3034
White matter abnormalities in pediatric idiopathic growth hormone deficiency: A DTI study using TBSS analysis1Department of Radiology, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: White Matter, Diffusion Tensor Imaging, Idiopathic growth hormone deficiency, TBSS
Idiopathic growth hormone deficiency (IGHD) is an important and unknown causes of pediatric short stature. Although grey matter morphological changes in the cerebral cortex of IGHD have been proved, the knowledge about white matter (WM) is poorly investigated. Whether the mental status of IGHD children is associated with WM abnormalities is unclear. In this study, 50 pediatric with IGHD and 48 age- and gender-matched typically developing (TD) children included for TBSS analysis. Our results indicated that IGHD children showed the WM abnormalities (especially in bilateral posterior corona radiata), which are correlated with behavioral and mental problems.Introduction
Growth hormone deficiency (GHD) is a rare but important cause of short stature, classified as idiopathic and organic GHD. Idiopathic GHD (IGHD) was inadequate growth hormone (GH) within unknown causes1. Growth hormone-insulin-like growth factor-l axis (GH-IGF-1) is involved extensively in neurogenesis and brain development2. Previous studies have proved that children with IGHD have significant morphological changes in the cerebral cortex 3, 4 which probably indicate other more essential changes, such as white matter (WM). Furthermore, IGHD children always showed emotional problems which can be improved when GH is replaced, since there is an association between the somatotropic axis and mental disorders, especially affective disorders5. However, there is no consensus exists the mental status of IGHD children is associated with abnormalities of brain WM structure. In this study, we used diffusion tensor imaging (DTI) and tract-based spatial statistics (TBSS) to investigate white matter (WM) changes in pediatric IGHD and explain the potential cause of the mental status.Methods
Fifty pediatric clinical diagnosis of IGHD (mean age: 8.560 ± 2.98 yr) and 48 age- and gender-matched typically developing (TD) children (mean age: 8.979 ± 2.41 yr) were included. IGHD children were assessed for behavioral and mental problems using the Achenbach's Child Behavior Cheeklist (CBCL), reported by parents. DTI and TBSS analyses were performed to evaluate WM alternations, and the statistical maps were processed at the cluster level with threshold-free cluster enhancement (TFCE). For all tests, a P-value < 0.05 was considered statistically significant. What's more, partial correlation analyses were performed to identify the relationship between clinical characteristics and DTI parameters, considered age and sex of each subject as covariates.Results
In the TBSS analysis, the IGHD group showed increased fractional anisotropy (FA) values (mainly in bilateral posterior corona radiata) and increased axial diffusivity (AD) values (mainly in 3 fibers: right retrolenticular part of internal capsule and bilateral posterior corona radiata) (P < 0.05, TFCE corrected) (Table 1, Fig. 1). However, there were no significant differences in RD and MD values. Total score of CBCL were positively associated with FA values in the cluster of left posterior corona radiata (r=0.351 P=0.014) (Fig. 2).Discussion
In this investigation, we used DTI parameters combined with TBSS method to investigate WM abnormalities in pediatric IGHD.Firstly, relative to the TD group, FA values of bilateral posterior corona radiata were significantly increased. Furthermore, FA values of left posterior corona radiata was positively associated with the severity of the total score of CBCL in IGHD children. Recent studies have identified pathological increases in FA in many mental disorders, for example, ADHD, schizophrenia6, as well as obsessive-compulsive disorder7. Hyperconnectivity expressed by high FA may be diminished axonal branching and/or increased axonal packing8, which may drive the difficulties in regulating emotions. We speculate that increased FA values may reflect more redundant organization of WM microstructure or delay of WM development strategy, and may cause more severe behavioral and mental problems underlying IGHD.
Secondly, AD measures diffusion of water parallel to axons which primarily show axonal status, and the axonal pruning process causes a decrease in AD9, 10. In IGHD children, the AD values of the right retrolenticular part of internal capsule and bilateral posterior corona radiata were also increased, which probably related to a decrease or delay in the myelination process and the normal pruning process.
In conclusion, our findings suggest that WM alternations in IGHD may be more related to increased redundant organization caused by delay in the pruning process.
