2731
Added Value of Quantitative DCE-MRI in Prediction of Breast Cancer Recurrence Following Neoadjuvant Chemotherapy?1Hematology and Oncology, Oregon Health and Science University, Portland, OR, United States, 2Biostatistics Shared Resource, Oregon Health and Science University, Portland, OR, United States, 3Medicine, Oregon Health and Science University, Portland, OR, United States, 4Radiology, Oregon Health and Science University, Portland, OR, United States, 5Advanced Imaging Research Center, Oregon Health and Science University, Portland, OR, United States
Synopsis
Keywords: Breast, Cancer
Breast cancer patients treated with neoadjuvant chemotherapy (NACT) are at risk of recurrence depending on clinicopathological characteristics. This preliminary study aimed to investigate the predictive performances of quantitative dynamic contrast-enhanced (DCE) MRI parameters, alone and in combination with clinicopathological variables, for prediction of recurrence in patients treated with NACT.
Pre- and post-NACT DCE-MRI parameters performed better than tumor size measurement in prediction of recurrence, whether alone or in combination with clinicopathological variables. Combining post-NACT Ktrans with residual cancer burden and age showed the best improvement in predictive performance with ROC AUC = 0.965.
Introduction
Breast cancer patients treated with neoadjuvant chemotherapy (NACT) are at risk of recurrence depending on clinicopathological characteristics, including residual cancer burden (RCB).[1] Accurate identification of patients at high risk of recurrence post NACT may help select for appropriate treatment escalation and de-escalation strategies to improve outcomes. However, prediction of recurrence by clinicopathological characteristics alone is not satisfactory. [2,3] Further, pathologic response status such as RCB can only be assessed after NACT completion and surgery, precluding opportunities to adjust therapy regimen in the NACT setting to lower the recurrence risks. The aim of this study is to investigate the predictive performances of quantitative dynamic contrast-enhanced (DCE) MRI parameters pre- and post-NACT, alone and in combination with clinicopathological variables, for prediction of recurrence in patients treated with NACT.Methods
47 breast cancer patients treated with standard of care (SoC) NACT were consented to a longitudinal research DCE-MRI study, where they underwent DCE-MRI at visit 1 (V1) - before NACT, V2 - after first NACT cycle, V3 – midpoint of NACT, and V4 - after NACT completion but prior to surgery. Clinicopathological variables including RCB, tumor type, tumor grade, ER, PR, and HER2 status, clinical nodal disease, stage, and age were collected from the electronic medical records. Axial bilateral and full-coverage breast DCE-MRI was performed using a 3T Siemens system, achieving high spatiotemporal resolution of 14-18 s temporal resolution and 1x1x1.4 mm3 voxel size using the TWIST sequence.[4] Tumor regions of interest (ROIs) were manually drawn and the longest diameter (LD) was measured according to the RECIST guidelines. [5] Within the ROIs, the voxel DCE time-course data were fitted with the Shutter-Speed pharmacokinetic model (SSM) [6] to extract the Ktrans, ve, kep (= Ktrans/ve), and τi (mean intracellular water lifetime) parameters. The tumor mean parameter value was calculated by averaging the voxel parameter values. For data analysis, only the V1 and V4 metrics were used to align with the current SoC practice of only performing pre- and post-NACT MRI. RCB was determined from the post-NACT resection specimens. [7]T-test was used to compare means of continuous variables between the recurrence and non-recurrence groups. Univariate logistic regression (ULR) C statistics value, equivalent to ROC AUC, was reported for each MRI metric for prediction of recurrence. Firth logistic regression (FLR) was used to build multivariate prediction models for recurrence. Clinicopathological variables with a p-value < 0.2 from the univariate analysis were used to build the initial FLR model, followed by an automated stepwise model selection procedure to select the final model which included RCB and age only. Then, MRI parameters were added to this model one at a time to examine the predictive performance presented as ROC AUC. Wald p-values were calculated to evaluate the significance of contribution by the MRI metrics. Five-fold cross validation was performed to obtain cross-validated (cv) ROC AUC. In addition, the first principal component (PC1) of all MRI metrics was used to examine the added value of multiple MRI metrics in predictive performance.
