3064
Normal left ventricular flow dynamics in a paediatric population assessed by 4D Flow MRI
Fraser Maurice Callaghan1,2, Barbara Burkhardt2,3, Julia Geiger2,4, Emanuela Valsangiacomo Buechel2,3, and Christian Kellenberger2,4
1University Children's Hospital Zurich, Zurich, Switzerland, 2Children’s Research Center, University Children's Hospital Zurich, Zurich, Switzerland, 3Division of Pediatric Cardiology, University Children's Hospital Zurich, Zurich, Switzerland, 4Department of Diagnostic Imaging, University Children's Hospital Zurich, Zurich, Switzerland
1University Children's Hospital Zurich, Zurich, Switzerland, 2Children’s Research Center, University Children's Hospital Zurich, Zurich, Switzerland, 3Division of Pediatric Cardiology, University Children's Hospital Zurich, Zurich, Switzerland, 4Department of Diagnostic Imaging, University Children's Hospital Zurich, Zurich, Switzerland
Synopsis
Keywords: Data Analysis, Cardiovascular, 4D flow
4D flow MRI provides a rich dataset that can make analysis challenging. A new technique of left ventricle (LV) registration is presented and compared with established techniques for analysis of flow dynamics in a normal paediatric population. Averaging of group flow dynamics in a common space permits additional analysis, complementary to established techniques.
Our technique demonstrated flow dynamics on a common LV space and identified subtle differences in LV velocities between normal male and female subjects of a paediatric population.
This represents a new tool in 4D flow data analysis for potential biomarker development.
INTRODUCTION
4D flow MRI has proven to be a valuable tool for providing new insights and greater detail in the hemodynamics and flow efficiencies of the heart and great vessels 1,2. Normal population statistics of these advanced parameters have been generated permitting the possibility for the discovery of new imaging and hemodynamic biomarkers for cardiovascular disease 3,4.A common method of normalisation of ventricular parameters for group analysis is classification of ventricular flow components into direct flow (DF), delayed ejection (DE), retained inflow (RI) and residual volume (RV) parts depending on their relative cardiac cycle of inflow and ejection 5. This technique has given promising results for comparison of subject groups 6,7. In separate studies, 4D flow datasets have been able to display subtle ventricular differences showing its potential for biomarker development 8,9.
This work develops a new technique for registration and normalisation of left ventricle (LV) flow dynamics permitting group analysis in a common LV space. We investigate and compare sex differences using the traditional flow classification technique and using our spatial classification technique in a cohort of normal paediatric subjects.
METHODS
From subjects that had received cardiac MRI at our institution over a period of April 2018 to September 2022 we selected subjects clinically classified to have normal structural and functional heart anatomy. Selection criteria was 4D-flow MRI with full coverage of the heart and informed consent (provided by a guardian in cases of young subjects).MRI examinations were performed on a GE 1.5T Discovery, or SIGNA Artist scanner. Spatial resolution was 1.4±0.1 mm in-plane, slice thickness 2.1±0.1 mm. Mean temporal resolution was 32.4±6.9 ms (20-25 phases per cardiac cycle). A k-t acceleration parallel imaging technique (kat-ARC=8) was employed.
The LV of all subjects were segmented from the 4D flow data and pathline tracking was performed and classified into components DF, DE, RI and RV. Separately, all LVs were registered to a single left ventricular space via diffeomorphic transformation and the resultant transformation field was applied to the pathlines for assessment in a common space. The common LV space was discretized into three longitudinal sections labelled: base, middle and apex, permitting spatial analysis of hemodynamics.
Pathlines were discretized into 20 time points covering a normalised cardiac cycle and mean velocity was compared using independent t-test between groups both by flow component classification and by spatial classification.
RESULTS
The normal group consisted of 33 individuals aged 3-20 years (mean± standard deviation 14±3.8), 20 (60%) were males.Transformation of all datasets to a single LV space was inspected manually for all cases and accurate registration and transformation was confirmed. Mean flow from all subjects through the common LV showed expected hemodynamics of the RV component being formed from flow driven towards the apex during LV filling and the RI component formed from LV filling on the free ventricle wall side and circulating towards the apex, while the base of the ventricle was predominantly occupied by the DF component at end diastole (Figure 1).
Total fractions of DF, DE, RI, RV within the LV of normal subjects at end diastole showed no correlation with age, cardiac output, and ejection fraction (R<0.3). Mean ( ± standard deviation) values were DF: 42.9±9.5%, DE: 31.4±6.7%, RI: 10.0±3.3% and RV: 10.6±4.7%. LV end diastolic volume (LVEDV) (indexed by body surface area) ranged from 53.1 to 113.3 mL/m2 (81.6±16.6 mL/m2). There was a medium correlation with LVEDV: DF: -0.45, DE: 0.37, RI: -0.13, RV: 0.2.
The technique of ventricular flow component classification showed a significantly lower velocity for female subjects compared to males for the DF, DE and RI flow components during late systolic ejection. Using spatial classification of hemodynamics, significantly lower velocities for females compared to males during late systolic ejection was observed in both the base and middle LV sections.
