2754
Total Generalized Variation (TGV) Constrained Reconstruction Improves Test-retest Reliability of High Resolution 3D pCASL in Children1Laboratory of Functional MRI Technology (LOFT), Stevens Neuroimaging and Informatics Institute, University of Southern California, Los Angeles, CA, United States, 2Department of Population and Public Health Sciences, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States, 3Institute of Biomedical Imaging, Graz University of Technology, Graz, Austria
Synopsis
Keywords: Arterial spin labelling, Brain
We developed an accelerated multi-delay 3D pCASL scheme with high-resolution (iso-2mm), CAIPI acceleration and TGV reconstruction to achieve a ~9-minute protocol with 5 delays with 8 averages per delay. We tested the feasibility of this protocol on 19 pediatric subjects and found the proposed imaging protocol with TGV constrained reconstruction can improve the test-retest reliability of high-resolution 3D pCASL perfusion imaging in typically developing children compared to a standard segmented acquisition.Introduction
Pseudo Continuous Arterial Spin Labeling (pCASL) is a promising imaging technique to quantify cerebral blood flow (CBF) and has been applied to many studies of neurodevelopment1,2. Multi-delay ASL was proposed to achieve more accurate quantification of both CBF and arterial transit time (ATT) through fitting a kinetic model3. However, acquiring multi-delay perfusion images would require longer scan time and this would make it especially challenging for pediatric imaging with more possibilities for head motion. Accelerated acquisition and reconstruction with parallel imaging can be used to shorten scan time and thus reduce motion artifacts with constrained reconstruction and denoising methods. In this work, we developed a protocol with 2×4 CAIPIRINHA acceleration and spatio-temporal total generalized variation (TGV) constrained reconstruction to achieve whole brain isotropic 2mm multi-delay 3D pCASL with 5 post labeling delays (PLDs) in 8 minutes and 33 seconds. We tested this protocol on 19 typically developing children who underwent repeated MRI scans.Methods
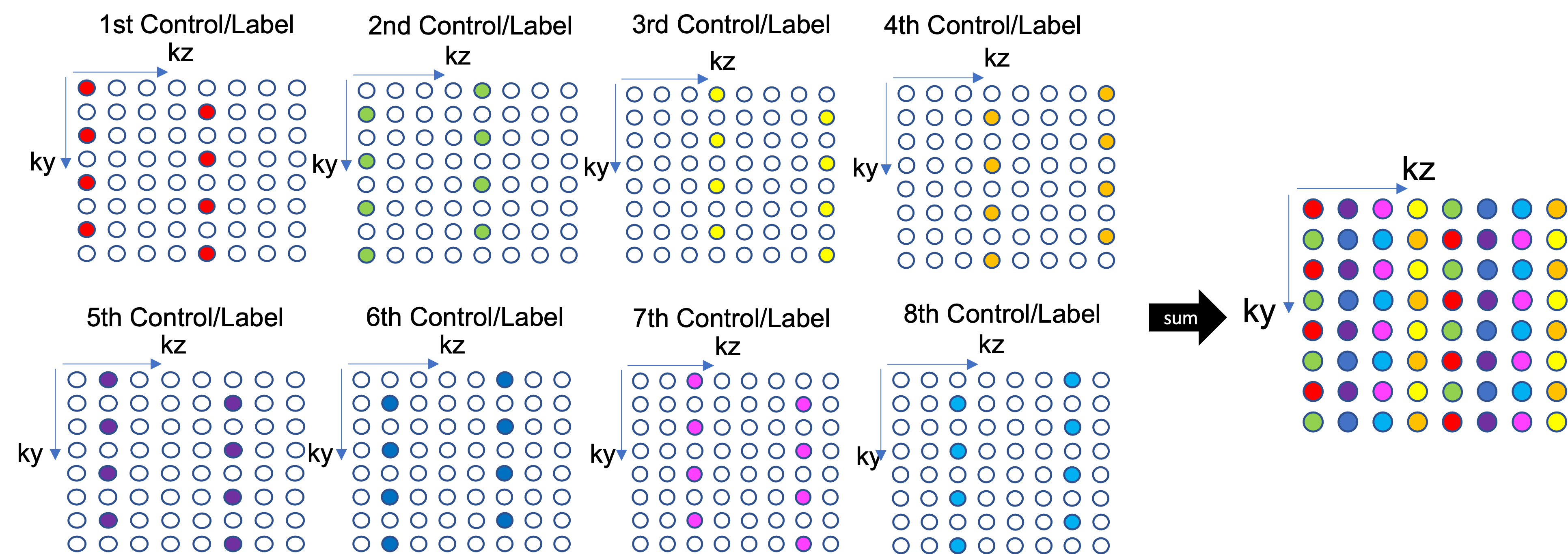
Imaging ProtocolFigure 1 shows the under-sampling pattern of image acquisition. A time dependent 2D-CAIPIRINHA sampling4 along with 3D GRASE readout was applied with the acceleration factor of 2 in the phase encoding (y) direction and 4 in the slice partition (z) direction to allow single shot acquisition of 3D volume. The imaging protocol is shown as follows: TR = 6180ms, TE = 52.5ms, labeling duration = 1500ms and 5 post-labeling delays (600, 1000, 1400, 1800 and 2200ms), which was used with 8 control/label pairs for each PLD. Background suppression with 2 inversion pulses was used and optimized for each PLD. The resolution was 2mm isotropic, matrix size of 96×96×48. The total scan time was 8 minutes and 33 seconds.
