2735
Optimizing Breast Isotropic DCE-MRI Imaging Based on Compressed SENSE Technique
Ning Ning1, Lina ZHANG1, Zhuo WANG1, Qi WU1, Hongbing LIANG1, Qingwei SONG1, Ailian LIU1, and Yiming Wang2
1First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Clinical and Technical Support,PhilipsHealthcare, Shanghai, China
1First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Clinical and Technical Support,PhilipsHealthcare, Shanghai, China
Synopsis
Keywords: Breast, Breast
Dynamic contrast-enhanced (DCE) MRI is a multi-phase sequence that is limited by long scan times, which makes acquisition acceleration necessary to accomplish clinical feasibility. The aim of this study was to investigate the effect of different Acceleration Factors (AFs) on the image quality of isotropic DCE-MRI acquired with the Compressed SENSE (CS) technique, and to find the optimal AF for the isotropic DCE-MRI.CS factors of 4 to 7 were compared against the conventional SENSE technique in 43 patients. Preliminary results show a CS factor of 5 is the optimal AF with optimized image and velocity data quality.Introduction
In today's world, breast cancer has become the most prevalent malignancy in women worldwide and is an important cause of death in women [1]. Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) is a technique that assesses tumor perfusion and vascular permeability by the injection of exogenous contrast agent, which is of great value in the qualitative diagnosis of breast tumors[2,3]. DCE-MRI requires high temporal and spatial resolution because lower spatial resolution limits morphological observation and interpretation and poor temporal resolution may affect the proper analysis of quantitative breast parameters[4]. However, these two are usually mutually constrained, so finding a balance between them is a difficult task for the clinical applications of DCE-MRI imaging. Recently, the Compressed sense (CS) technique has been widely reported to further reduce the scan time while maintaining high spatial resolution by employing image sparsity and noncoherent K-space sampling during data acquisition[5]. However, if improperly used or the acceleration factor (AF) is blindly increased, parallel imaging-related artifacts can be generated, resulting in blurred images and affecting the diagnosis. To improve the clinical feasibility of DCE-MRI, this study evaluates the applicability of CS acceleration for DCE-MRI. Therefore, acquisitions with different CS acceleration factors were compared with the conventional acquisition method using SENSE parallel imaging, and an optimal AF was determined.Methods
