2857
Aberrant functional connectivity density in different cognitive states of T2DM patients1Shaanxi Provincial People’s Hospital, Xi’an, China, 2Philips Healthcare, Xi’an, China
Synopsis
Keywords: Brain Connectivity, fMRI, T2DM
To investigate the underlying neural mechanism of T2DM-related brain damage, the functional connectivity density (FCD) mapping method was used to examine the density distribution of whole-brain resting functional connectivity from 77 patients with T2DM under different cognitive states (with normal cognitive function, DMCN and mild cognitive impairment, DMCI) and 40 healthy controls (HCs). The decreased long-range FCD in the left superior temporal gyrus (STG) in DMCI patients and its correlation with Rey Auditory Verbal Learning Test (RAVLT) score in all T2DM patients, which suggested left STG may be involved in the neuropathology of auditory memory in T2DM patients.Introduction
Type 2 diabetes mellitus (T2DM) increase the risk of mild cognitive impairment (MCI) and promote the patients who convert from MCI to dementia[1]. However, the exact neurophysiological mechanism of T2DM-related brain damage remains unknown. FCD reflects to a large extent of the brain information communication capability. Several studies have confirmed that the balance of FCD disorder is closely related to cognitive impairment[2]. As the brain is vulnerable to the fluctuations in plasma glucose levels, the impaired glucose homeostasis caused by T2DM may disrupt the established balance of short- and long-range FCD[3]. Therefore, exploring the altered pattern of FCD in T2DM patients under different cognitive states may better reflect the functional abnormalities caused by long-term abnormal glucose homeostasis, and will help to fully reveal the neural mechanism of cognitive impairment in T2DM.Material and Methods
