2730
Comparison of DWI score and Kinetic score as a Prognostic Marker in Breast Cancer Patients receiving Neoadjuvant Systemic Treatment.1Department of Radiology, Tenri Hospital, Nara, Japan, 2Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University graduate school of medicine, Kyoto, Japan, 3Department of Diagnostic Radiology, Kansai Electric Power Hospital, Osaka, Japan, 4Department of Diagnostic Pathology, Kyoto University Hospital, Kyoto, Japan, 5Department of Breast Surgery, Kyoto University Hospital, Kyoto, Japan
Synopsis
Keywords: Breast, Cancer, disease-free survival
This study aimed to investigate the association of DWI score of breast cancer derived from MRI obtained after neoadjuvant systemic treatment (NST) with disease-free survival (DFS). Kinetic score from standard DCE-MRI at the same timing was analyzed for comparison. Kaplan-Meier analysis showed that patients with DWI score of 2 showed significantly shorter DFS than those with DWI score 0 or 1. Patients with kinetic score of 2 or 3 showed significantly shorter DFS than those with kinetic score of 0 or 1. DWI score demonstrated excellent inter-reader agreement and is suitable for predicting prognosis of breast cancer patients after NST.Purpose:
Neoadjuvant systemic treatment (NST) is commonly and increasingly used for women with locally advanced breast cancer. Residual cancer burden after NST is linked to the long-term prognosis [1]. We have previously developed a visual score based on diffusion-weighted image (DWI score) for evaluating residual tumors after NST [2]. Based on the above-mentioned evidence, we hypothesized that the score might be linked to the long-term prognosis of the patients. Therefore, we aimed to investigate if the DWI score of the post-NST breast cancer was associated with disease-free survival (DFS). Dynamic contrast-enhanced (DCE)-based kinetic score after NST was also investigated as a comparison.Methods and Materials:
Study population:All breast cancer patients who received NST, who underwent breast MRI including DWI after completion of the treatment, followed by surgery between October 2014 and May 2019 were included.
MRI protocol:
MRI was acquired using a 3T MRI scanner (Prisma/Trio; Siemens Healthineers, Erlangen, Germany) and a 16 or 18-channel dedicated breast coil. MR images were obtained using routine protocols sequence: T1WI, T2WI, DWI (axial single-shot EPI; TR/TE, 6300-7000/50-62ms; pixel size 2x2x3 mm; NEX, 3; b=0, 1000sec/mm2), and DCE-MRI (pre, 1-2, 5-6 min post-contrast; axial VIBE with fat suppression; TR/TE, 3.8/1.4ms; 0.9x 0.9x1 mm).
Image analysis:
On DWI, the target lesion was evaluated and scored using a three-point scale: 2, obvious high signal intensity; 1, intermediate signal intensity in a scar-like shape; and 0, no abnormal signal intensity (Figure 1). On DCE-MRI, kinetic patterns of the lesions were evaluated based on BI-RADS and were scored as 3: washout, 2: plateau, 1: persistent, and 0: no enhancement (Figure 2). Two experienced breast radiologists independently evaluated both scores with two-months’ interval between DWI and DCE evaluation, with a reference to baseline breast MRI only.
Statistical analysis:
The agreement of DWI or kinetic scores between the two radiologists was evaluated using Kappa statistics. Survival analyses were performed for disease-free survival using Kaplan-Meier method and Univariate Cox proportional hazards models. Statistical analysis was performed using MedCalc Software (Mariakierke, Belgium)
Results:
A total of 97 patients (mean age 50.4 years) with 32 triple-negative, 14 HER2 positive, 22 luminal-HER2, and 29 luminal subtypes were included. Among them, 47 achieved pathological complete response (pCR) on surgery and 16 developed recurrence/distant metastasis. Median DFS was 4.7 years (range, 0.17-7.58 years). On pre-surgical evaluation, lesions were categorized as DWI scores of 2 (n=47), 1 (9), and 0 (41) by reader 1, and 2 (46), 1 (10), and 0 (41) by reader 2, respectively.On DCE-MRI, the lesions were categorized as kinetic scores of 3 (34), 2 (15),1 (31), and 0 (17), by reader 1, 3 (32), 2 (9),1 (35), and 0 (21) by reader 2, respectively. The weighted kappa value of DWI score between readers was 0.93, while that of kinetic score was 0.80.