Results
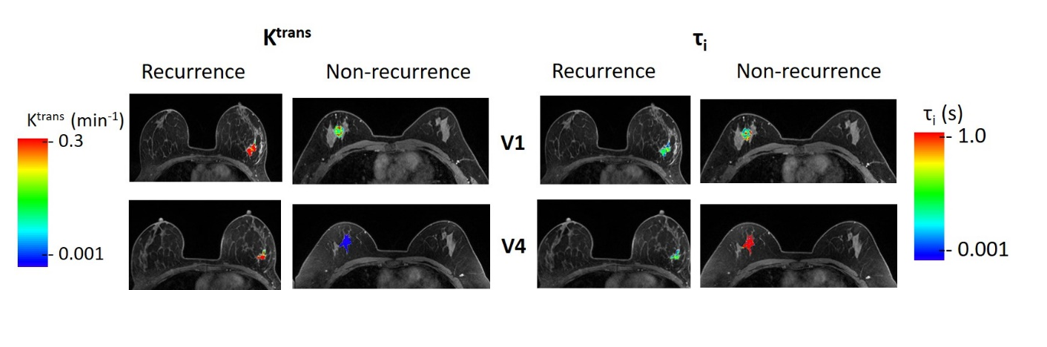
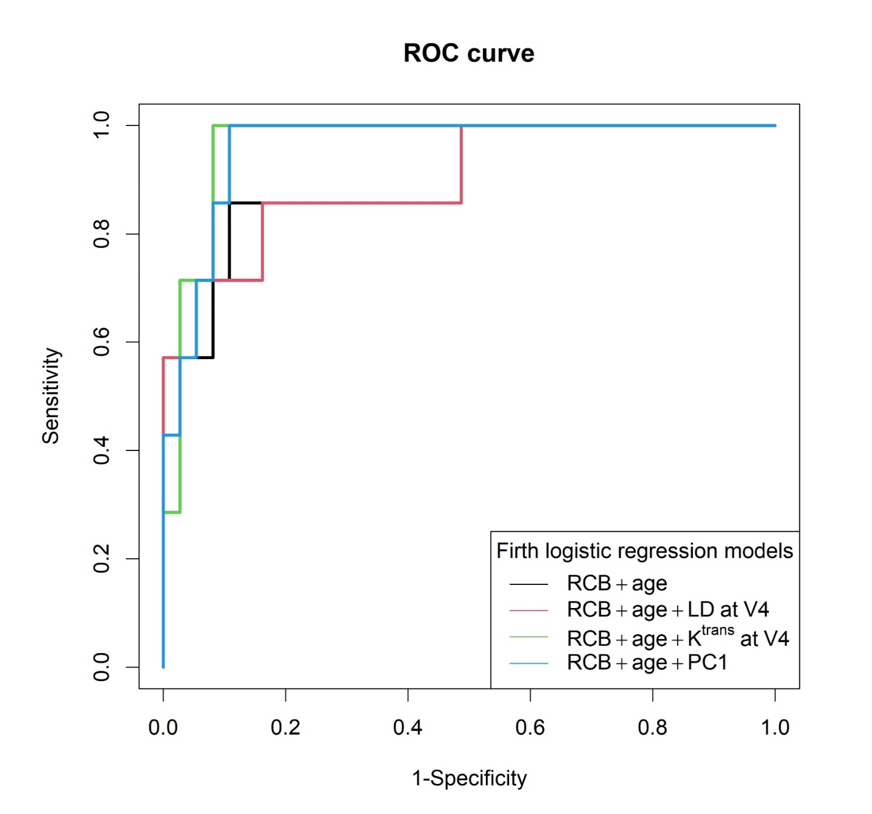
7 out of the 47 patients experienced recurrence. Mean and SD values for the two groups, t-test p-values, and ULR C values (with 95% CI) are summarized in Table 1 for each MRI metric at V1 and V4, and the percent change of V4 relative to V1 (V4_1%). For prediction of recurrence, only V1 Ktrans and V4 LD, Ktrans, kep, and τi showed C > 0.7 with V4 Ktrans having the largest C value of 0.812. Figure 1 shows tumor Ktrans and τi parametric maps for a patient with recurrence and a patient without recurrence at V1 and V4. The latter showed substantially larger changes in DCE parameters from V1 to V4 (decreases in Ktrans and increases in τi) compared to the former. Table 2 shows ROC AUC (with 95% CI) and cv ROC AUC values for prediction of recurrence when using clinicopathological variables of RCB and age only, combining RCB and age with a single MRI metric, and with PC1 of all MRI metrics. While adding LD to RCB and age did not improve predictive performance, the addition of each DCE-MRI parameter (except for V4_1% of τi) or PC1 improved predictive accuracy with AUCs > 0.900, with addition of V4 Ktrans showing the largest improvement from AUC = 0.900 to 0.965. Representative results from Table 2 are shown as ROC curves in Figure 2.Discussion and Conclusion
This preliminary study shows that quantitative DCE-MRI parameters outperform tumor size measurement in prediction of breast cancer recurrence following NACT, whether alone or in combination with clinicopathological variables. The predictive accuracy by pre-NACT Ktrans alone shown in this study may