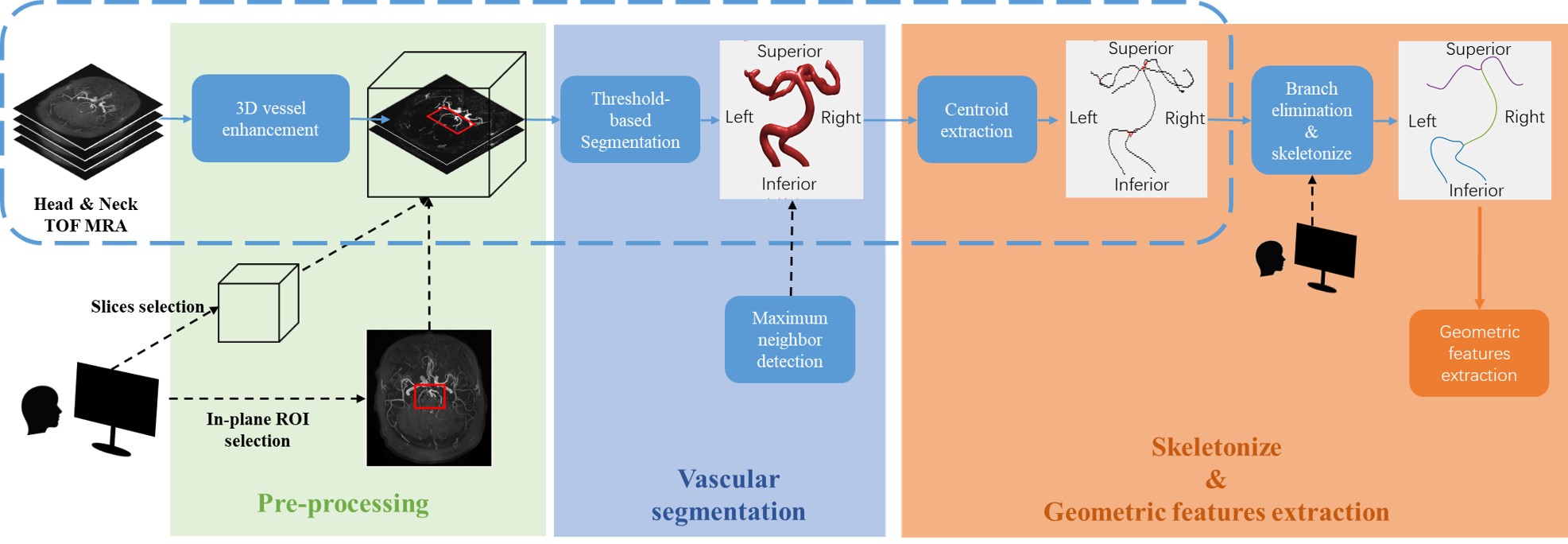
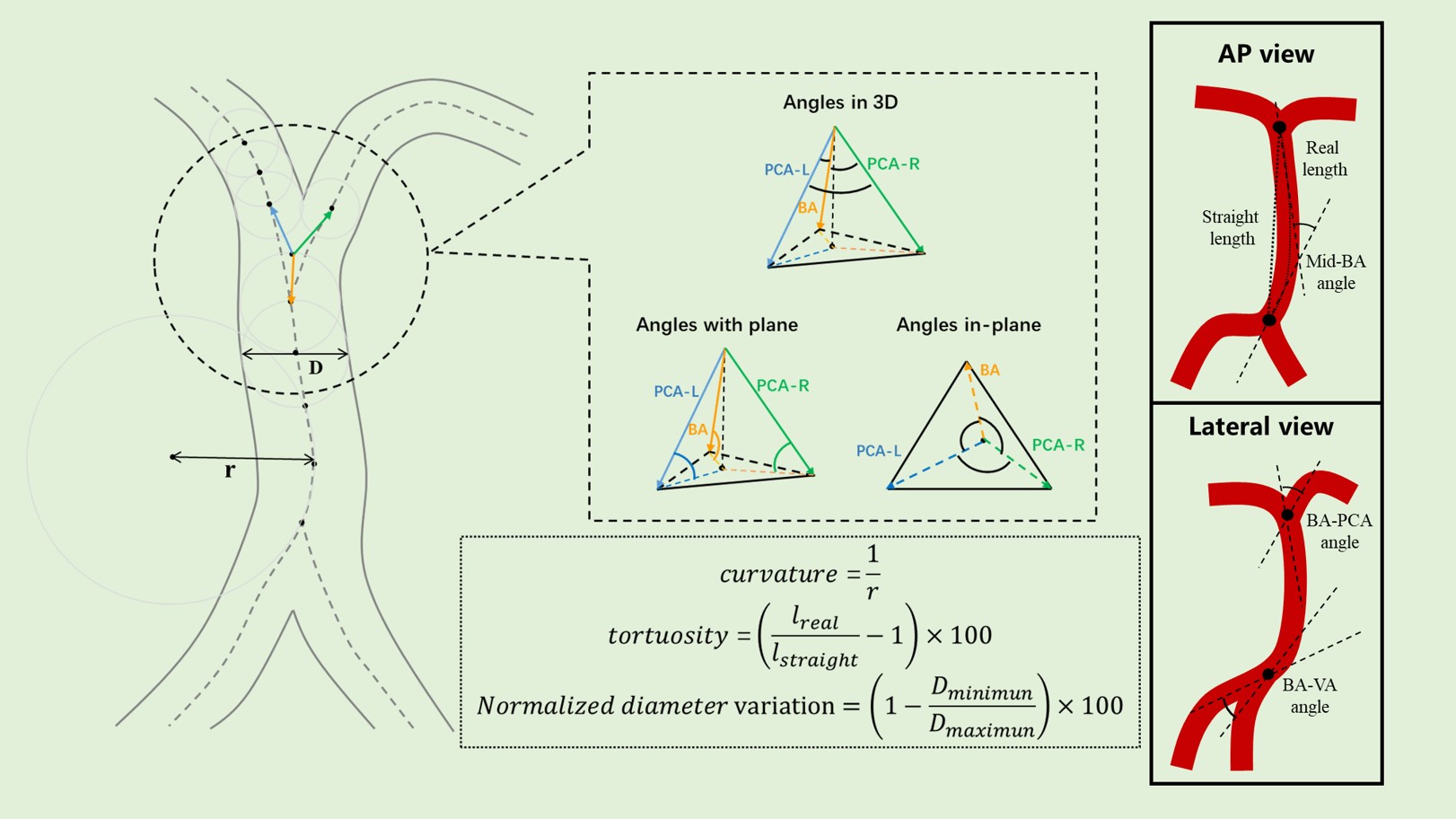
Study sample: Patients with symptomatic intracranial artery stenosis (stenosis >30%) were recruited and underwent MR angiography and vessel wall imaging for intracranial arteries. The study protocol was approved by institutional review board and written consent forms were obtained. MR imaging: The MR examinations were performed on 3.0 T Philips or Siemens MR scanners with 8-channel phase-array head coil or 16-channel neurovascular coil. The imaging protocol included 3D TOF MRA as well as T1-VISTA/SPACE and the MR imaging parameters are presented in Table 1. Image analysis: A semi-automated segmentation and geometric extraction algorithm based on 3D TOF MRA was proposed to quantitatively evaluate VBA geometry (Figure 1)2-5. When evaluating VBA geometry, local lumen diameter and curvature and normalized diameter variation were taken into account. VBA angles were also measured automatically, including those in 3D space and their projections in 2D planes (in both lateral view and anteroposterior view) (Figure 2). BA plaques were identified