Survival analyses were shown in Kaplan-Meier survival curve (Figures 3, 4). Cox proportional hazards analysis showed that patients with DWI score of 2 showed significantly shorter DFS compared to those with DWI score 0 or 1 (Reader 1; Hazard radio (HR) 16.1: 95% Confidence interval (CI) 5.7-45.5, p<0.001/ Reader 2; HR 16.7: 95% CI 5.8-47.3, p<0.001). On DCE, patients with kinetic score of 2 or 3 showed significantly shorter DFS compared to those with kinetic score of 0 or 1 (Reader 1; HR 7.07: 95% CI 1.7-29.4, p=0.017/ Reader 2; HR 7.5: 95% CI 1.2-47.8, p=0.059). Cox regression analysis revealed a significantly higher risk of recurrence or metastasis for women with DWI score of 2 compared to those with scores of 0 and 1, and kinetic score of 3 compared to those with scores of 0, 1 and 2, respectively. Results were similar for scores by both readers.
Discussions and Conclusions:
DWI-based visual score and kinetic score showed similar diagnostic performances. Several studies demonstrated that changes in the ADC measured from DWI of pre-treatment and post-treatment MRI were predictive of pCR in patients with breast cancer who received neoadjuvant chemotherapy [3]. However, evaluations based on ADC values require a sufficiently large lesion size for reliable ADC measurement, which is often difficult to perform in case of small or irregular-shape lesions demonstrating dendritic shrinkage patterns after NST. In this context, DWI score based on visual assessment of DWI may be a more feasible option for predicting prognosis, as well as estimating disease extent [2]. In spite of visual assessment, DWI score showed excellent inter-reader agreement, indicating that this is a reliable imaging biomarker. Limitation of the current analysis included retrospective analysis. Relatively small sample size and lack of pre-treatment MRI. Information of ADC value might be worth investigation for patients with available ADC measurement.In conclusion, DWI score after NST of breast cancer was associated with DFS. Although the score is visual-based, high inter-reader agreement was demonstrated suggesting reliability of this value. DWI score derived from MRI after NST may be a promising and clinically feasible imaging biomarker in predicting prognosis of breast cancer patients who undergo NST.
Acknowledgements
No acknowledgment found.References
- Yau, C., et al., Residual cancer burden after neoadjuvant chemotherapy and long-term survival outcomes in breast cancer: a multicentre pooled analysis of 5161 patients. Lancet Oncol, 2022. 23(1): p. 149-160.
- Ota, R., et al., Evaluation of pathological complete response after neoadjuvant systemic treatment of invasive breast cancer using diffusion-weighted imaging compared with dynamic contrast-enhanced based kinetic analysis. Eur J Radiol, 2022. 154: p. 110372.
- Minarikova, L., et al., Investigating the prediction value of multiparametric magnetic resonance imaging at 3 T in response to neoadjuvant chemotherapy in breast cancer. Eur Radiol, 2017. 27(5): p. 1901-1911.
