2861
Brain redundancy metric in cerebral small vessel disease:A community-based study.1Radiology, The second affiliated hospital of ZheJiang University, Hangzhou, China
Synopsis
Keywords: Brain Connectivity, fMRI (resting state), redundancy
We applied a dynamic whole-brain network metric, redundancy, to a community-based middle-aged and elderly population, revealed the potential mechanisms of SVD on cognitive impairment ; we also explored the relationship between cognitive reserve and brain redundancy metric.We found that aging, hypertension and lacunes could impair redundancy in brain networks, whereas better brain redundancy corresponds to better executive function, which partly explains the potential mechanism of cognitive impairment by SVD. Secondly, we found no significant correlation between redundancy and cognitive reserve.
Introduction
Small vessel disease (SVD) means patients with clinical features or neuroimaging lesions of presumed vascular origin attributable to abnormal cerebral perforating vessels(1).Presenting to some extent in virtually every individual aged 60 years or older(2),SVD is now recognized to be the most important vascular contributor to dementia(3).Common radiological markers of SVD include white matter hyperintensities (WMHs), lacunes, enlarged perivascular spaces, microbleeds, recent small subcortical infarcts and brain atrophy(4).Previous studies have found a strong correlation between brain imaging severity and cognitive impairment in SVD(5-7).However, many individuals remain functionally independent despite a considerable burden of SVD . An alternative approach has proposed the ‘cognitive reserve’ concept to explain this phenomenon, which referring to lifetime experiences, such as education (8).Previous studies of brain functional networks are considered to be a great way to explore cognitive reserve. Recently, a new brain function network metric, redundancy, has become available.Defined as the existence of alternate elements within a system that ensure functionality in case of failure, redundancy has been suggested to operate as a neuroprotective mechanism that is deployed in the early stages of neurodegenerative diseases such as Parkinson's disease (PD) (9, 10)and Alzheimer's disease (AD)(11) .
No study has yet explored the relationship between redundancy and SVD. Therefore, in the present study, we aimed to reveal the potential mechanisms of SVD on cognitive impairment through redundancy metric in a community-based middle-aged and elderly population; we also explored the relationship between cognitive reserve and brain redundancy metric, and we hypothesized that cognitive reserve is the basis for the formation of brain redundancy network, and SVD may damage the redundancy network and thus cause cognitive impairment.
Methods
Denote a network G with a node set V (G) and an edge set E(G). G is connected if there is a path between any pair of nodes. A connected network G is called 2-connected if, for every two node x, y ∈ V (G), there are at least two independent paths between x and y.We based on sliding window approach, using pairwise Pearson’s correlation to construct whole-brain dynamic functional network models in Shen268 atlas for 158 community subjects. On each window (among all T windows), multiple binary networks are formed with N different density levels to create N binary networks for each t. We further define state vector ‘bt’ to quantitatively characterize spatiotemporal changes of network redundancy. Let b∈ {bt} (1 ≤ t ≤ T), where bt = 1 if the minimally connected network in t (among all N binary networks in t) is not 2-connected and bt = 2, otherwise. Redundancy is defined as the percentage of count 2 in {bt}.
Cognitive reserve was assessed using the CRIq scale. The relationship between redundancy and demographic indicators was analyzed using Pearson’s correlation; the relationship between redundancy and SVD imaging marker and cognition was explored using partial correlation analysis; and further differences between groups were determined using independent samples t-tests.
Results
Redundancy is associated with age and presence of hypertension; Grouping according to presence of lacunes or not showed significant differences in redundancy between groups. Regressing out the age, gender, and education, redundancy is negatively correlated with time to TMTB completion; further regressing out the number of lacunes, the negative correlation remained. No relationship found between redundancy and cognitive reserve.Discussion
We applied redundancy, such a dynamic whole-brain network metric, to a community-based middle-aged and elderly population,and found that aging,hypertension as well as lacunes could impair redundancy in brain networks, whereas better brain redundancy corresponds to better executive function, which partly explains the potential mechanism of cognitive impairment by SVD. Secondly, we found no significant correlation between redundancy and cognitive reserve, speculating that because the effect of cognitive reserve on functional brain networks was previously found to be regional, while redundancy acts as a whole-brain metric may not provide insight into the differences.Acknowledgements
Thanks to my advisor,my lab and ljx.References
1. Wardlaw JM, Benveniste H, Williams A. Cerebral Vascular Dysfunctions Detected in Human Small Vessel Disease and Implications for Preclinical Studies. Annual review of physiology. 2022;84:409-34.