potentially help guide adjustment of NACT regimen to reduce recurrence risk and improve survival outcome. The improvement in predictive performance when combining DCE-MRI parameters with clinicopathological variables demonstrate the potential added value of quantitative DCE-MRI in prediction of recurrence. This study is limited by the cohort size which precludes analysis stratified by breast cancer subtypes and is the likely reason for lack of statistical significance in predictive performance improvement when adding DCE parameters to clinicopathological variables (as shown by Wald p-values). Therefore, validation with a larger cohort is warranted.Acknowledgements
Grant support: NIH R01 CA248192References
1. Caudle, A. S. et al. Local-regional control according to surrogate markers of breast cancer subtypes and response to neoadjuvant chemotherapy in breast cancer patients undergoing breast conserving therapy. Breast Cancer Res. 14, R83 (2012).
2. Asselain, B. et al. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 19, 27–39 (2018).
3. Chou, H.-H. et al. Factors affecting locoregional recurrence in breast cancer patients undergoing surgery following neoadjuvant treatment. BMC Surg. 21, 160 (2021).
4. Tudorica, A. et al. Early Prediction and Evaluation of Breast Cancer Response to Neoadjuvant Chemotherapy Using Quantitative DCE-MRI. Transl. Oncol. 9, 8–17 (2016).
5. Eisenhauer, E. A. et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur. J. Cancer Oxf. Engl. 1990 45, 228–247 (2009).
6. Springer, C. S. et al. Intratumor mapping of intracellular water lifetime: metabolic images of breast cancer? NMR Biomed. 27, 760–773 (2014).
