2972
IVIM helps accurately diagnose PAS by showing the basal plate of placenta1First Affiliated Hospital of Xi'an Jiaotong University, Xi'an, China
Synopsis
Keywords: Placenta, Placenta
Placenta accreta spectrum (PAS) is a serious threat to maternal life, but ultrasound and conventional MRI have limitations in the diagnosis of PAS. Intravoxel incoherent motion (IVIM) is a technique of diffusion weighted MR imaging, which allows separation of tissue diffusivity and perfusion information based on the signal intensity at varying degrees of b values. We found that IVIM was able to diagnose PAS by showing the basal plate of placenta, the structure dividing the placenta and the uterus. This new finding could improve the diagnostic efficacy of MRI in the diagnosis of PAS.Introduction
Placenta accreta spectrum (PAS) is a serious threat to maternal life, as the placental villi invade the myometrium, the placenta cannot be separated from the uterus during delivery causing heavy bleeding1-3. Preoperative imaging diagnosis of PAS is very important, but ultrasound and conventional MRI have limitations in the diagnosis of PAS4,5. Ultrasound is susceptible to amniotic fluid and abdominal wall fat. Conventional MRI can compensate for these deficiencies to some extent though. However, in late pregnancy, the myometrium is so thin that conventional MRI cannot show whether the placenta is demarcated from the myometrium1. Intravoxel incoherent motion (IVIM) is a technique of diffusion weighted MR imaging, which allows separation of tissue diffusivity and perfusion information based on the signal intensity at varying degrees of b values6-9. IVIM has been found to detect the difference between PAS and normal placenta. Based on these studies, we found that IVIM was able to diagnose PAS by showing the basal plate of placenta, the structure dividing the placenta and the uterus.Materials and Methods
This study was approved by ethical committee of First Affiliated Hospital of Xi’an Jiaotong University. Written parental informed consent was obtained for all pregnant women. 68 pregnant women were recruited in First Affiliated Hospital of Xi’an Jiaotong University. No sedatives were used for MRI. The scanning was stopped immediately once the pregnant woman has chest discomfort or other discomfort. Placental MR examination for each gestational woman was performed on a 3T MRI system (GE Healthcare, Milwaukee, Wisconsin) with an 8-channel body flex coil. Single shot fast spin echo (SSFE) T2-weighted images were acquired using: TR minimum; TE 85 ms, matrix 228×256, FOV 