A total of 43 patients (mean age: 49.78 ± 9.83, range: 31-69 years) were recruited, with written informed consent acquired from each subject. All patients were scanned using a 3.0 T MR scanner (Ingenia CX, Philips Healthcare, Best, the Netherlands) with a seven-channel bilateral phase-array breast coil. The sequence optimization was performed on the delayed e-THRIVE sequence (shown in Table 1). Table1: Sequence parameter table between different groups Images were reconstructed on the scanner by the vendor-supplied software package (Compressed SENSE, Philips Healthcare). All image post-processing was performed off-line using GTFlow (Gyrotools LLC, Zurich, Switzerland). After image reconstruction, two radiologists performed subjective independent scoring based on considerations of the clarity of the breast gland, display of the lesion, image artifacts and fat suppression effect. Five-point scoring criteria of image quality were used (the scoring system listed in Table 2), and a score greater than 3 was considered to meet the clinical requirements. For quantitative data, the slice with the largest area of abnormal enhancement tumors was selected on the DCE-MRI images. The mean signal intensity (SI) and noise (SD) within regions of interest (ROIs) covering tumors, contralateral fibroglandulars and ipsilateral pectoralis major muscles respectively were independently measured three times for each AF group , and the mean value of three measurements was recorded (Fig 1). The ROIs are sized 20-25mm2 and were drawn avoiding fat, blood vessels, air and other tissues. Kappa test was used for subjective score consistency analysis between the two observers. The Shpiro-Wilk test was used to analyze the normality of the data. The Friedman test was used to compare the objective evaluations and subjective scores among groups, and data with differences were selected for two-way comparisons (P values corrected by Bonferroni). p < 0.05 was considered statistically significant.Results
The subjective scores of image quality were consistent between the two observers (kappa = 0.831), and there were significant differences in SNRfibroglandular, CNRfibroglandular, SNRlump and CNRlump among different acceleration factors (P < 0.05). There were no significant differences in RCfibroglandulars-to-lump, RClump-to-muscle and RCfibroglandulars-to-muscle among different acceleration factors (P>0.05). The results of pairwise comparison showed that the SNRfibroglandular, CNRfibroglandular, SNRlump , CNRlump and subjective scores of images acquired with 4-fold-accelerated SENSE, 4-fold-accelerated CS and 5-fold-accelerated CS were higher than those of images acquired with 6-fold-accelerated CS and 7-fold-accelerated CS (P <0.05), indicating that 5-fold-accelerated CS can achieve the fastest scanning without compromising image quality. See Table 3 and Table 4 for details.Discussion
