2902
Subject-Specific Circular Artifacts in ASL Perfusion Imaging with 3D Stack-of-Spirals FSE Readout1United Imaging, Houston, TX, United States, 2United Imaging, Shanghai, China
Synopsis
Keywords: Artifacts, Arterial spin labelling
In perfusion images of ASL scans of brain, artifacts originated from unlabeled blood inflow can be effectively suppressed by inferior saturation. In our study with spiral-based readout, artifacts in the patterns of bright spots and concentric rings were determined to arise from arterial blood inflow. We discovered that the emergence of the artifacts is directly related to the carotid artery anatomies of human subjects. The artifacts appeared persistently for just one out of four participating volunteers. The application of inferior saturation should be favored to avoid such artifacts, which had been a fact not fully recognized from recent ASL studies.Introduction
3D stack-of-spirals (SOS) fast spin echo (FSE) has been an ideal readout sequence in arterial spin labeling (ASL) applications, owing to its inherent nature including efficient acquisition, higher sensitivity, and less susceptibility to motions. Nonetheless, spiral-based ASL may suffer contamination of artifacts arising from factors such as off-resonant spins. One of the many types of artifacts with an appearance of a bright spot center and concentric rings were previously generalized as “high signal spiral artifacts”1,2 or suggested to be resulted from physiological movements, e.g. pulsation3. This type of artifacts has not been explicitly investigated on human subjects. In this study, we looked into the cause of the artifacts with volunteers and found that the emergence of the artifacts is directly related to the carotid artery anatomies of the subjects. The artifacts emerged persistently for one of the four volunteers, whereas unnoticeable for the rest. Consistent results for each subject were obtained with repeated scans. Employment of inferior saturation pulses at specific timings during post-labeling delay was proven to be effective to avoid such circular artifacts and should be proposed for routine clinical ASL scans.Methods
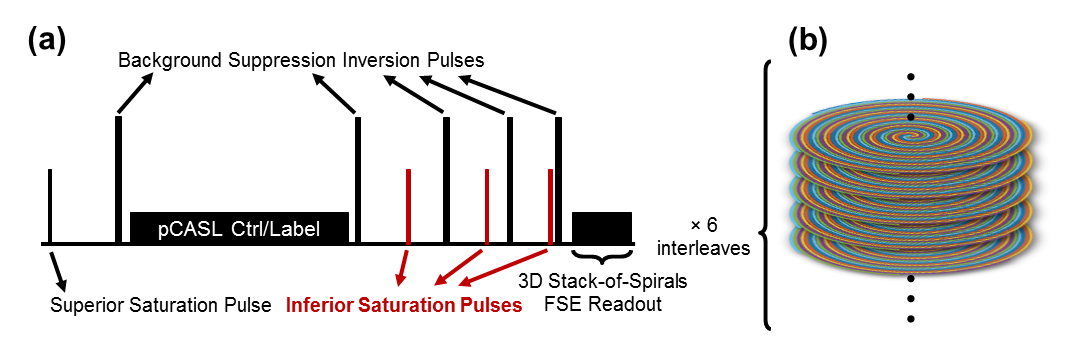