2. Ter Telgte A, van Leijsen EMC, Wiegertjes K, Klijn CJM, Tuladhar AM, de Leeuw FE. Cerebral small vessel disease: from a focal to a global perspective. Nature reviews Neurology. 2018;14(7):387-98.
3. METACOHORTS for the study of vascular disease and its contribution to cognitive decline and neurodegeneration: An initiative of the Joint Programme for Neurodegenerative Disease Research. Alzheimer's & dementia : the journal of the Alzheimer's Association. 2016;12(12):1235-49.
4. Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. The Lancet Neurology. 2013;12(8):822-38.
5. Cheng HL, Lin CJ, Soong BW, Wang PN, Chang FC, Wu YT, et al. Impairments in cognitive function and brain connectivity in severe asymptomatic carotid stenosis. Stroke. 2012;43(10):2567-73.
6. Schaefer A, Quinque EM, Kipping JA, Arélin K, Roggenhofer E, Frisch S, et al. Early small vessel disease affects frontoparietal and cerebellar hubs in close correlation with clinical symptoms--a resting-state fMRI study. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 2014;34(7):1091-5.
7. Zhou Y, Yu F, Duong TQ. White matter lesion load is associated with resting state functional MRI activity and amyloid PET but not FDG in mild cognitive impairment and early Alzheimer's disease patients. Journal of magnetic resonance imaging : JMRI. 2015;41(1):102-9.