MRI data of 37 DMCN, 40 DMCI and 40 HCs were obtained from a 3.0-T scanner (Ingenia, Philips Healthcare, the Netherlands) with a 16-channel phased-array head coil. Resting-state functional BOLD images were acquired by using a gradient-echo planar sequence with the following parameters: TR = 2000 ms, TE = 30 ms, FA = 90◦, 200 volumes, thickness = 4 mm (no gap), slices = 34, FOV = 230 mm × 230 mm and matrix = 128 × 128. Sagittal 3-dimensional T1-weighted images were obtained using a fast spoiled gradient echo sequence with the following parameters: TR = 7.5 ms, TE = 3.5 ms, FA = 8◦, thickness = 1 mm (no gap), slices = 328, FOV = 250 mm × 250 mm and matrix = 256 × 256. All subjects also underwent a battery of clinical and neuropsychological examination. Functional data were preprocessed by DPARSF_V4.3 (http://www.restfmri.net/forum/DPARSF) and custom-written software in Neuroscience Information Toolbox (NIT). One-way ANOVA was utilized to compare the clinical features, neuropsychological scores and the FCD maps across the three groups. GRF correction and least significant difference (LSD) were used to perform post hoc comparisons.Results
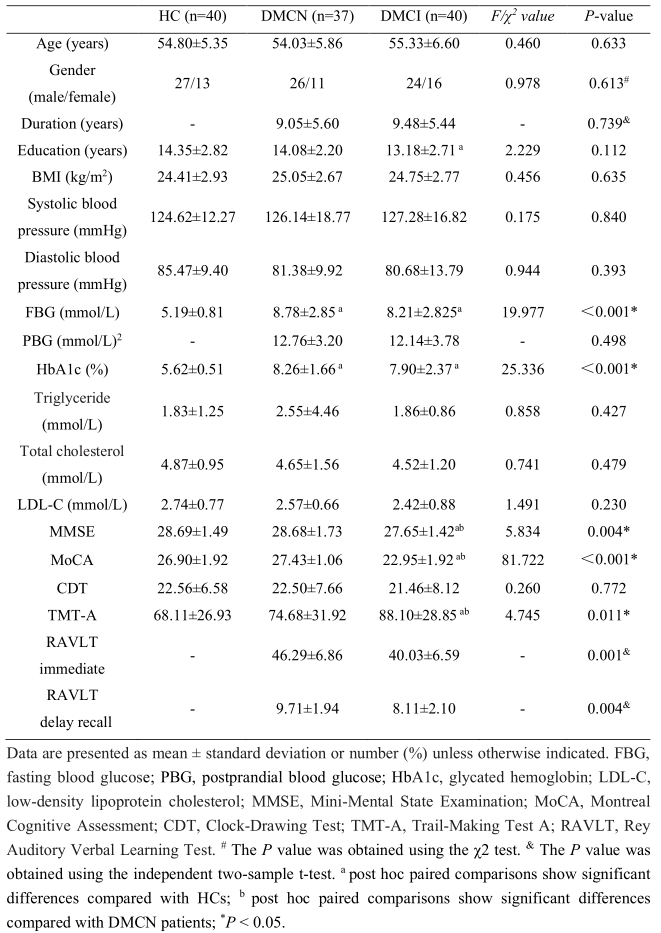
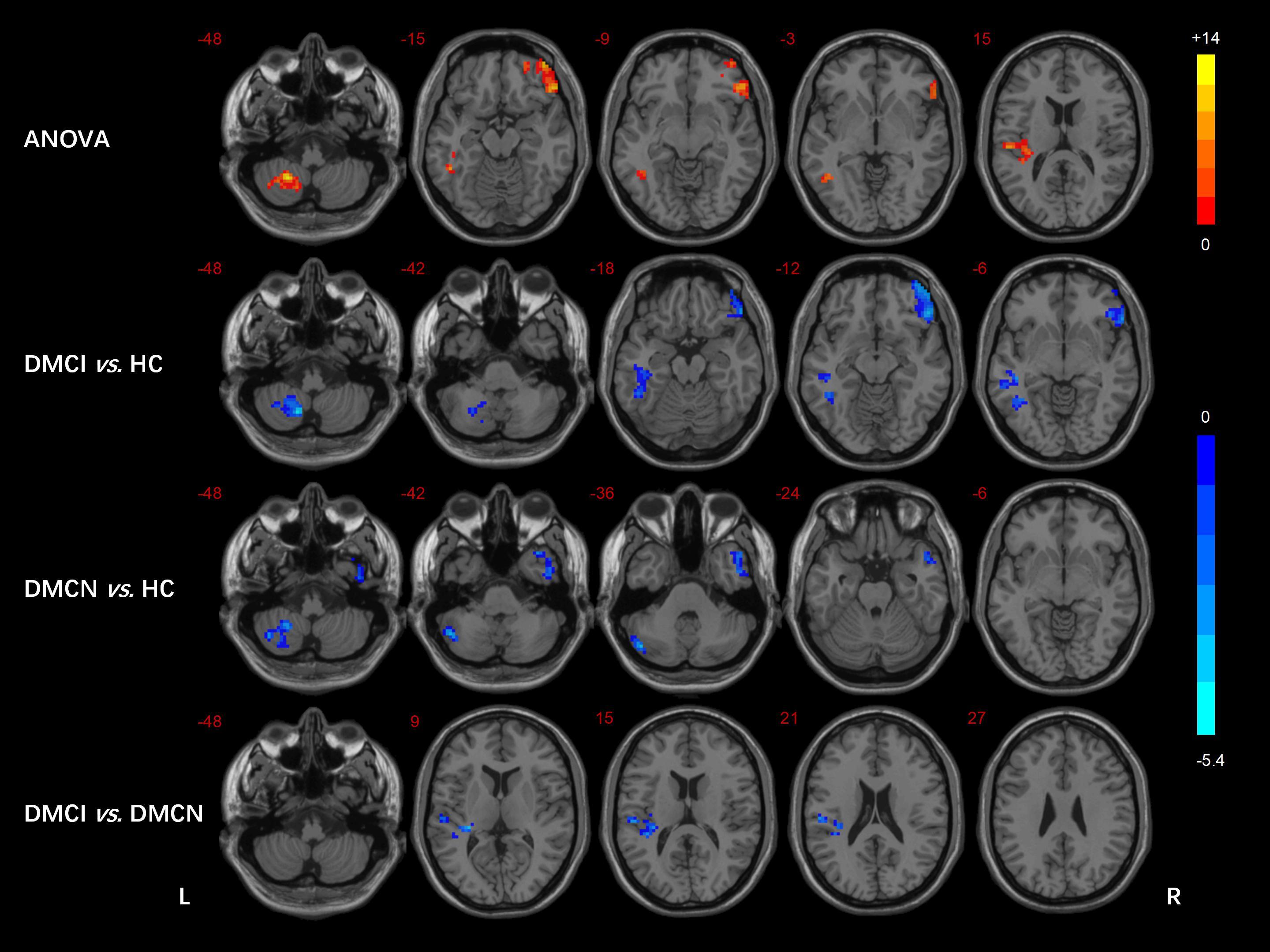
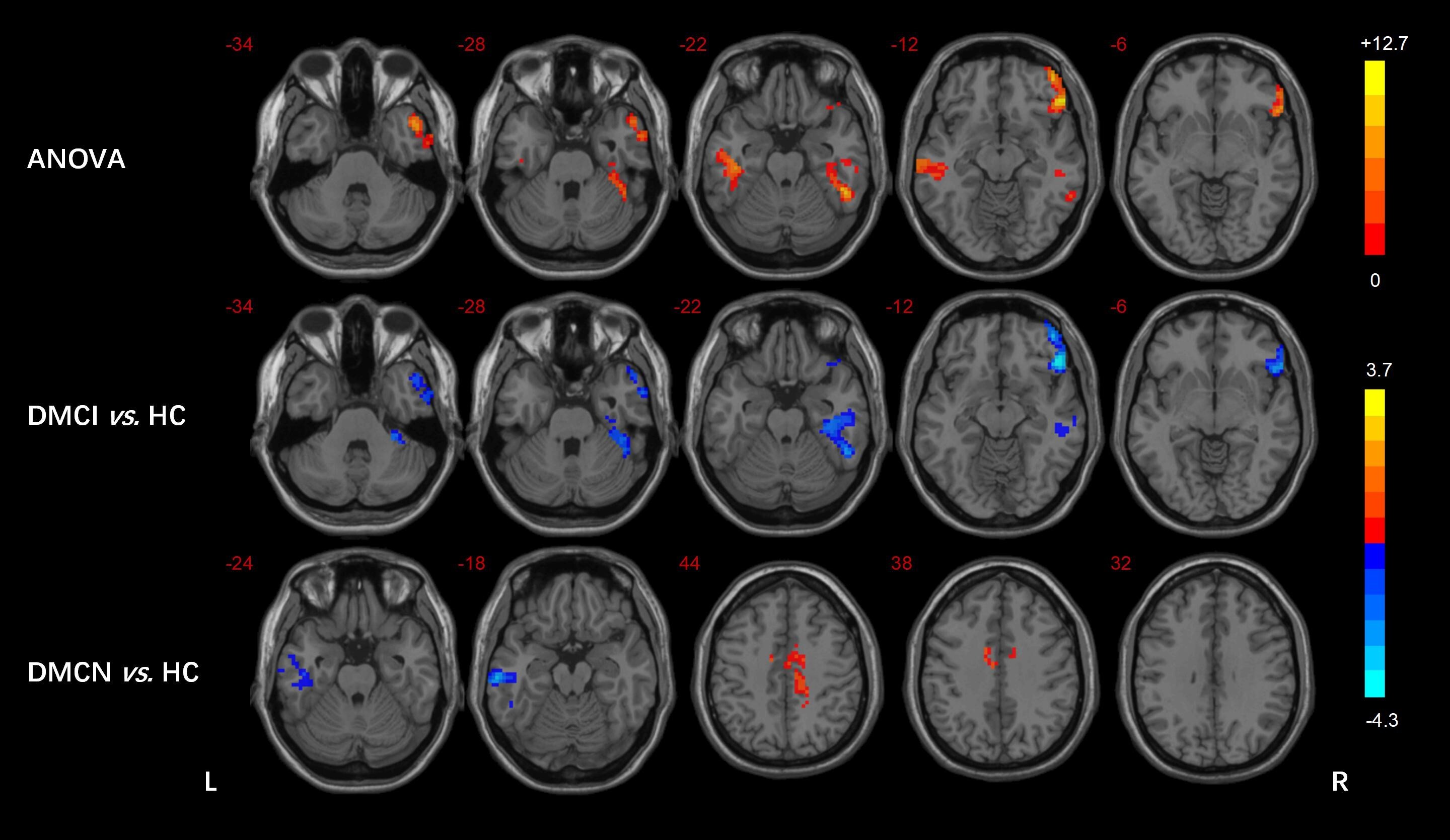
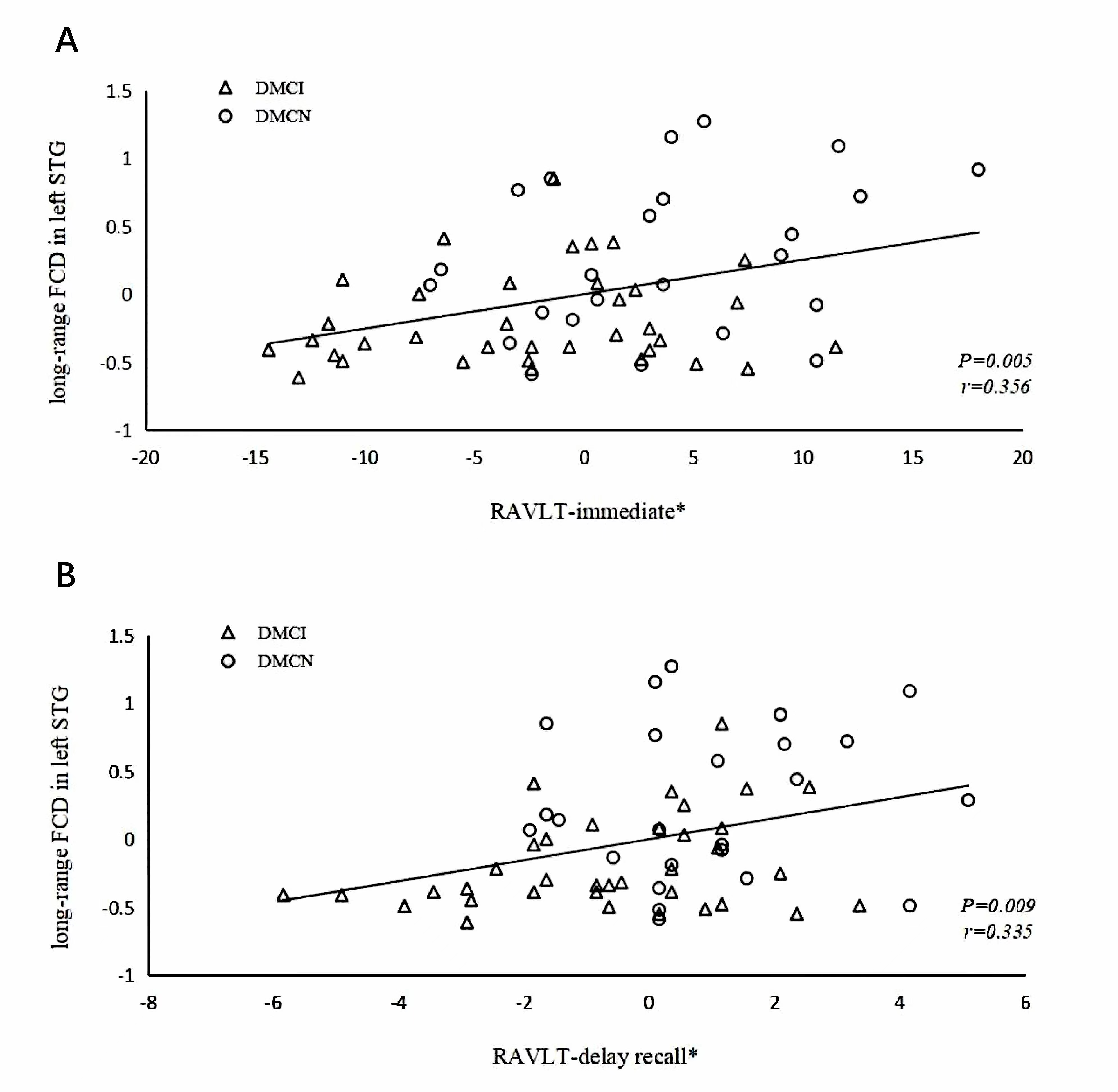