As shown in Figure 1(a), a superior saturation pulse and a selective inversion pulse were applied prior to pseudo-continuous ASL (pCASL) control/labeling pulses, together with four non-selective inversion pulses following the control/labeling block for background suppression. Three inferior saturation pulses were positioned between every two consecutive non-selective inversion pulses. The timings of the saturation and inversion pulses were set according to a previous study.4 To inspect the variations of the circular artifacts, the ASL sequences with and without the three inferior saturation pulses were conducted with four healthy volunteers (40.25 ± 8.66 y/o) at 3.0 T using a 75-cm wide bore uMR Omega scanner (United Imaging), and the pairs of scans were repeated for each volunteer on later days. The k-space based on the employed 3D SOS FSE readout sequence is shown in Figure 1(b). Echoes along the FSE echo train were assigned to a series of slice encodings. 6 spiral interleaves compose each stack of the 3D k-space, resulting in 6 SOS FSE shots to fulfill the k-space acquisition. TR/TE = 5200/7.84 ms. Labeling duration and post-labeling delay were both 1800 ms. In-plane field-of-view (FOV) was 220×220 mm2 and matrix size was 64×64. Slice oversampling was set to 15%. Slice thickness was 4 mm and 28 axial slices were shown to cover a whole brain. Bandwidth was 1570 Hz/pixel. With 4 averages, the duration of each ASL scan was 4:42 min. Time-of-flight (TOF) angiography based on gradient echo (GRE) sequence at the same center of FOV as ASL scans was applied to a voluteer for characterizing the arterial anatomy. TR/TE settings were 16.1 ms and 3.5 ms. In-plane FOV was 220×220 mm2 and matrix size was 256×256. Slice thickness was 1 mm and 92 axial slices were selected to approximately match the ASL FOV. Slice oversampling was set to 20%. Slice interpolation ratio was 2. Bandwidth was 220 Hz/pixel. Scan duration was 3:52 min.Results
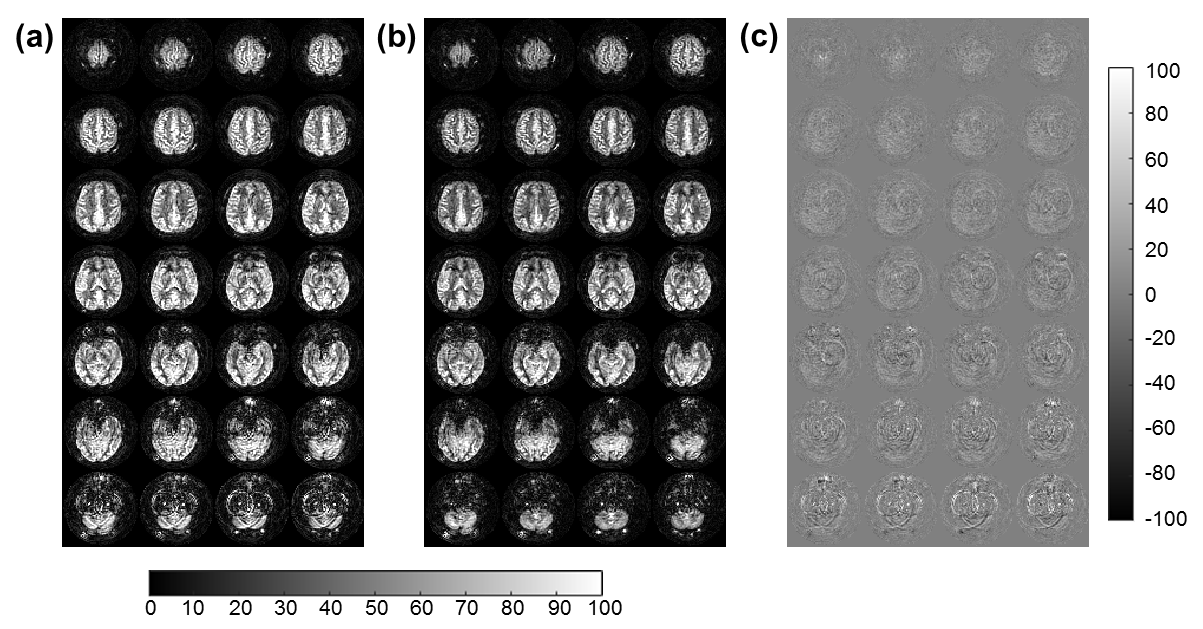
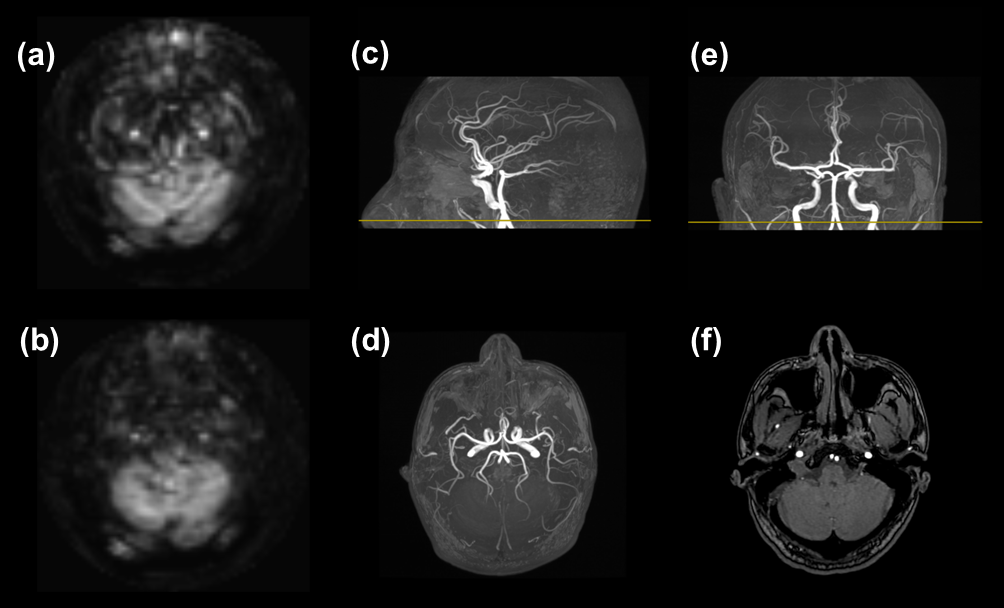
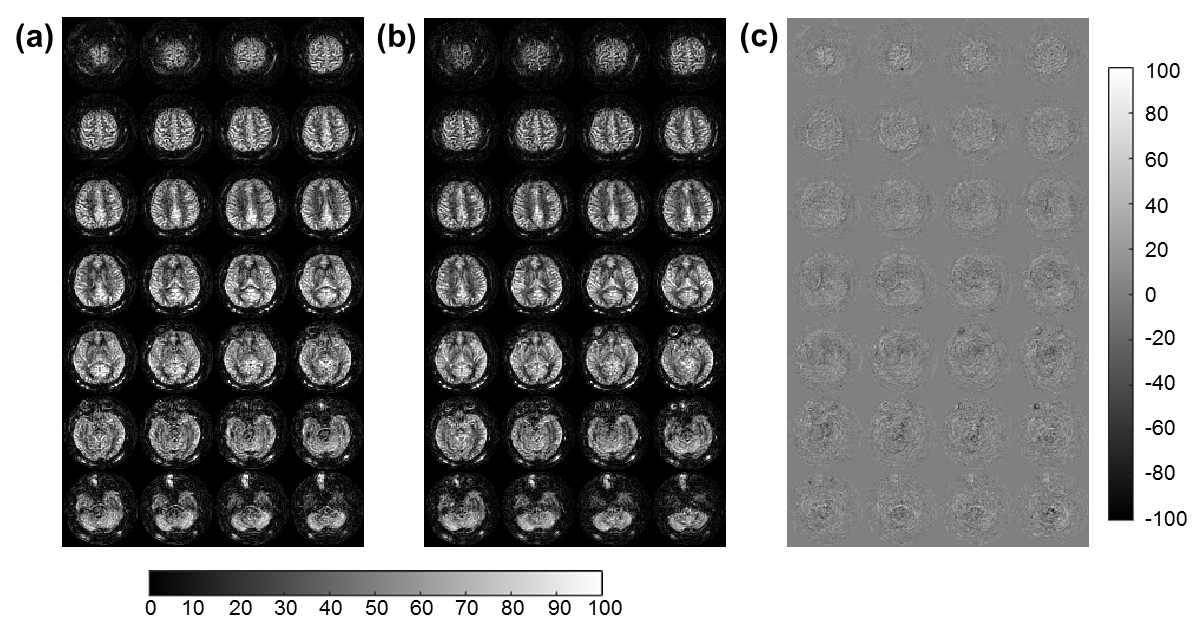
There were particularly distinct differences between ASL perfusion images with and without the inferior saturation for one of the four healthy volunteers. When no inferior saturation pulses were applied, artifacts in the forms of two bright spots and corresponding concentric rings could be evidently identified, especially in the inferior slices covering the cerebellum (Figure 2a). These artifacts were largely eliminated while the pulses were switched on in a following scan (Figure 2b). The artifacts can be more easily discerned by subtracting Fig. 1b from Fig 1a, as exhibited in Figure 1(c), where it’s distinct that the artifacts