Conclusion
Our results indicated that children with IGHD showed the WM abnormalities, especially in bilateral posterior corona radiata. Furthermore, the WM abnormalities are correlated with behavioral and mental problems, providing evidence of potential pathophysiologic mechanisms accounting for the behavioral and mental abnormalities in IGHD children.Acknowledgements
None.References
1. Lindsay, R., et al., Utah Growth Study: growth standards and the prevalence of growth hormone deficiency. J Pediatr, 1994. 125(1): p. 29-35.2. Aberg, D., Role of the growth hormone/insulin-like growth factor 1 axis in neurogenesis. Endocr Dev, 2010. 17: p. 63-76.
3. Zhang, Z., et al., Morphological changes of the cerebral cortex between children with isolated growth hormone deficiency and idiopathic short stature. Brain Res, 2020. 1748: p. 147081.
4. Zhang, Z., et al., Morphological changes in the central sulcus of children with isolated growth hormone deficiency versus idiopathic short stature. Dev Neurobiol, 2021. 81(1): p. 36-46.
5. Karachaliou, F.H., et al., Association of growth hormone deficiency (GHD) with anxiety and depression: experimental data and evidence from GHD children and adolescents. Hormones (Athens), 2021. 20(4): p. 679-689.
6. Peterson, D.J., et al., Increased regional fractional anisotropy in highly screened attention-deficit hyperactivity disorder (ADHD). J Child Neurol, 2011. 26(10): p. 1296-302.
7. Hartmann, T., et al., Increased fractional anisotropy in cerebellum in obsessive-compulsive disorder. Acta Neuropsychiatr, 2016. 28(3): p. 141-8.
8. Li, Q., et al., Increased fractional anisotropy in white matter of the right frontal region in children with attention-deficit/hyperactivity disorder: a diffusion tensor imaging study. Neuro Endocrinol Lett, 2010. 31(6): p. 747-53.
9. Song, S.K., et al., Demyelination increases radial diffusivity in corpus callosum of mouse brain. Neuroimage, 2005. 26(1): p. 132-40.
10. Bockhorst, K.H., et al., Early postnatal development of rat brain: in vivo diffusion tensor imaging. J Neurosci Res, 2008. 86(7): p. 1520-8.
Figures
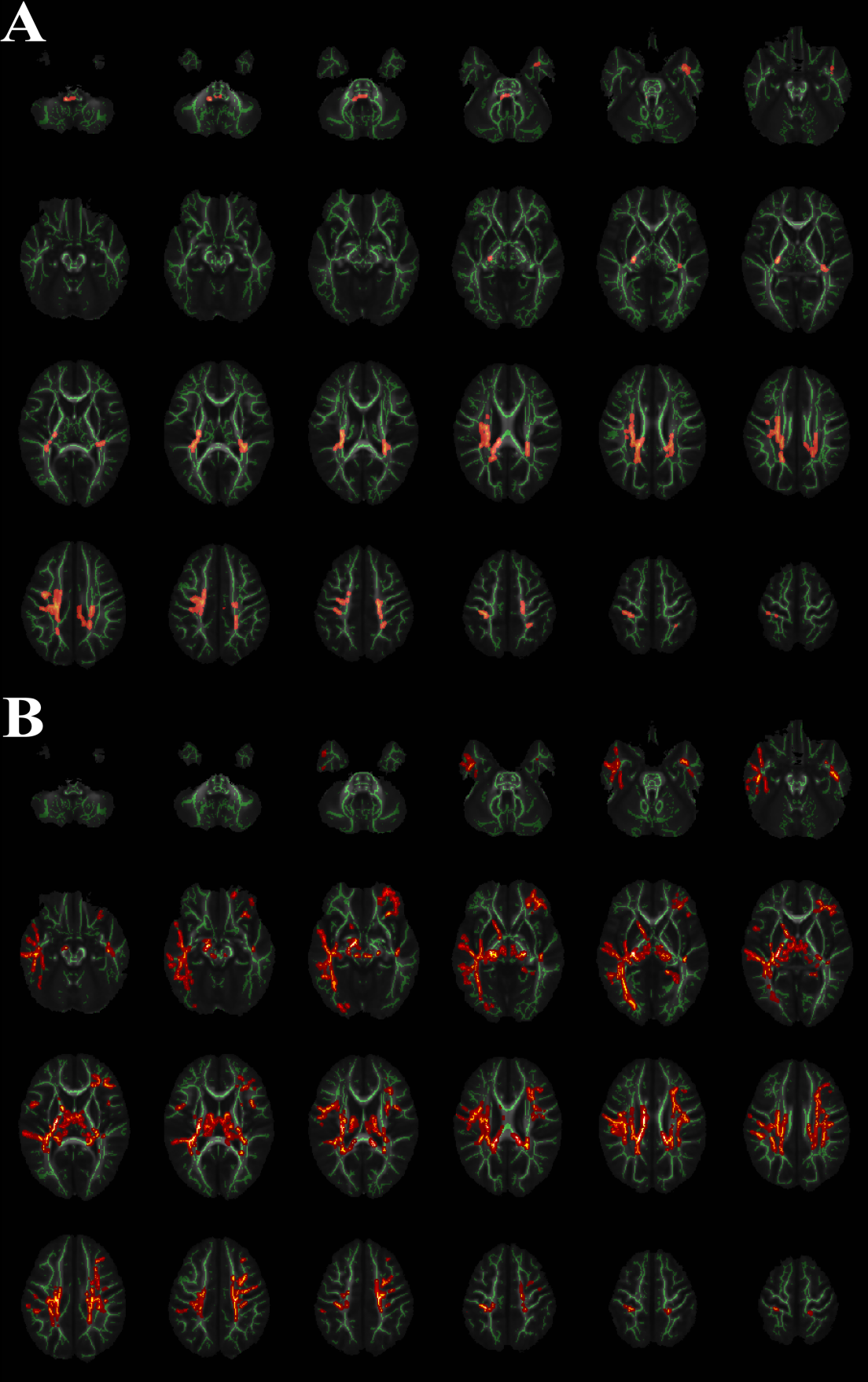
Figure 1.White Matter regions with significant increasing FA and AD values in IGHD group versus the TD group