8. Stern Y. Cognitive reserve. Neuropsychologia. 2009;47(10):2015-28.
9. Arkadir D, Bergman H, Fahn S. Redundant dopaminergic activity may enable compensatory axonal sprouting in Parkinson disease. Neurology. 2014;82(12):1093-8.
10. Postuma RB, Montplaisir J. Predicting Parkinson's disease - why, when, and how? Parkinsonism & related disorders. 2009;15 Suppl 3:S105-9.
11. Ghanbari M, Zhou Z, Hsu LM, Han Y, Sun Y, Yap PT, et al. Altered Connectedness of the Brain Chronnectome During the Progression to Alzheimer's Disease. Neuroinformatics. 2022;20(2):391-403.
Figures
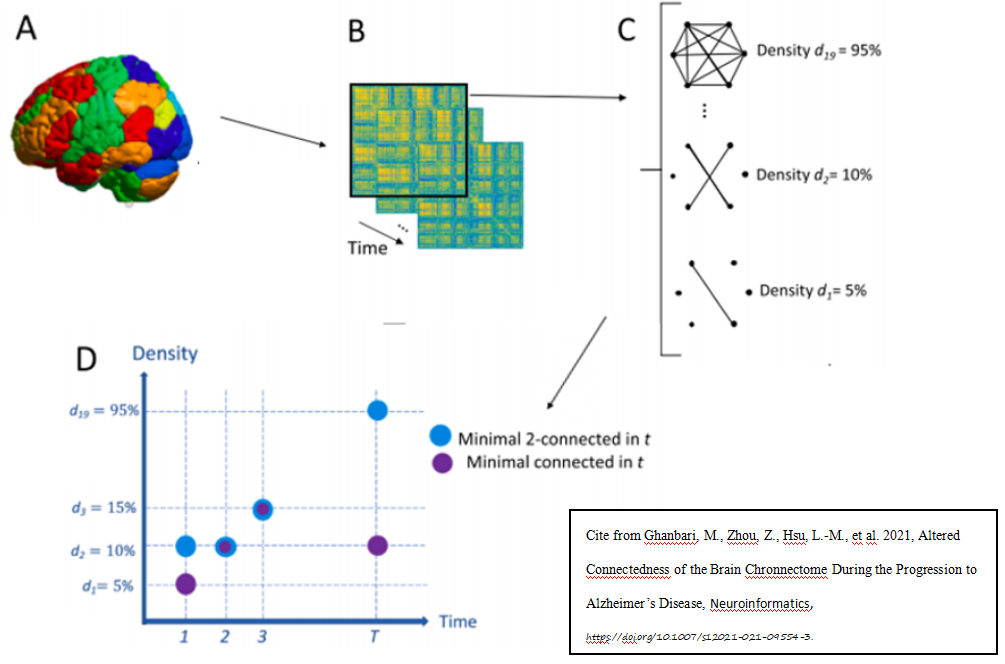
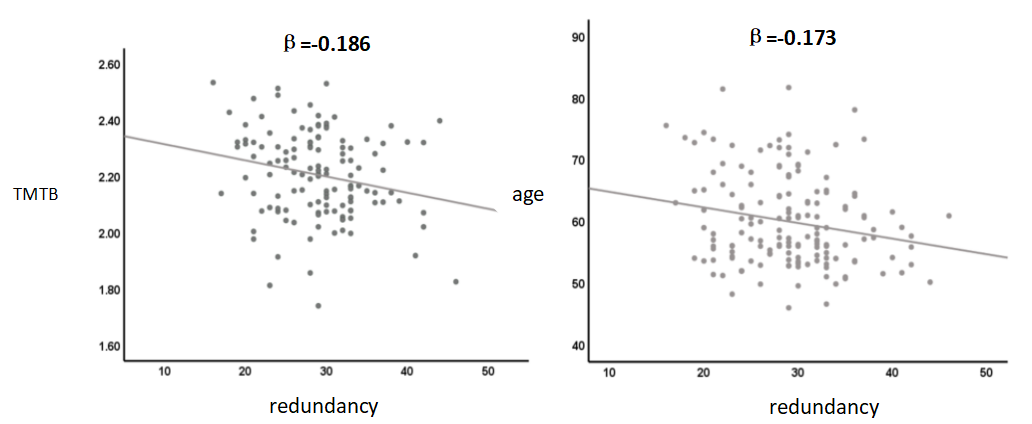
Fig. 2.Left:The relationship between brain redundancy and TMTB completion time.Right:The relationship between brain redundancy and age.
Horizontal coordinates indicate brain redundancy.
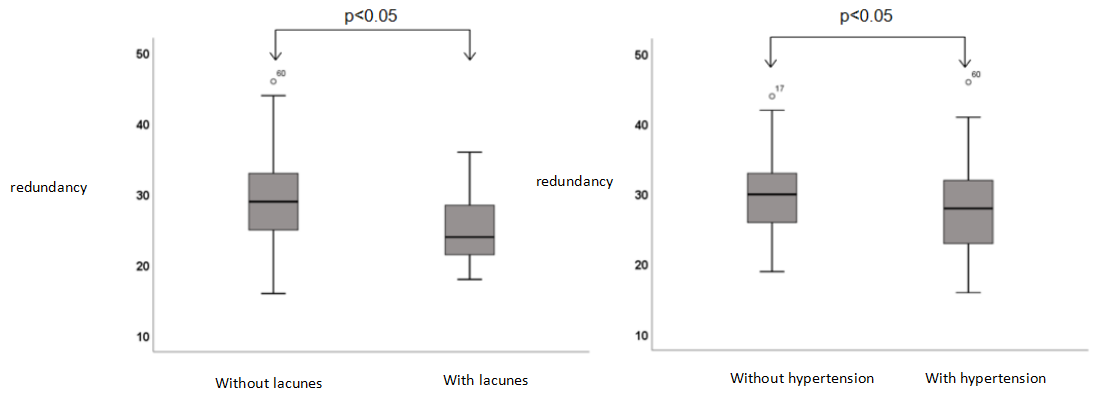
Fig. 3.Left:The difference of brain redundancy between with and without lacunes group.Right:The difference of brain redundancy between with and without hypertension group.
Vertical coordinate indicate brain redundancy.