Figures
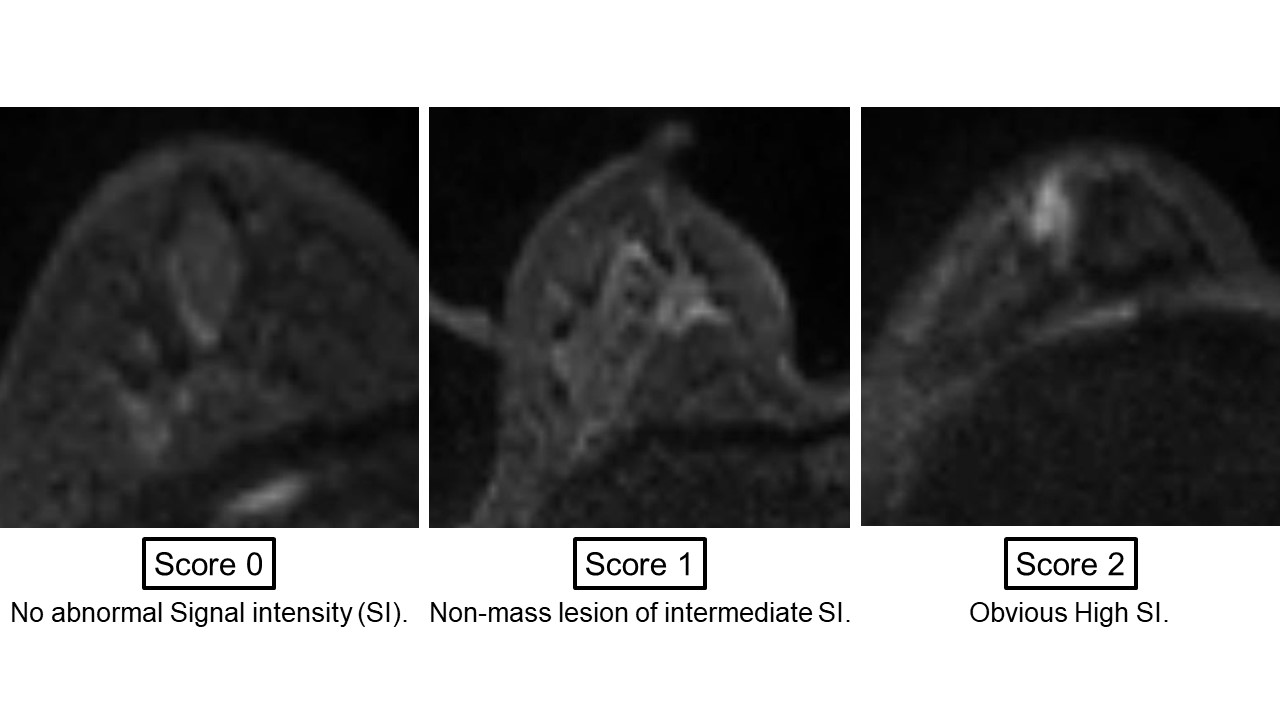
Figure 1. DWI score.
DWI score was scored based on visual assessment of high intensity area on DWI and defined as follows; 0 : no abnormal signal intensity, 1 : non-mass lesion of intermediate signal intensity, and 2 : obvious high signal intensity. Lower score indicates a higher likelihood of pCR and less cancer burden.
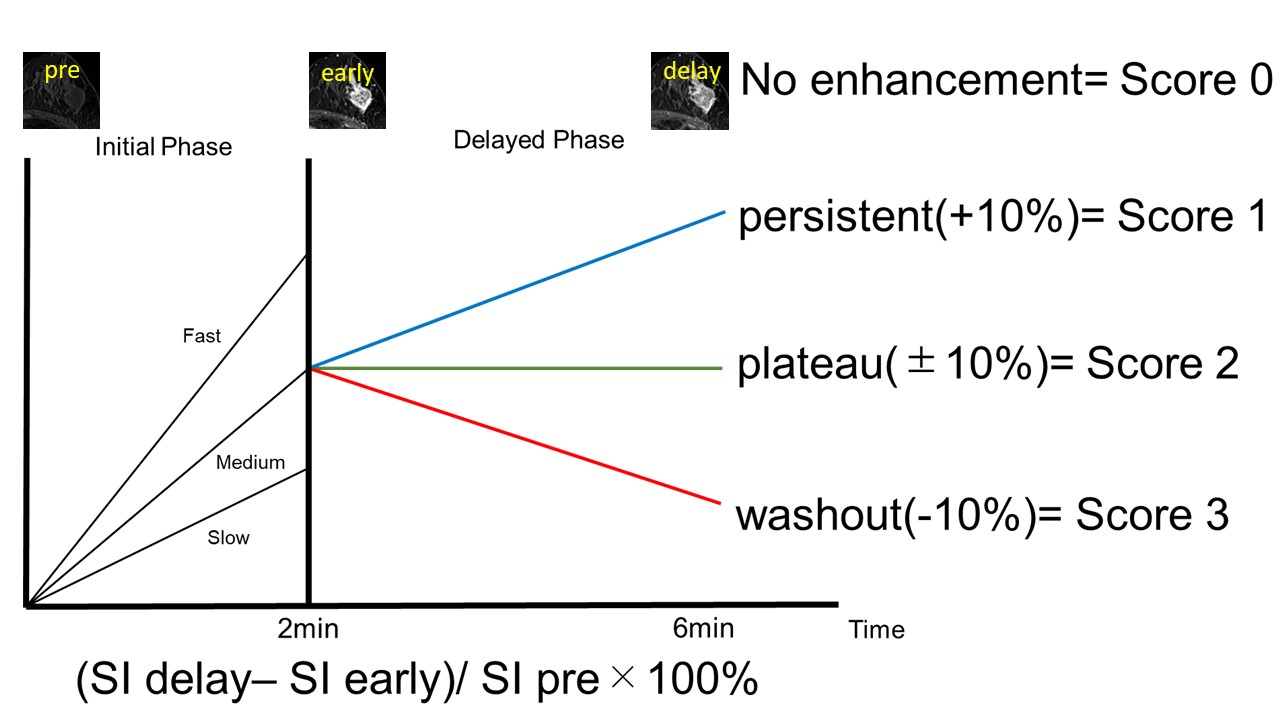
Figure 2. Kinetic score.