Compressed SENSE provides better acceleration and better delineation of image details than the traditional parallel imaging methods such as SENSE, and it is beneficial for breast tumor imaging, and the display of mammary glands, arteries, veins and other mammary glands. In order to obtain a reliable assessment of tumor morphology and hemodynamics, this study proposes a combination of breast DCE-MRI and rapid imaging technology to achieve a balance between the two by finding an optimal acceleration factor for CS. This enables simultaneous and accurate assessment of lesion morphology, lesion and enhancement kinetics, with optimized sensitivity and specificity.Conclusion
During clinical practice, considering the scanning time and image quality, an acceleration factor of 5 for CS is recommended for breast Isotropic DCE-MRI (Delayed e-THRIVE) sequence, which saves 26.7% of scanning time compared with conventional parallel imaging. The optimized Isotropic Dynamic Contrast-Enhanced MRI (DCE-MRI) sequence (CS with AF = 5) not only ensures the image quality, but also shortens the scanning time, which is beneficial to the display of breast tumors, arteries, veins and other breast tissues, and has good prospect and value for better clinical application.Acknowledgements
NoneReferences
[1] Sung H, Ferlay J, Siegel R L, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin, 2021, 71(3): 209-249. [2] Kang S R, Kim H W, Kim H S. Evaluating the Relationship Between Dynamic Contrast-Enhanced MRI (DCE-MRI) Parameters and Pathological Characteristics in Breast Cancer. J Magn Reson Imaging, 2020, 52(5): 1360-1373. [3] Cheng Q, Huang J, Liang J, et al. The Diagnostic Performance of DCE-MRI in Evaluating the Pathological Response to Neoadjuvant Chemotherapy in Breast Cancer: A Meta-Analysis. Front Oncol, 2020, 10: 93. [4] Leithner D, Moy L, Morris E A, et al. Abbreviated MRI of the Breast: Does It Provide Value?. J Magn Reson Imaging, 2019, 49(7): e85-e100. [5] Delattre B M A, Boudabbous S, Hansen C, et al. Compressed sensing MRI of different organs: ready for clinical daily practice?. Eur Radiol, 2020, 30(1): 308-319.Figures
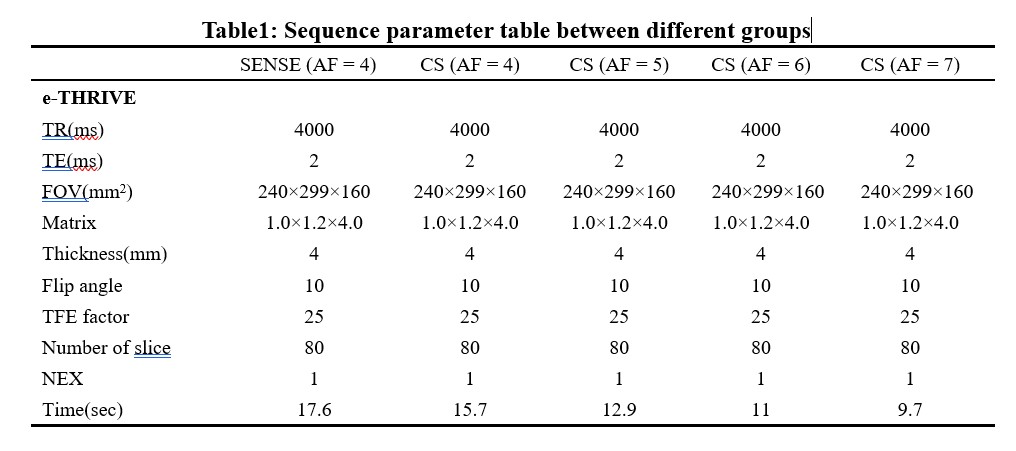
Table1: Sequence parameter table between different
groups
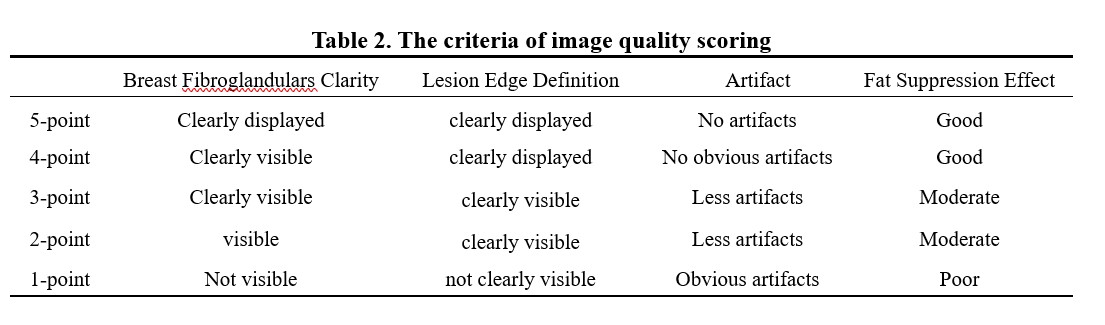
Table 2. The criteria of image quality scoring
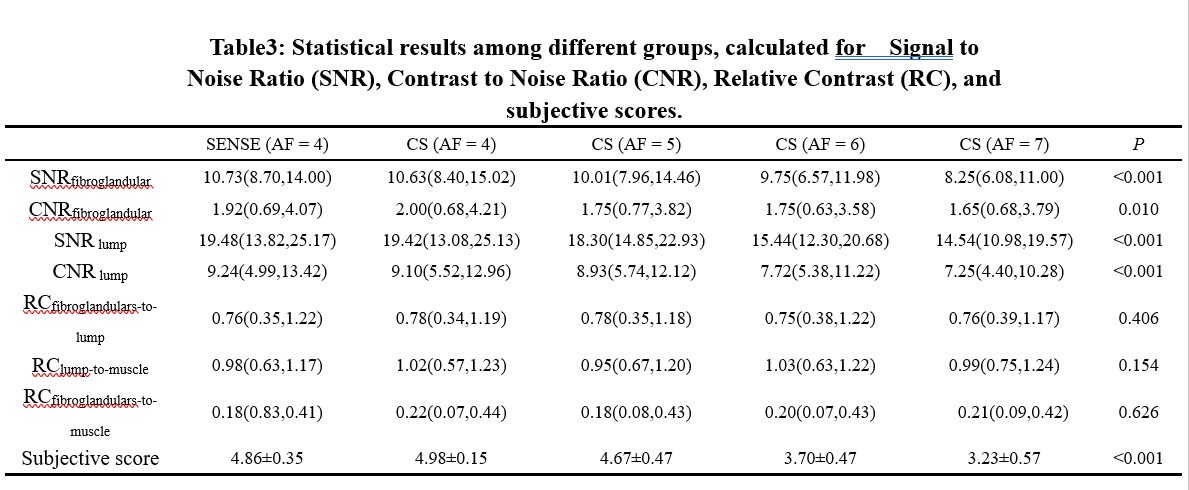
Table3: Statistical results among different groups,
calculated for Signal to Noise Ratio (SNR),
Contrast to Noise Ratio (CNR), Relative Contrast (RC), and subjective scores.
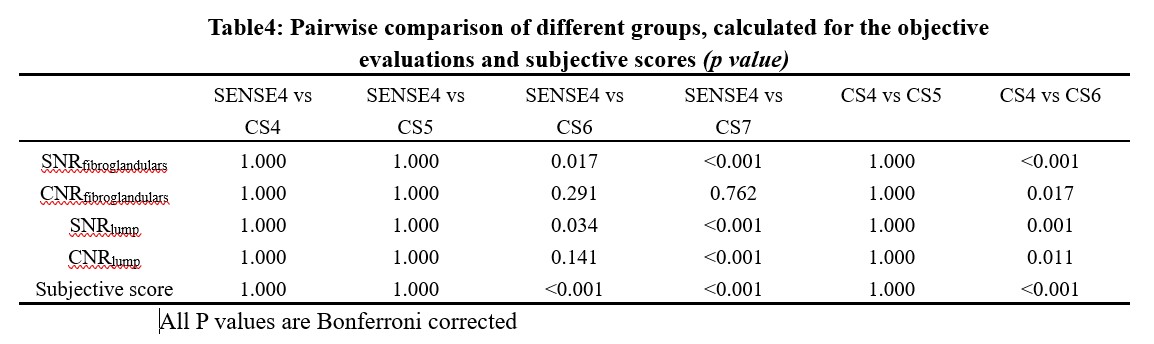
Table4: Pairwise comparison of different groups,
calculated for the objective evaluations and subjective scores (p value)

Figure1.(A) The picture shows a
schematic diagram of ROI placement, with ROI placed in the contralateral breast
fibroglandulars (R1), lump (R2) and ipsilateral pectoralis major muscle(R3),
respectively.(B-G)pictures for A 58-year-old female diagnosed with infiltrating
ductal carcinoma grade 2.(B-F) Images of DCE-MRI (e-THRIVE) SENSE with AF = 4,
CS with AF=4, 5, 6, and 7 respectively.(G) The picture shows that the time
signal intensity curve(TIC) is platform type.
DOI: https://doi.org/10.58530/2023/2735