Table 1 shows the demographic, clinical and neuropsychological data of all participants. Compared with HCs, the two T2DM groups showed higher FBG and HbA1c scores, and the DMCI group had fewer years of education (all Ps < 0.05). In addition, the DMCI group had poorer MMSE, MoCA scores and higher TMT-A scores compared to the DMCN group and HCs, and poorer RAVLT immediate and delay recall scores compared to the DMCN group (all Ps < 0.05). We also found short- and long-range FCD of multiple brain regions were significantly different by ANOVA. Between-group analysis demonstrated the abnormal FCD regions in T2DM patients mainly located in the temporal lobe and cerebellum, but the abnormal functional architecture in DMCI patients is more extensive (Figure 1 and 2). After controlling for education, we observed significant positive correlation between the long-range FCD in left STG and RAVLT immediate (r = 0.356, P = 0.005) and delay recall (r = 0.335, P = 0.009) scores in all T2DM group (Figure 3).Discussion
The results of this study showed that the patterns of functional architecture in T2DM patients with different cognitive status were somewhat similar, but not completely consistent. Middle temporal gyrus (MTG) has emerged as a network hub of semantic processing, and mainly contributes to controlled semantic retrieval processes[4]. Our results may provide some clues for further exploration of semantic cognitive dysfunction in T2DM. Inferior temporal gyrus (ITG) is an important part of the ventral visual pathway, it is believed that information of primary visual cortex is transmitted to ITG through ventral visual pathway, culminating in high-level visual representations[5]. Our results also provide some new insights to elucidate visual cognitive dysfunction in patients with T2DM. Cerebellar lobule Ⅷ and crus I/II belong