Based on the time-intensity curve after contrast agent injection, kinetic scores of the lesions on DCE-MRI was defined as follows; 0 : no enhancement, 1 : persistent, 2 : plateau and 3 : washout. Lower score indicates a higher likelihood of achieving pCR and less cancer burden.
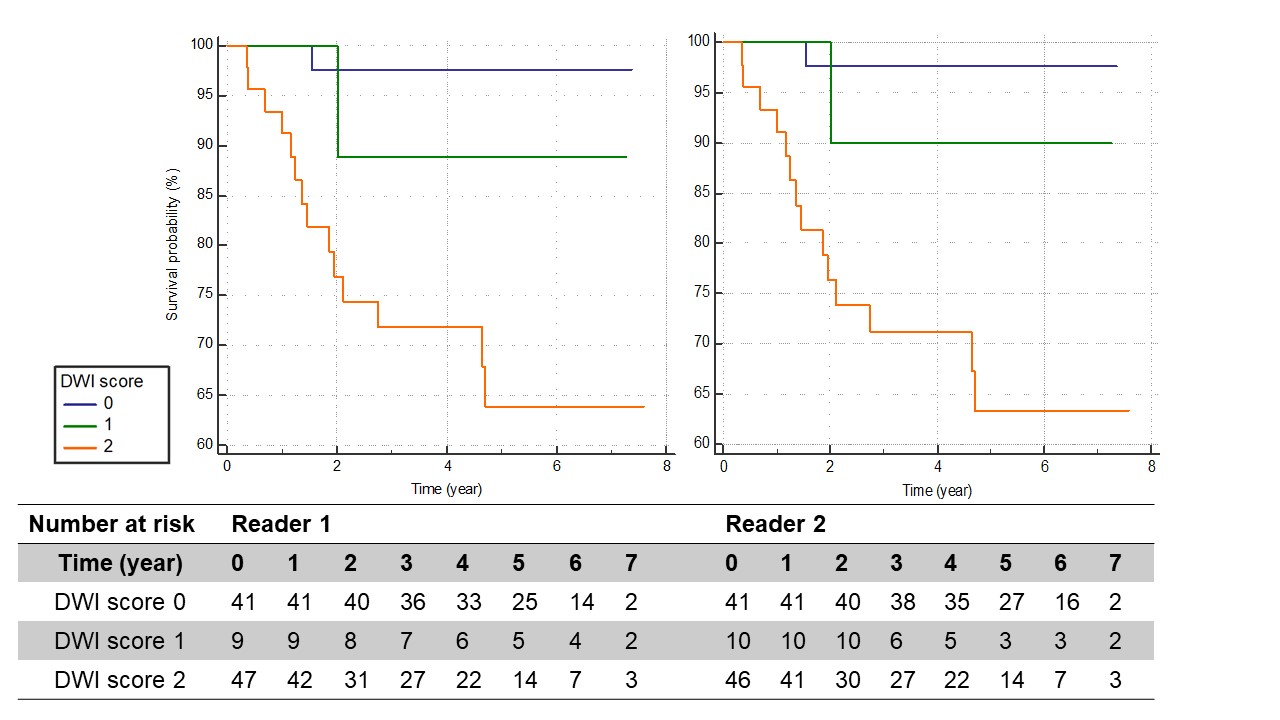
Figure 3. Kaplan-Meier survival curve of DFS for patients who underwent NST stratified by DWI score after NST (reader 1 and 2).