Reconstruction and Quantification
A spatio-temporal TGV constrained reconstruction5 was applied to the raw data for each PLD. The reconstruction solves the following optimization equation:
$$
\begin{gathered}\left(c^{\star}, l^{\star}\right) \in \underset{c, l}{\operatorname{argmin}} \frac{\lambda_c}{2}\left\|K c-d_c\right\|_2^2+\frac{\lambda_l}{2}\left\|K l-d_l\right\|_2^2+\gamma_1(w) T G V_{a_1, a_0, \beta}(l) \\+\gamma_1(w) T G V_{a_1, a_0, \beta}(c)+\gamma_2(w) T G V_{\alpha_1, a_0, \beta}(c-l)\end{gathered}
$$
where $$$c$$$ and $$$l$$$ are control and label images, $$$K$$$ is the forward encoding matrix, $$$d$$$ is acquired k space data, $$$\alpha_{1}$$$ , $$$\alpha_{2}$$$ and $$$\beta$$$ are TGV reconstruction parameters and $$$\gamma_{1}(w)$$$, $$$\gamma_{2}(w)$$$ are the weights to balance control, label, and perfusion images. The suggested values of these parameters according to5 were used in this study. 8 control and label images were constructed for each PLD, and the perfusion images were calculated by subtraction of control and label images and then averaged. In comparison, we combined the 8 CAIPI segments to form a complete k-space (shown in Figure 1) and reconstruct the image with conventional inverse Fourier Transform to compare with the TGV reconstruction. M0 image is fitted from the mean control images of 5 PLDs according to the theoretical model for different background suppression timings. CBF and ATT maps were fitted from the multi-delay perfusion images and M0 image using the kinetic model. Blood T1 values were corrected for age and sex of each subject according to the model proposed by6. The brain mask was segmented from the structure image and coregistered to the M0 image. Global CBF and ATT values were calculated as the mean value of CBF and ATT maps within the brain masks.
In vivo experiments
19 typically developing children within the age of 9-17 years (7 males) were recruited under IRB approval. All children were scanned twice with two weeks apart for test-retest purposes on a 3T SIEMENS Prisma scanner and 32-channel head coil. The multi-delay ASL images were acquired with the proposed scheme, along with T1w MPRAGE scan. Global CBF and ATT were calculated with the aforementioned method and intra-class correlation coefficient (ICC) was calculated between the two visits for reproducibility.