Areas in red are regions where FA (Panel A) and AD (Panel B) were significantly higher (P<0.05, corrected by TFCE) in IGHD group relative to TD group. To aid visualization, regions showing increased FA/AD (red) are thickened using the tbss_fill script implemented in FSL. The left side of the image corresponds to the right hemisphere of the brain.
*IGHD = Idiopathic growth hormone deficiency; TD = typically developing; FA = Fractional Anisotropy; AD = Axial Diffusivity
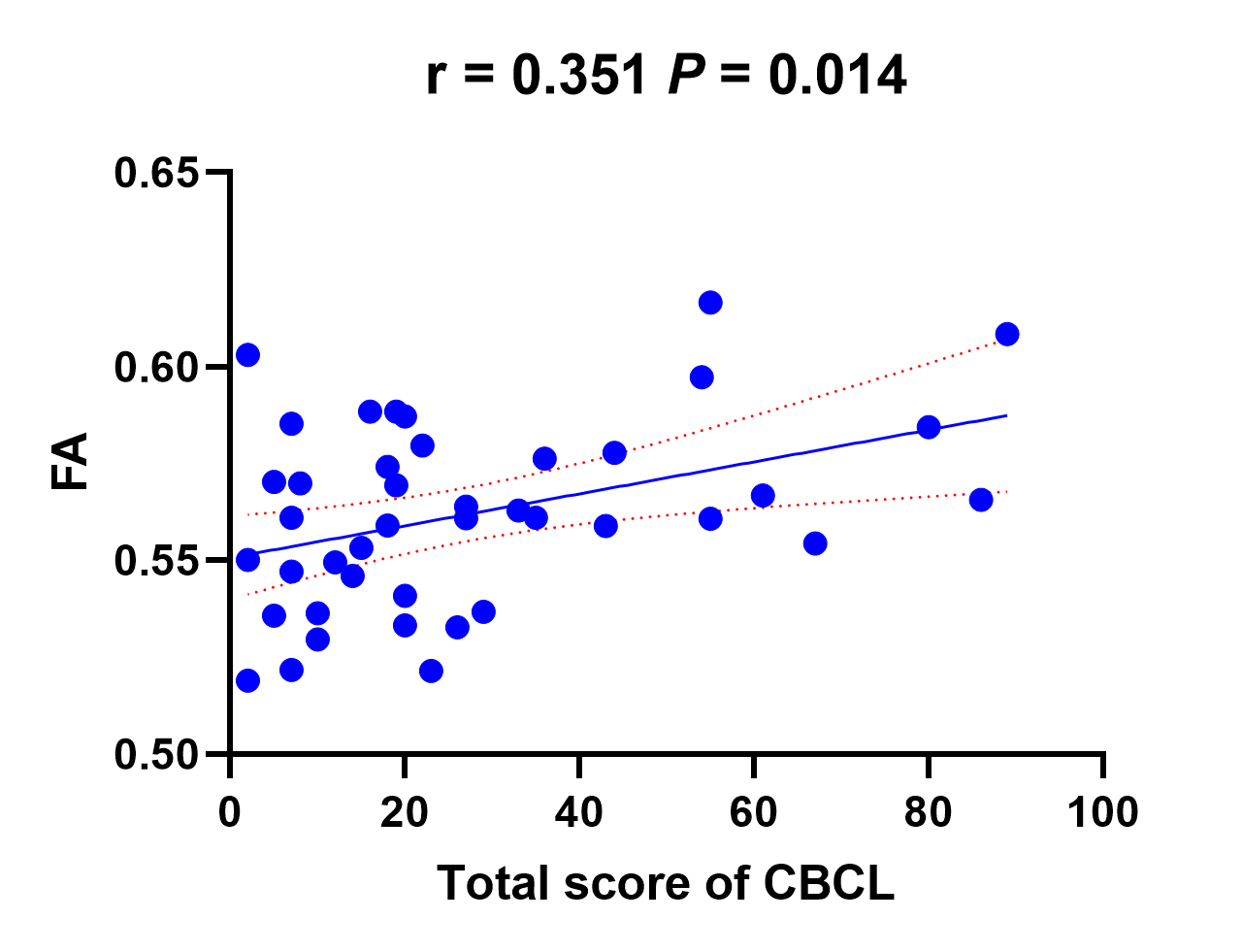
Figure 2. Scatterplot of total score of CBCL against FA values of left posterior corona radiata in the Idiopathic growth hormone deficiency (IGHD) patients
*IGHD = Idiopathic growth hormone deficiency; TD = typically developing; FA = Fractional Anisotropy; AD = Axial Diffusivity; CBCL = Achenbach's Child Behavior Cheeklist
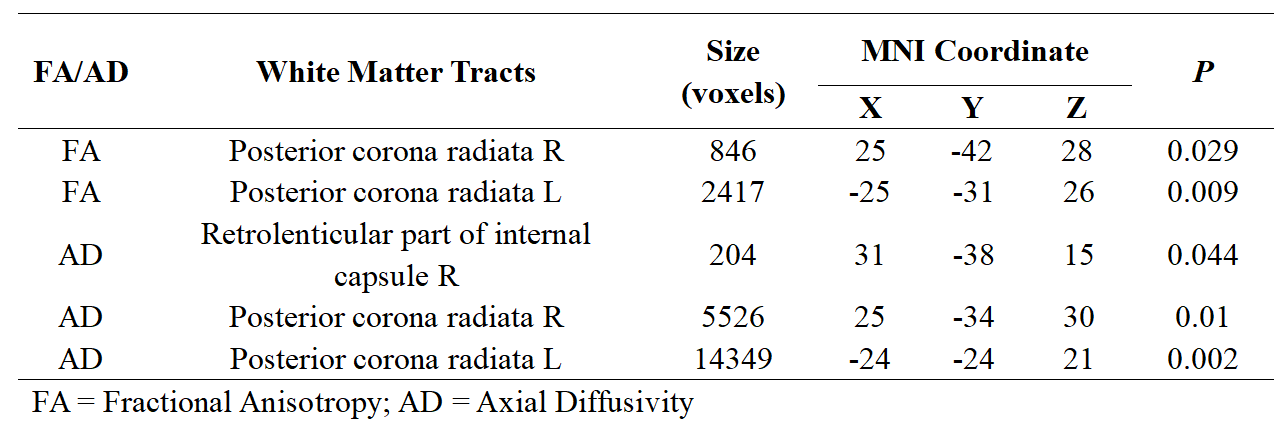
Table 1. Increased FA and AD values in comparisons between the Idiopathic growth hormone deficiency(IGHD) group and typically developing(TD)-group for TBSS analysis
*FA = Fractional Anisotropy; AD = Axial Diffusivity