by experienced radiologists with >5 years’ experience in neurovascular imaging. Statistics: All quantitative geometric parameters calculated by the proposed algorithm were compared between patients with and without BA plaques using independent samples t-test or Mann-Whitney U test. Univariable and multivariable logistical progressions were also applied to determine the association between geometric features and presence of BA plaques.Results
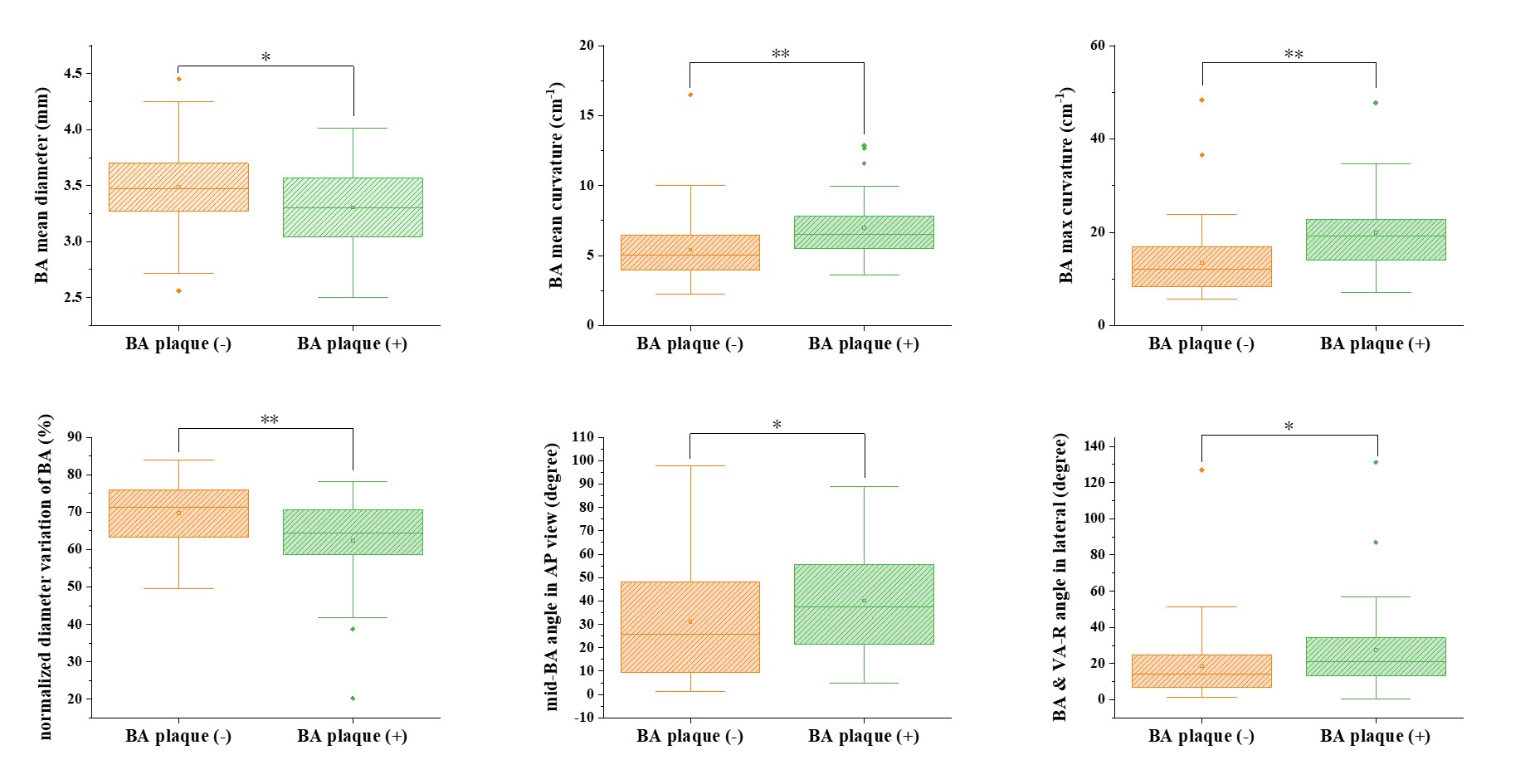
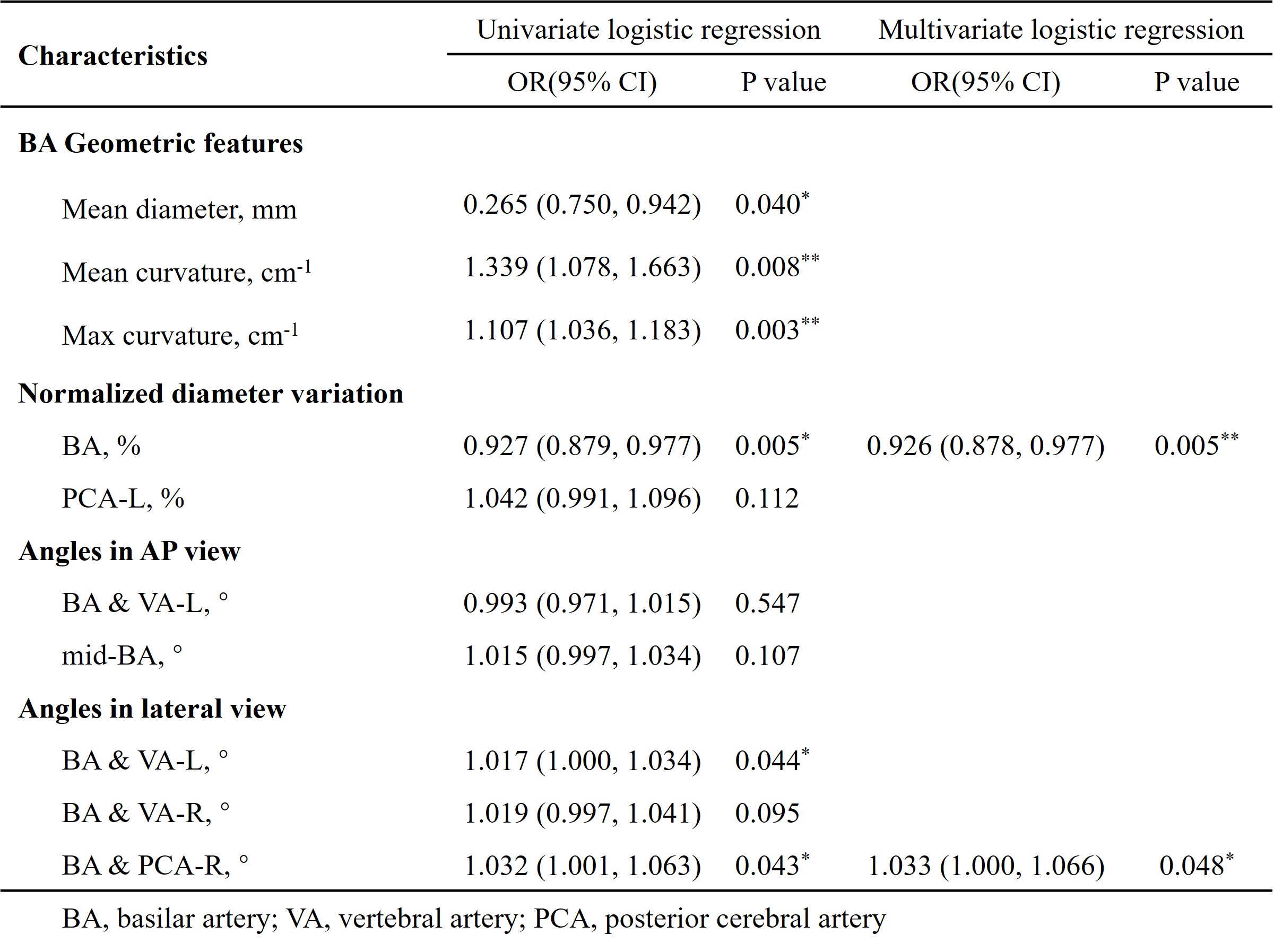
Of the 88 recruited patients (mean age: 57 ± 12.15 years; 44 males), 29 (33.0%) had BA plaques. Patients with BA plaques showed significantly smaller mean lumen diameter (3.30 ± 0.36 mm vs. 3.48 ± 0.38 mm, P = 0.036), larger mean curvature (7.00 ± 2.45 cm-1 vs. 5.42 ± 2.21 cm-1, P = 0.001), larger max curvature (19.96 ± 9.04 cm-1 vs. 13.45 ± 7.25 cm-1, P < 0.001), smaller normalized diameter variation (62.37 ± 12.50 % vs. 69.70 ± 8.26 %, P = 0.007) of BA, as well as a larger mid-BA angle from the AP view (40.14° ± 22.98° vs. 31.04° ± 25.06°, P = 0.049) and a larger BA &VA-R angle from the