Results
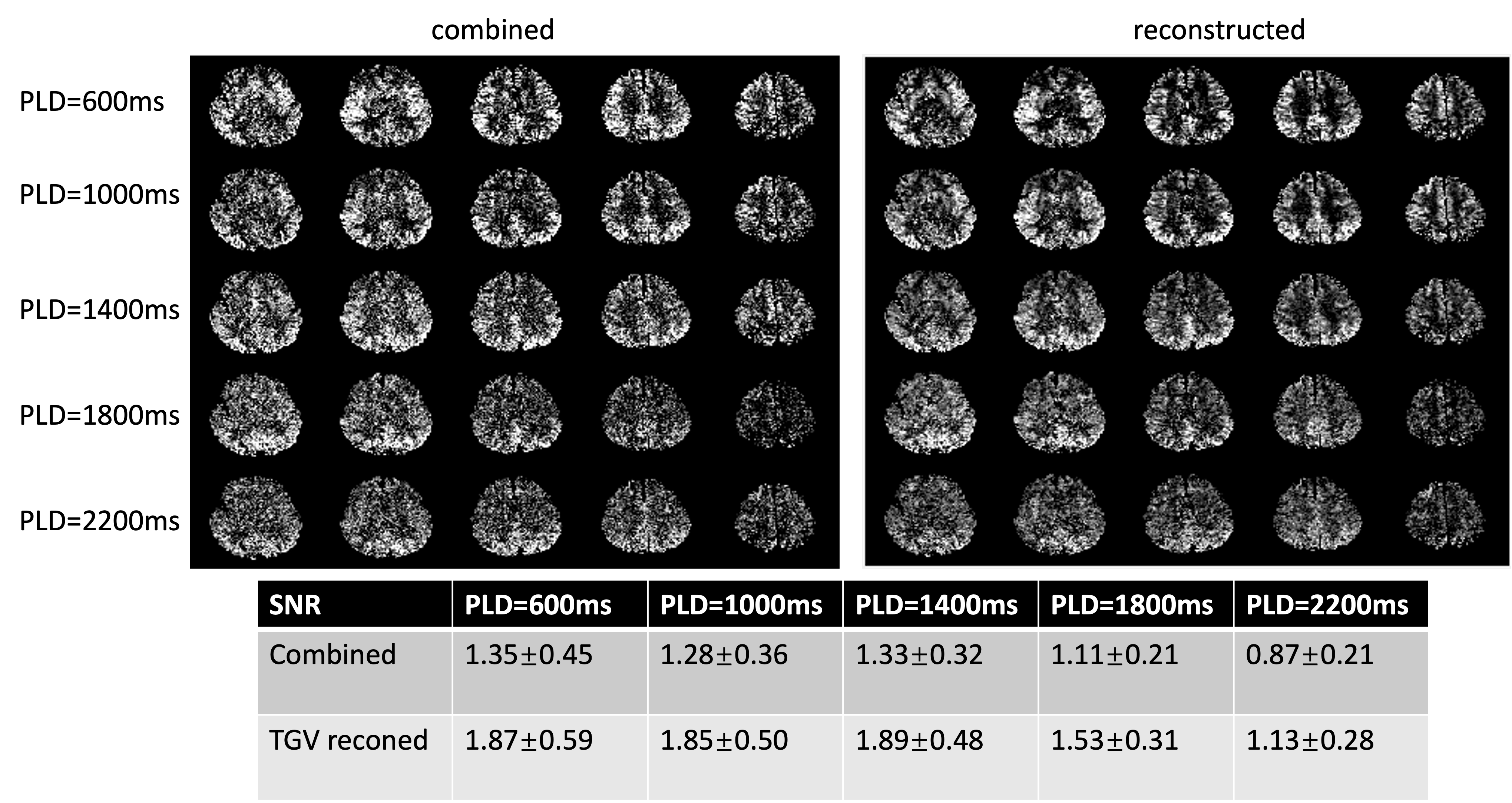
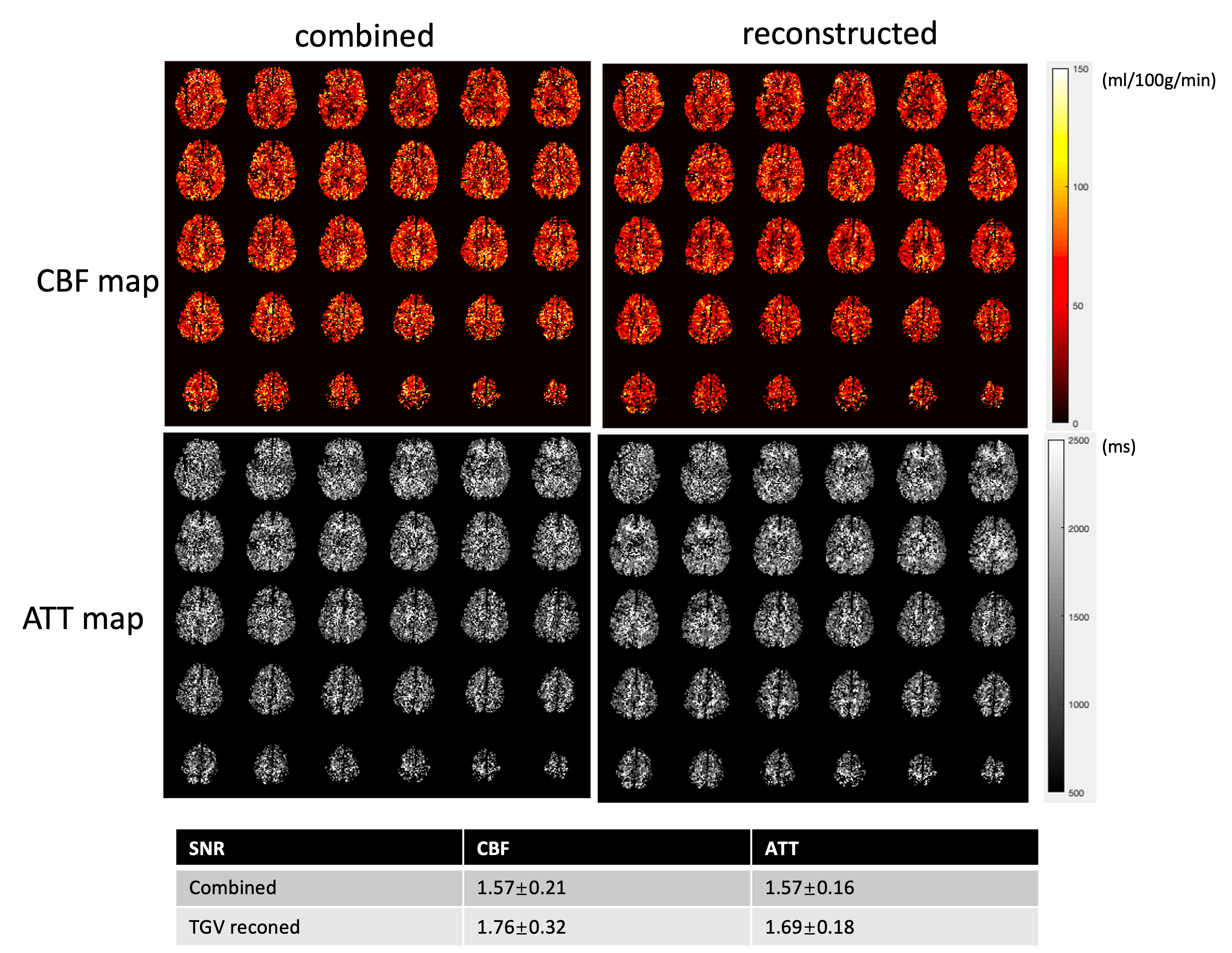
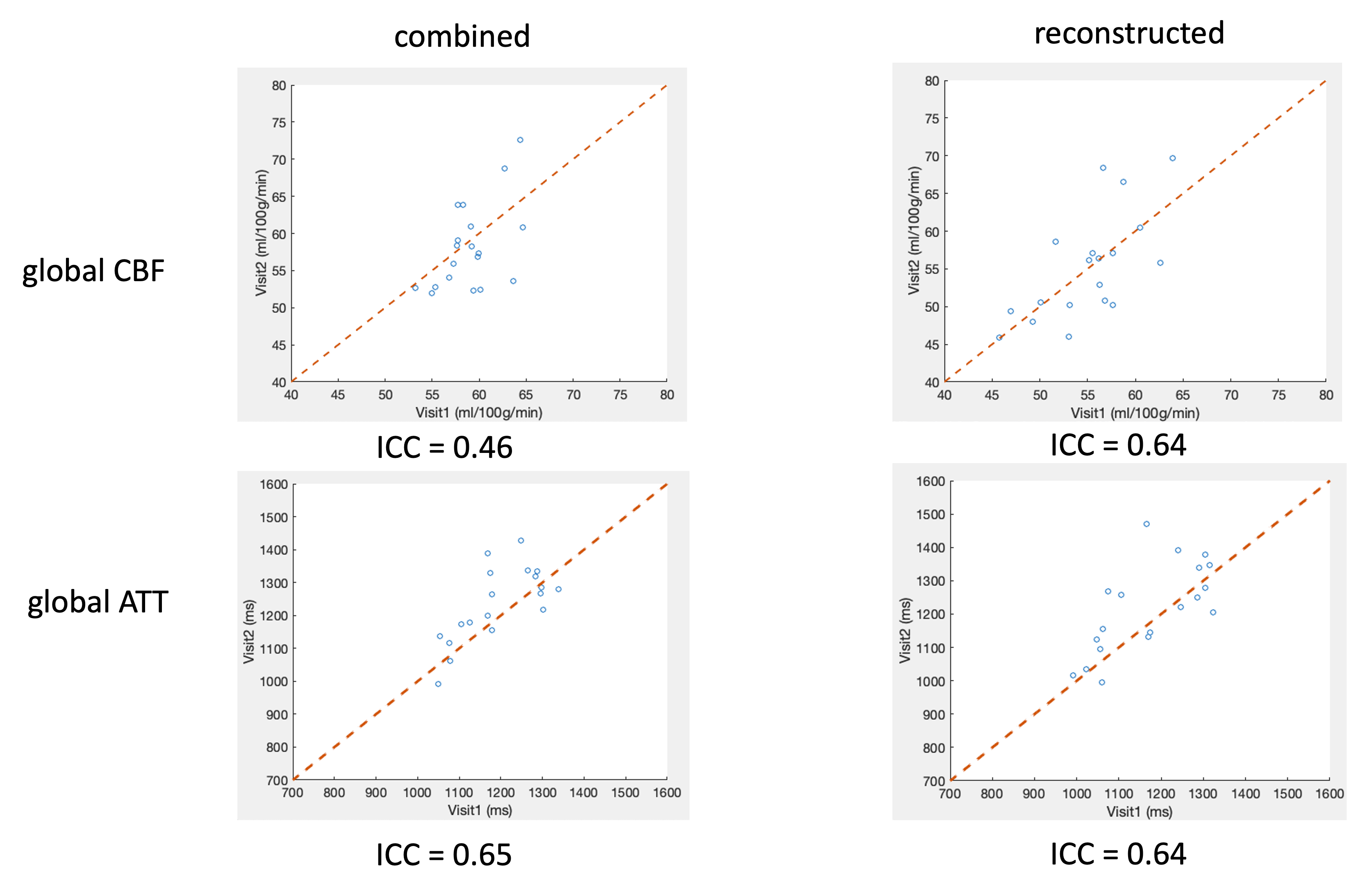
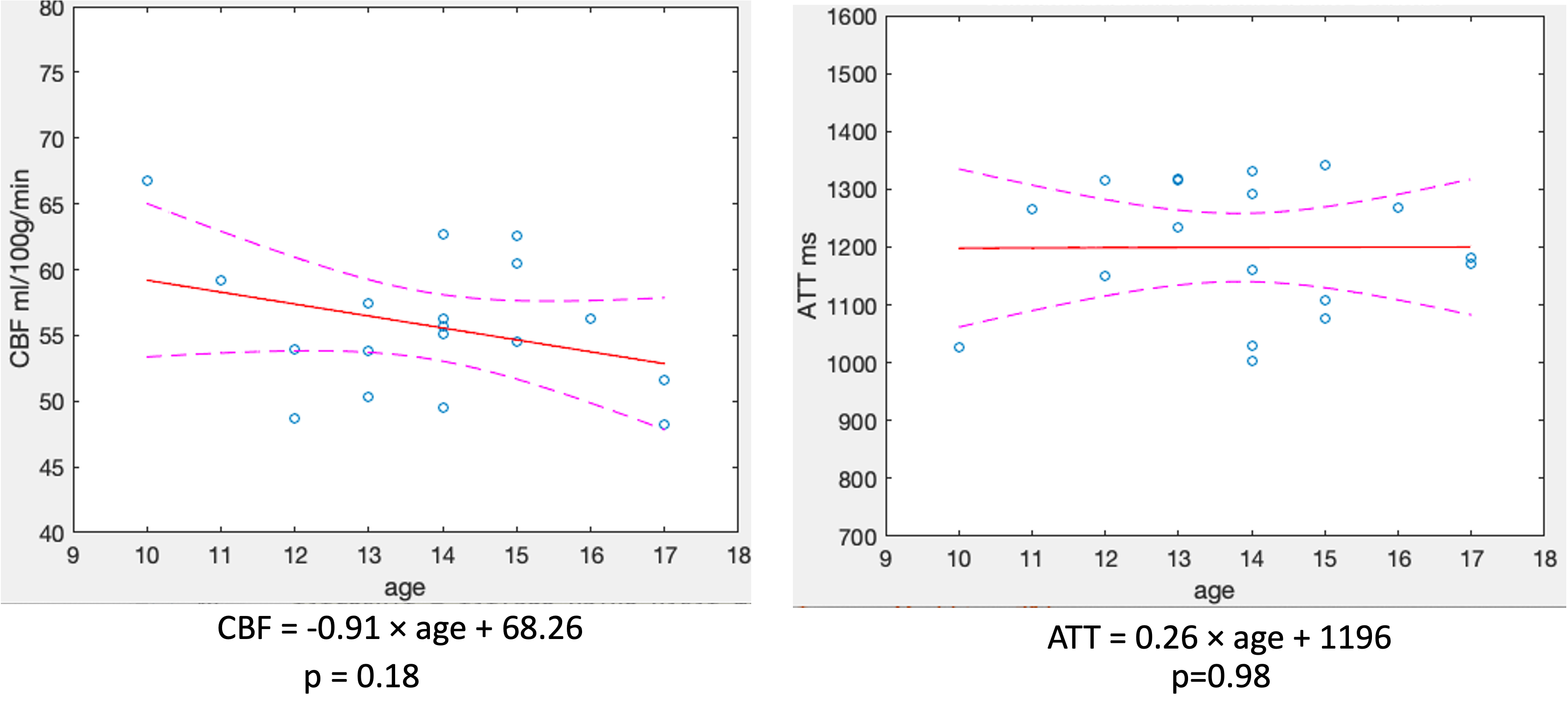
Figure 2 shows the combined and the TGV reconstructed perfusion images for the 5 PLDs. The perfusion images with TGV reconstruction have higher SNR compared to the standard combined method in all 5 PLDs. Figure 3 shows the CBF and ATT maps fitted from the multi-delay perfusion images. The CBF map and ATT map from the TGV reconstruction have higher SNR (12% and 7.6% higher) and gray and white matter contrast compared to the combined method. Figure 4 shows the test-retest performance of global CBF and ATT for both methods. TGV reconstruction