36mm, section-thickness 4 mm without gap. Intra Voxel Incoherent Motion (IVIM) images were collected with each of the following b values: 0, 20, 50, 80, 100, 150, 200, 400, 600, 800sec/mm2. The scanning parameters were as follows: TR 2000ms; TE 63 ms, matrix 128×128, FOV 38mm, section-thickness 4mm with 1mm gap. A total examination time was less than 10 min.Results
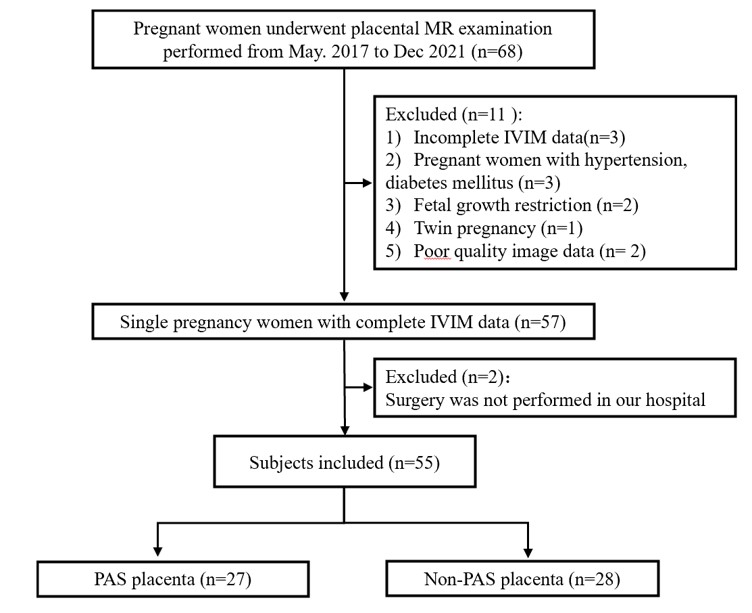
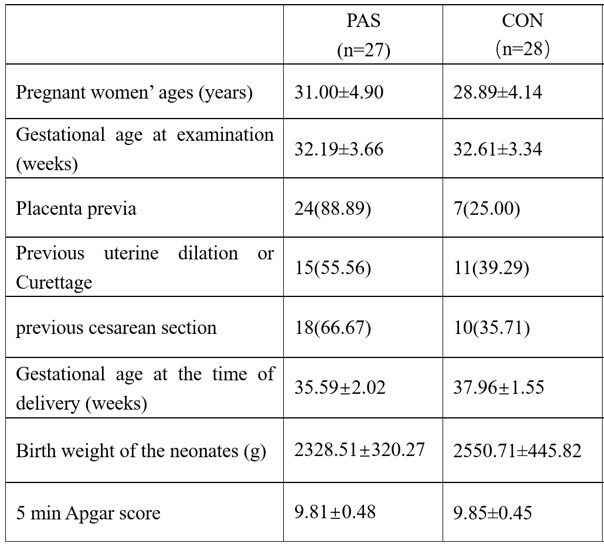
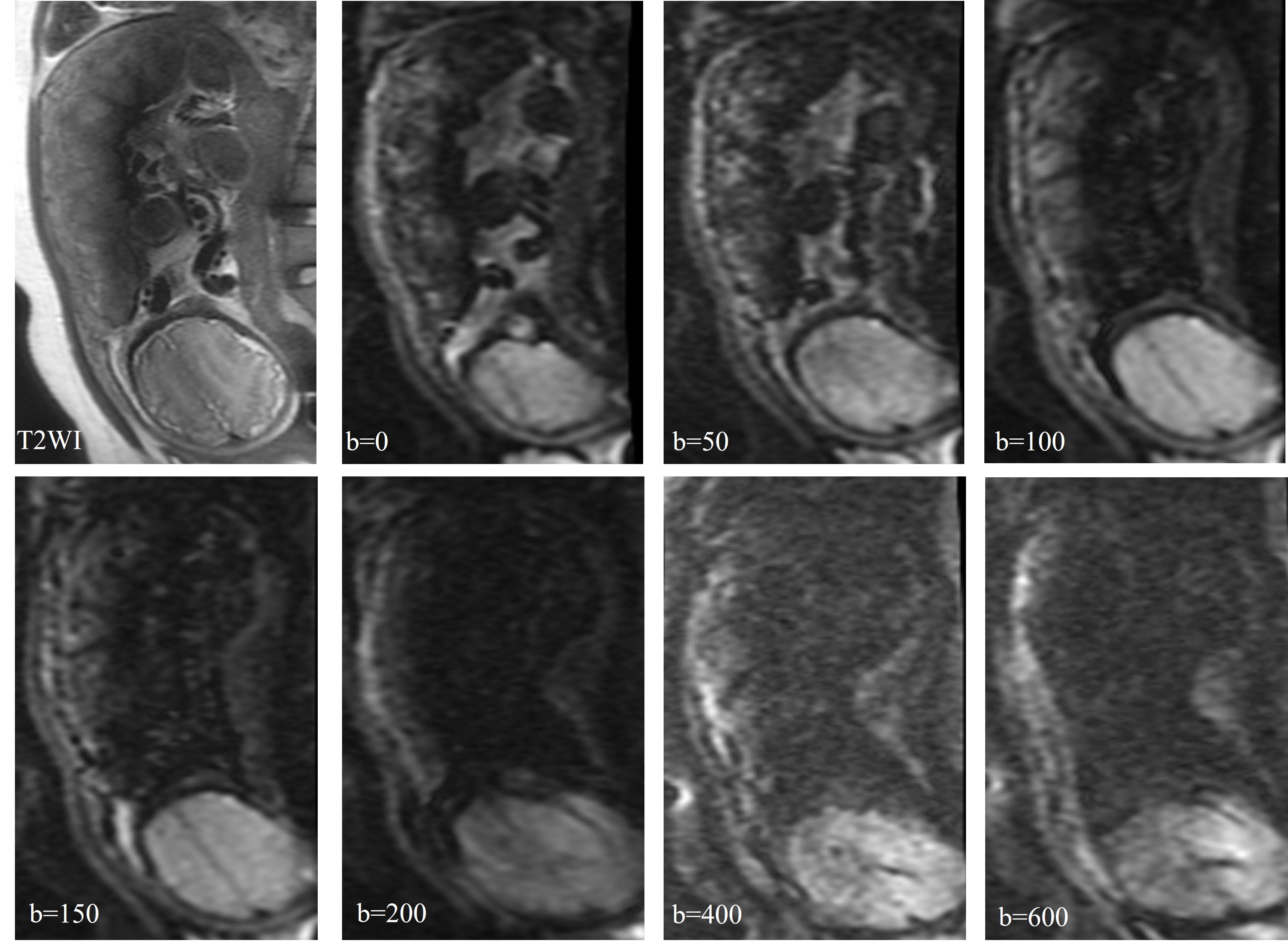
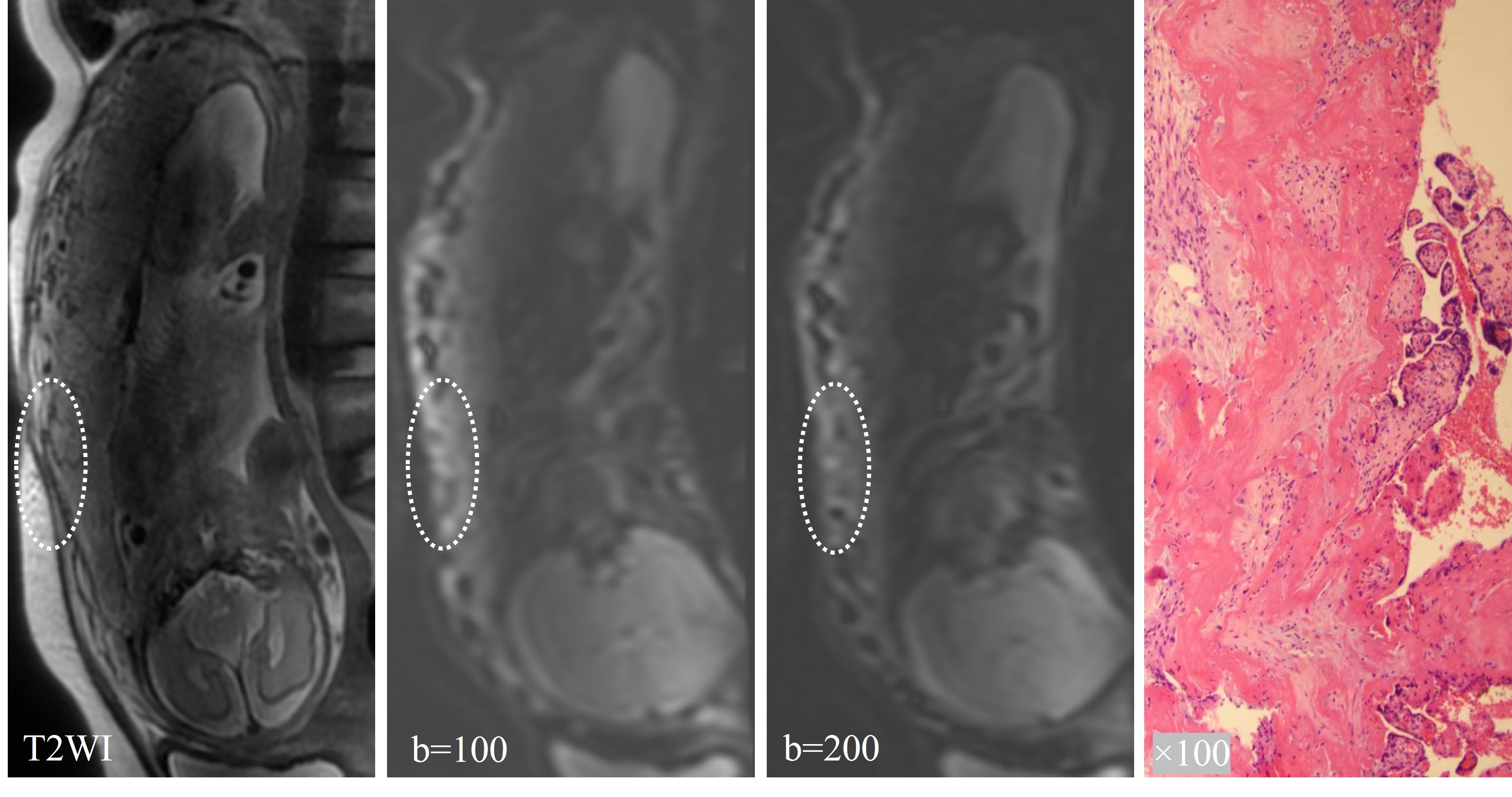
A total of 55 pregnant women were included in the study with 27 patients with PAS were included as PAS group and 28 subjects without PAS were included as control group (Figure 1). All patients with PAS had their diagnosis confirmed by intraoperative and pathological findings. Table 1 demonstrated the clinical characteristics of the mothers as well as the fetuses in the PAS and control groups.In the original IVIM images with b values of 50-600, the three-layer structure of the placental margin was shown (Figure 2). Combining all the cases in this study, b values between 50-200 could be shown clearly. When b=0, the three-layer structure was not displayed, and when b>200 the three-layer structure were not shown clearly due to image deformation.