to the posterior cerebellum, which are closely related to sensorimotor task, and several studies have confirmed that the posterior cerebellum is susceptible to diabetes-related disruptions[6]. There were 46 T2DM patients with diabetic peripheral neuropathy in our study, which may be the reason for the aberrant FCD in the cerebellum. The right inferior frontal gyrus (IFG) is a central region for executive control and is involved in a variety of higher cognitive functions[7], we hypothesized that the reduced global FCD of right IFG in this study may suggest abnormal executive function in the DMCI patients. The left STG is a shared substrate for auditory short-term memory and speech comprehension, the structural integrity of the STG and sulcus predicted auditory short-term memory capacity[8]. DMCI group showed decreased long-range FCD in the left STG compared with DMCN group, which may suggest impaired cognitive function of auditory memory in DMCI patients. In addition, the z scores of long-range FCD in the left STG were positively correlated with the scores of RAVLT immediate recall and long-term delayed recall scores, which further confirms our speculation.Conclusion
In summary, the FCD method found that the altered patterns of functional characteristics were different in T2DM under different cognitive states. DMCI patients have more functional architecture abnormalities in higher-level cognitive function (executive function and auditory memory function). In addition, left STG may be involved in the neuropathology of auditory memory in T2DM patients, which provides some new insights into the neural mechanisms of T2DM-related cognitive impairment.Acknowledgements