improved ICC from 0.46 to 0.65 for global CBF, while ICC was comparable with the combined method for global ATT. Figure 5 shows the correlation of CBF and ATT with age. CBF shows a negative trend with age, while ATT does not vary with age.Discussion and Conclusion
In this work, we developed a high-resolution multi-delay 3D pCASL scheme to achieve whole brain isotropic 2mm CBF and ATT mapping within 9 minutes. With TGV reconstruction, high-resolution perfusion images can be achieved with adequate SNR. This improved the test-retest repeatability and potentially can improve the accuracy for CBF quantification in typically developing children. We achieved an ICC of 0.65 for global CBF, which is consistent with previous studies in children1, nevertheless our imaging protocol has much higher resolution and 5 PLDs. This shows the potential to use multi-delay ASL for neurodevelopmental studies.Acknowledgements
No acknowledgement found.References
[1] Jain, Varsha, et al. "Longitudinal reproducibility and accuracy of pseudo-continuous arterial spin–labeled perfusion MR imaging in typically developing children." Radiology 263.2 (2012): 527.
[2] Satterthwaite, Theodore D., et al. "Impact of puberty on the evolution of cerebral perfusion during adolescence." Proceedings of the National Academy of Sciences 111.23 (2014): 8643-8648.
[3] Wang, Danny JJ, et al. "Multi-delay multi-parametric arterial spin-labeled perfusion MRI in acute ischemic stroke—comparison with dynamic susceptibility contrast enhanced perfusion imaging." NeuroImage: Clinical 3 (2013): 1-7.
[4] Breuer, Felix A., et al. "Controlled aliasing in volumetric parallel imaging (2D CAIPIRINHA)." Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 55.3 (2006): 549-556.
[5] Spann, Stefan M., et al. "Robust single-shot acquisition of high resolution whole brain ASL images by combining time-dependent 2D CAPIRINHA sampling with spatio-temporal TGV reconstruction." NeuroImage 206 (2020): 116337.
[6] Wu, Wen‐Chau, et al. "In vivo venous blood T1 measurement using inversion recovery true‐FISP in children and adults." Magnetic resonance in medicine 64.4 (2010): 1140-1147.
Figures