lateral view (27.64° ± 26.51° vs. 18.58° ± 18.88°, P = 0.037). Variables with P<0.15 in univariable logistic regression were summarized in Table 2. After removing max curvature of BA (collinear with mean curvature of BA), all features were utilized as input in multivariable logistic regression with forward: LR method. The normalized diameter variation of BA (OR = 0.926; 95%CI [0.878, 0.977], P = 0.005) and the BA & PCA-R angle from the lateral view (OR = 1.032; 95%CI [1.001, 1.063], P = 0.048) remained significant association with presence of BA plaques in multivariable logistic regression analysis.Discussion & Conclusion
This study demonstrated that geometric features of VBA measured automatically on 3D TOF MRA show significant association with the presence of BA plaques. The normalized diameter variation of BA and the BA & PCA-R angle measured in the lateral view are independently associated with presence of BA plaques. It can be inferred that the geometric characteristics in VBA may influence the local hemodynamics like wall shear stress (WSS) and thus increase the probability of the formation of BA. However, the angles measured directly in 3D space didn’t show significant association with the presence of BA plaques. In future, we plan to include more patients and make a more comprehensive analysis.Acknowledgements
No acknowledgement found.References
1. Deng S, Zheng J, Wu Y, et al. Geometrical characteristics associated with atherosclerotic disease in the basilar artery: a magnetic resonance vessel wall imaging study. Quant Imaging Med Surg. 2021;11(6):2711-2720.
2. Jerman T, Pernus F, Likar B, et al. Enhancement of Vascular Structures in 3D and 2D Angiographic Images. IEEE Trans Med Imaging. 2016;35(9):2107-2118.
3. Li C, Xu C, Gui C, Fox MD. Distance regularized level set evolution and its application to image segmentation. IEEE Trans Image Process. 2010;19(12):3243-54.
4. Lee T, Kashyap R. Building Skeleton Models via 3-D Medial Surface/Axis Thinning Algorithms. CVGIP: Graphical Models and Image Processing. 1994;56(6):462-478.
5. Deshpande A, Jamilpour N, Jiang B, et al. Automatic segmentation, feature extraction and comparison of healthy and stroke cerebral vasculature. Neuroimage Clin. 2021;30:102573.
Figures