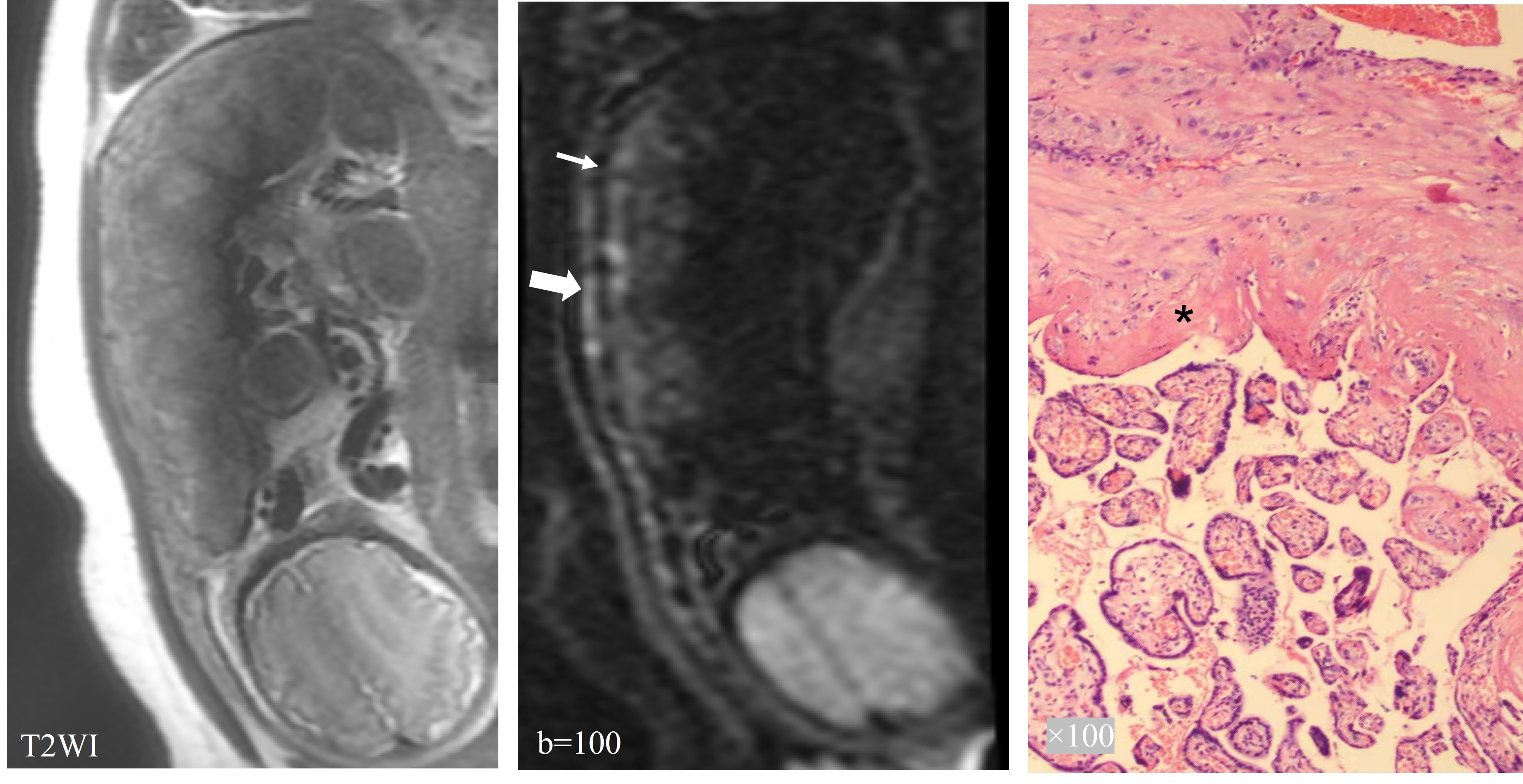
Figure 3 demonstrated three-layer structure of the placenta according to the images of pathologic tissue section. The original IVIM images clearly showed the outer myometrium as a strip of slightly high signal. There was a strip of low signal under the myometrium corresponding to the placental basal plate in the pathologic tissue section. The original IVIM image can more clearly show the myometrium as a strip of slightly high signal shadow, with a strip of low signal shadow under the myometrium corresponding to the basal layer of the placenta in the pathological section. Several short discontinuities (<10 mm in length) were seen in the low signal band of the basal layer, which was considered to be probably related to the curvature of the fibrous tissue of the basal layer (Figure 3C). The inner part of the basal plate was placental villous portion.