DISCUSSION
We have established a technique for reliable transformation of LV flow dynamics to a common space for 4D flow assessment. This was combined with LV flow component classification to illustrate normal flow passage through the LV.Comparison of the techniques of flow component classification and spatial classification in a common space showed that both techniques identified differences between male and female subjects in a normal paediatric population. The techniques can be considered as complimentary, as the spatial identification of differences in the middle and base sections of the LV agrees with differences in DF, DE and RI flow components, noting that the RV flow component is often observed to reside in the apex of the LV. Normal values for DF and DE were larger than those reported in a healthy adult population, with the difference compensated by reduced RV4. LVEDV values were similar to those reported in literature10 and we presented a trend for decreasing DF with increasing LVEDV.
CONCLUSION
We established a technique for comparison of subjects' and subject groups' 4D flow data in a common space. This provides many opportunities for detailed analysis of spatial hemodynamics and potential biomarker development, complimentary to already established techniques such as flow component analysis. Our technique showed agreement with established methods, is simple to implement and relies only on the 4D flow dataset.Acknowledgements
No acknowledgement found.References
Figures
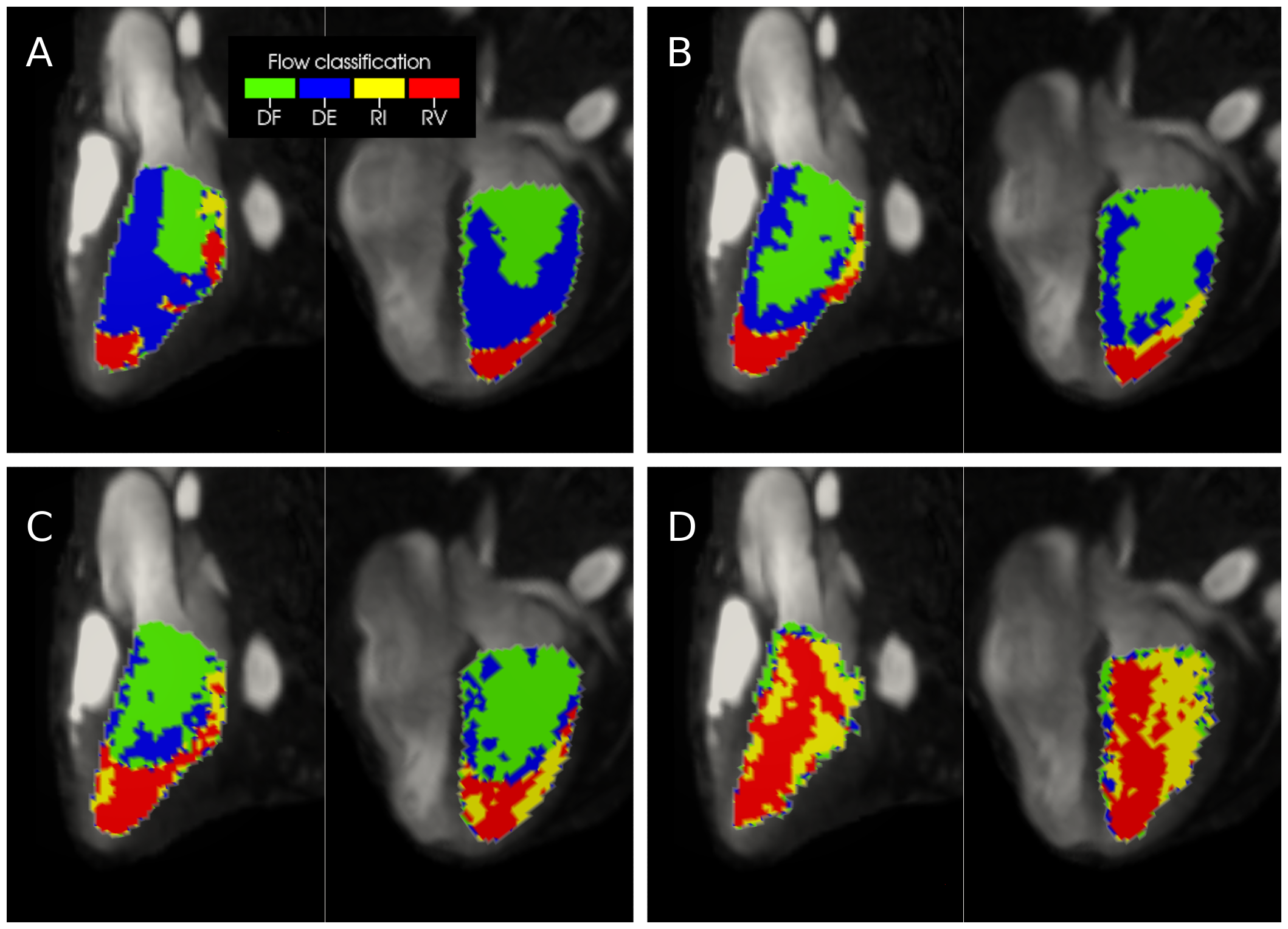
Figure 1. Phases showing (A) early LV filling, (B) mid LV filling, (C) early LV ejection and (D) late LV ejection of an averaged classification of LV flow dynamics in 33 subjects registered to a common LV space overlaid on LV 2-chamber (left) and 4-chamber views. DF=direct flow, DE=delayed ejection, RI=retained inflow, RV=residual volume.
DOI: https://doi.org/10.58530/2023/3064