This research was supported by the National Natural Science Foundation of China (82170820), the Key Research and Development Program of Shaanxi Province of China (2018ZDXM-SF-038), and the Shaanxi Provincial People’s Hospital Technological Development Incubation Foundation of China (2020YXM-04).References
[1] Koekkoek PS, Kappelle LJ, van den Berg E, et al. Cognitive function in patients with diabetes mellitus: guidance for daily care[J]. Lancet Neurol, 2015, 14 (3): 329-340.
[2] Song Y, Wu H, Chen S, et al. Differential Abnormality in Functional Connectivity Density in Preclinical and Early-Stage Alzheimer's Disease[J]. Front Aging Neurosci, 2022, 14: 879836.
[3] Bullmore E, Sporns O. The economy of brain network organization[J]. Nat Rev Neurosci, 2012, 13 (5): 336-349.
[4] Tune S, Asaridou SS. Stimulating the Semantic Network: What Can TMS Tell Us about the Roles of the Posterior Middle Temporal Gyrus and Angular Gyrus?[J]. J Neurosci, 2016, 36 (16): 4405-4407.
[5] Serre T. Models of visual categorization[J]. Wiley Interdiscip Rev Cogn Sci, 2016, 7 (3): 197-213.
[6] Fang P, An J, Tan X, et al. Changes in the cerebellar and cerebro-cerebellar circuit in type 2 diabetes[J]. Brain Res Bull, 2017, 130: 95-100.
[7] Schaum M, Pinzuti E, Sebastian A, et al. Right inferior frontal gyrus implements motor inhibitory control via beta-band oscillations in humans[J]. Elife, 2021, 10.
[8] Leff AP, Schofield TM, Crinion JT, et al. The left superior temporal gyrus is a shared substrate for auditory short-term memory and speech comprehension: evidence from 210 patients with stroke[J]. Brain, 2009, 132 (Pt 12): 3401-3410.
Figures