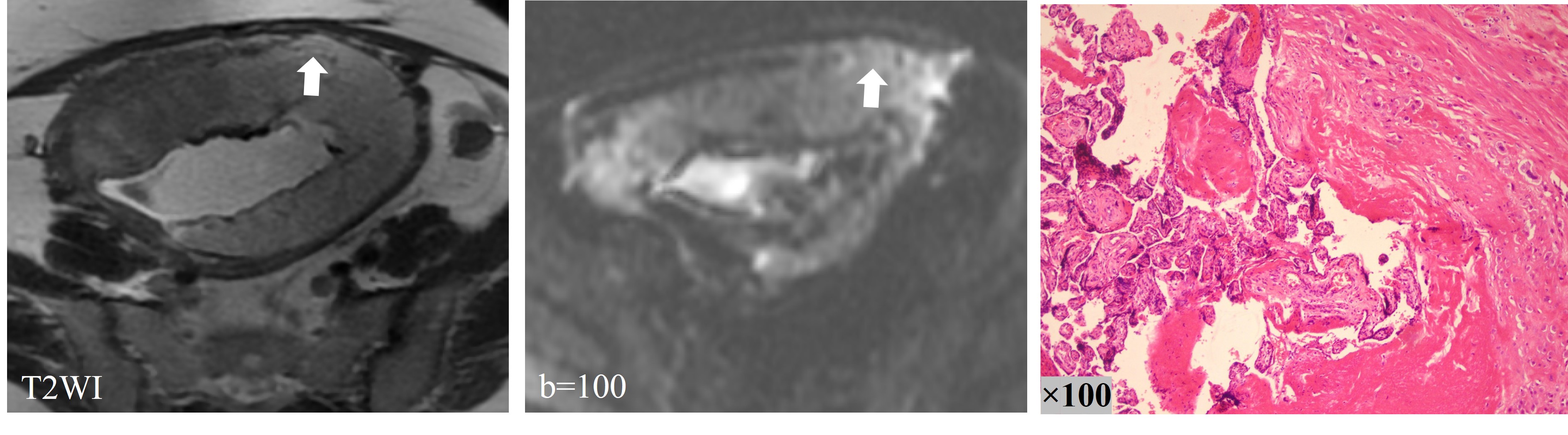
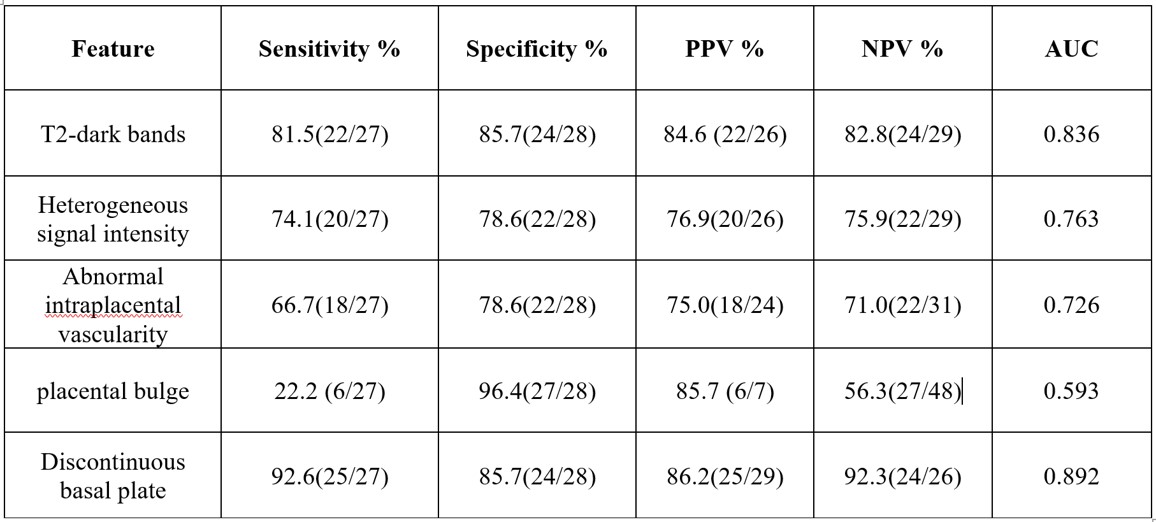
Figure 4 showed the characteristics of IVIM images of the placenta in patients with PA. Part of the basal plate disappeared (>10mm), and the myometrium could not be separated from placenta. T2WI images displayed partial bulge of placenta with PI, and IVIM images showed interrupted low signal bands of the basal layer at the same location (Figure 5). T2-dark bands, discontinuous myometrium, abnormal intraplacental vascularity and placental bulge are some of the most common signs of PAS diagnosed by conventional MRI. As shown in Table 2, comparing these signs of conventional MRI, sign of discontinuous basal plate in IVIM achieved the highest diagnostic sensitivity (92.6%) with an AUC of 0.892.