contaminate quite a few central slices as well. With a TOF angiography scan, we were able to directly attribute the bright spots to two large carotid arteries with inflowing blood (Figure 3). However, for the other three volunteers, such kind of artifacts was not observed with and without the incorporation of these saturation pulses. One such example is shown in Figure 4 where no swirls/circles could be discerned even in the subtraction image. The above scans were repeated 3-5 times for each of the volunteers and consistent results were obtained.Discussion and Conclusion
Based on the investigation with repeated scans, the circular artifacts were only observed from one out of the four healthy volunteers in our study. We suggest that the artifact is precisely related to the anatomical characteristics from a fraction of human subjects. Despite that the inferior saturation may be advised to be optional in some clinical protocols, it should be highly recommended to have it selected to play safe. Perfusion quantification accuracy can be largely destructed by the artifacts so that they need to be avoided. No systematic difference between perfusion images with and without the saturation pulses were discovered for the three volunteers not exhibiting the artifacts, indicating that interior saturation pulses merely act on unlabeled blood inflow after ASL control/labeling period. The benefit of inferior saturation may not be fully recognized from ASL studies on different organs or body parts.1 Here, we would like to emphasize the importance of the inferior saturation strategy to prevent perfusion quantification errors for improved clinical diagnosis.Acknowledgements
No acknowledgement found.References
1. Lin, Chien-Hung, et al. "Feasibility of Arterial Spin Labeling Magnetic Resonance Imaging for Musculoskeletal Tumors with Optimized Post-Labeling Delay." Diagnostics (2022).
2. Amukotuwa, Shalini A., et al. "3D Pseudocontinuous arterial spin labeling in routine clinical practice: A review of clinically significant artifacts." Journal of Magnetic Resonance Imaging (2016).
3. Dai, Weiying, et al. "Continuous flow‐driven inversion for arterial spin labeling using pulsed radio frequency and gradient fields." Magnetic Resonance in Medicine (2008).
4. Robson, Philip M., et al. "Strategies for reducing respiratory motion artifacts in renal perfusion imaging with arterial spin labeling." Magnetic Resonance in Medicine (2009).
Figures