7. Symmans, W. F. et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 25, 4414–4422 (2007).
Figures
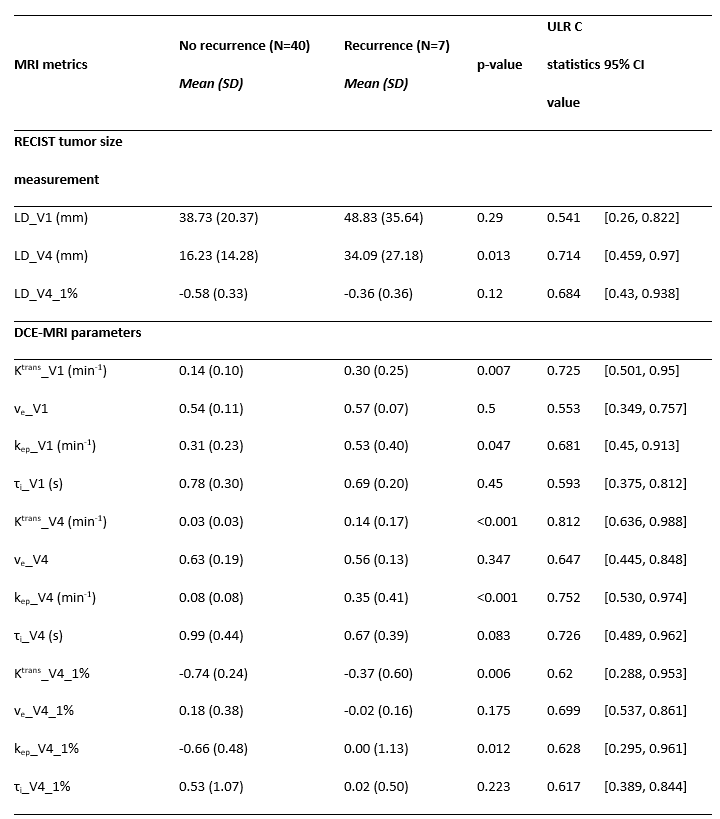
Table 1 - MRI Metrics for prediction of breast cancer recurrence
(ULR - Univariable logistic regression, 95% CI – 95% confidence interval for the C value, LD – Longest diameter, V1 – Visit 1 (pre-NACT MRI), V4 – Visit 4 (post NACT, pre-surgery MRI), V4_1% - corresponding percent changes (V4 relative to V1)
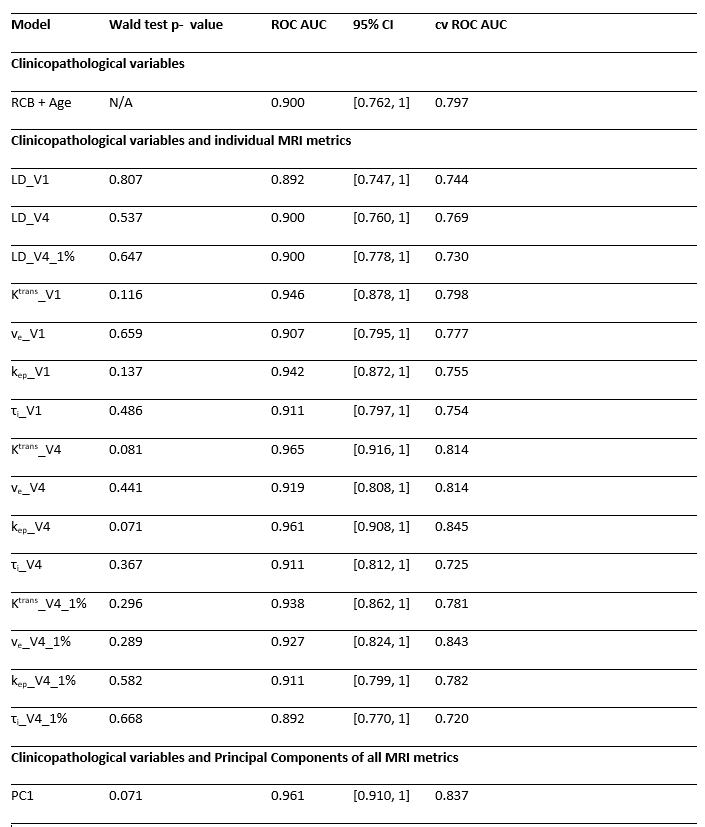
Table 2 - Predictive Performances for Recurrence Using Clinicopathological Variables Only and Combinations of Clinicopathological Variables and MRI Metrics.
(ROC AUC - area under the receiver operating characteristic curve, 95% CI – 95% confidence interval for ROC AUC, cv – cross validated, N/A – not applicable, LD – Longest diameter, V1 – Visit 1 (pre-NACT MRI), V4 – Visit 4 (post NACT, pre-surgery MRI), V4_1% - corresponding percent changes (V4 relative to V1), PC1 – first principal components of all MRI metrics)