Discussion
Both ultrasound and conventional MRI have limitations in the diagnosis of PAS, especially the difficulty of preoperative staging diagnosis, which is a risk to the patient's intraoperative hemorrhage and even life safety. To our knowledge, there are no reports showing any imaging technique capable of visualizing the placental floor. And the demonstration of the integrity of the floor basal plate is very important for the diagnosis of PAS. This study first found that IVIM raw images can more clearly show the stratified structure of the basal plate, which is very helpful for the diagnosis of PAS, and to our knowledge this finding is the first reported. The ability to observe disruption of the placental basement membrane in PAS placentas, a sign with high sensitivity and AUC, suggests that this new finding could improve the diagnostic efficacy of MRI in the diagnosis of PAS.Acknowledgements
This work was supported by the National Key Research and Development Program of China (2016YFC0100300), National NaturalScience Foundation of China (No. 81471631, 81771810 and 51706178), the 2011 New Century Excellent Talent Support Plan of theMinistry of Education, China (NCET-11-0438) the Clinical Research Award of the First Affiliated Hospital of Xi’an Jiaotong University(No.XJTU1AF-CRF-2015-004), Research and Development Fund of the First Affiliated Hospital of Xi'an Jiaotong University(YK201509), Shaanxi Natural Science Basic Research Program Fund (2017JQ8034), Basic Research Fund of central Colleges(xjj2018jchz07).References
1. Millischer AE, Deloison B, Silvera S, et al. Dynamic contrast enhanced MRI of the placenta: A tool for prenatal diagnosis of placenta accreta? Placenta. 2017;53:40-47.
2. Familiari A, Liberati M, Lim P, et al. Diagnostic accuracy of magnetic resonance imaging in detecting the severity of abnormal invasive placenta: a systematic review and meta-analysis. Acta obstetricia et gynecologica Scandinavica. 2018;97(5):507-520.
3. Silver R, Barbour K. Placenta accreta spectrum: accreta, increta, and percreta. Obstetrics and gynecology clinics of North America. 2015;42(2):381-402.
4. Jauniaux E, Bhide A, Kennedy A, Woodward P, Hubinont C, Collins S. FIGO consensus guidelines on placenta accreta spectrum disorders: Prenatal diagnosis and screening. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2018;140(3):274-280.
5. Yan G, Liao Y, Li K, et al. Diffusion MRI Based Myometrium Tractography for Detection of Placenta Accreta Spectrum Disorder. Journal of magnetic resonance imaging : JMRI. 2022;55(1):255-264.
6. Lu T, Pu H, Li K, Mei J, Huang M, Wang S. Can introvoxel incoherent motion MRI be used to differentiate patients with placenta accreta spectrum disorders? BMC pregnancy and childbirth. 2019;19(1):531..
7. Lu T, Song B, Pu H, et al. Prognosticators of intravoxel incoherent motion (IVIM) MRI for adverse maternal and neonatal clinical outcomes in patients with placenta accreta spectrum disorders. Translational andrology and urology. 2020;9(2):258-266.
8. Lu T, Pu H, Cui W, Mei J, Huang M, Wang S. Use of intravoxel incoherent motion MR imaging to assess placental perfusion in patients with placental adhesion disorder on their third trimester. Clinical imaging. 2019;56:135-139.
9. Bao Y, Pang Y, Sun Z, Li Q, Tang D, Xia L. Functional diagnosis of placenta accreta by intravoxel incoherent motion model diffusion-weighted imaging. European Radiology. 2021;31(2):740-748.
Figures