Patients with DWI score of 2 (orange) showed significantly shorter DFS compared to those with DWI score 0 (blue) or 1 (green), (Reader 1; Hazard radio (HR) 16.1: 95% Confidence interval (CI) 5.7-45.5, p<0.001/ Reader 2; HR 16.7: 95% CI 5.8-47.3, p<0.001).
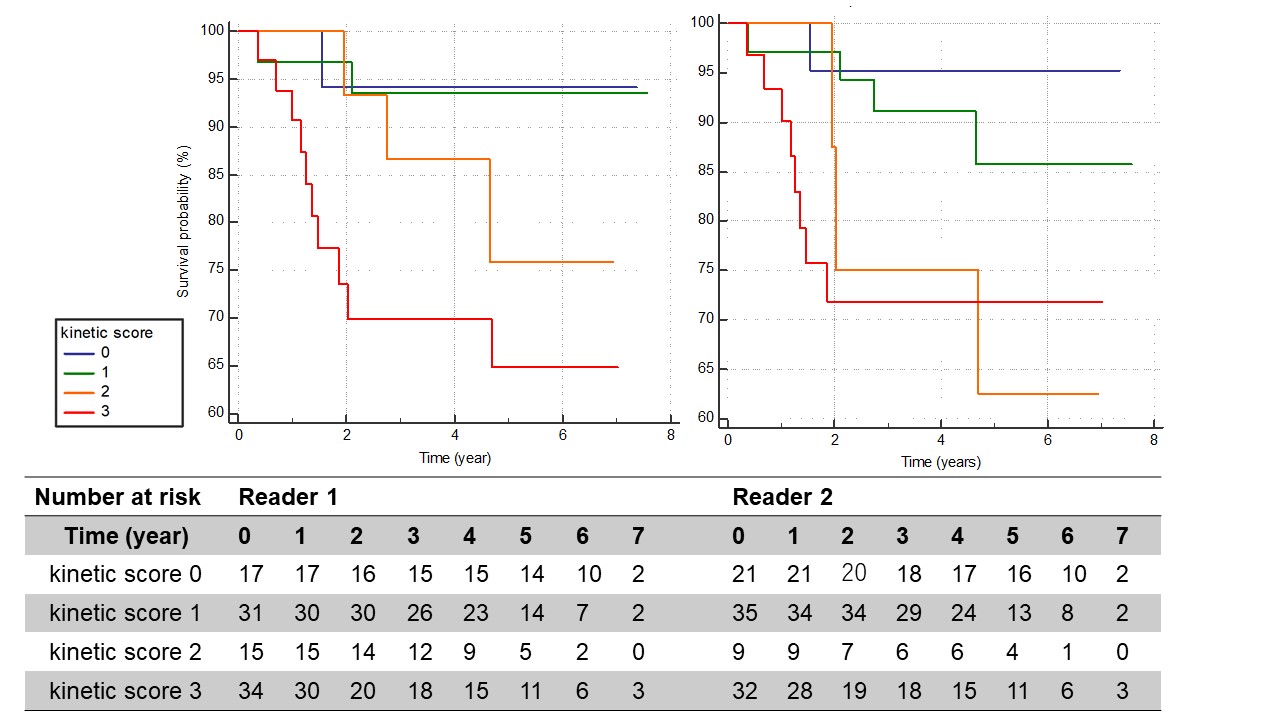
Figure 4. Kaplan-Meier survival curve of DFS for patients who underwent NST stratified by kinetic score after NST (reader 1 and 2).
Patients with kinetic score of 2 (orange) or 3 (red) showed significantly shorter DFS compared to those with kinetic score of 0 (blue) or 1 (green), (Reader 1; HR 7.07: 95% CI 1.7-29.4, p=0.017/ Reader 2; HR 7.5: 95% CI 1.2-47.8, p=0.059).
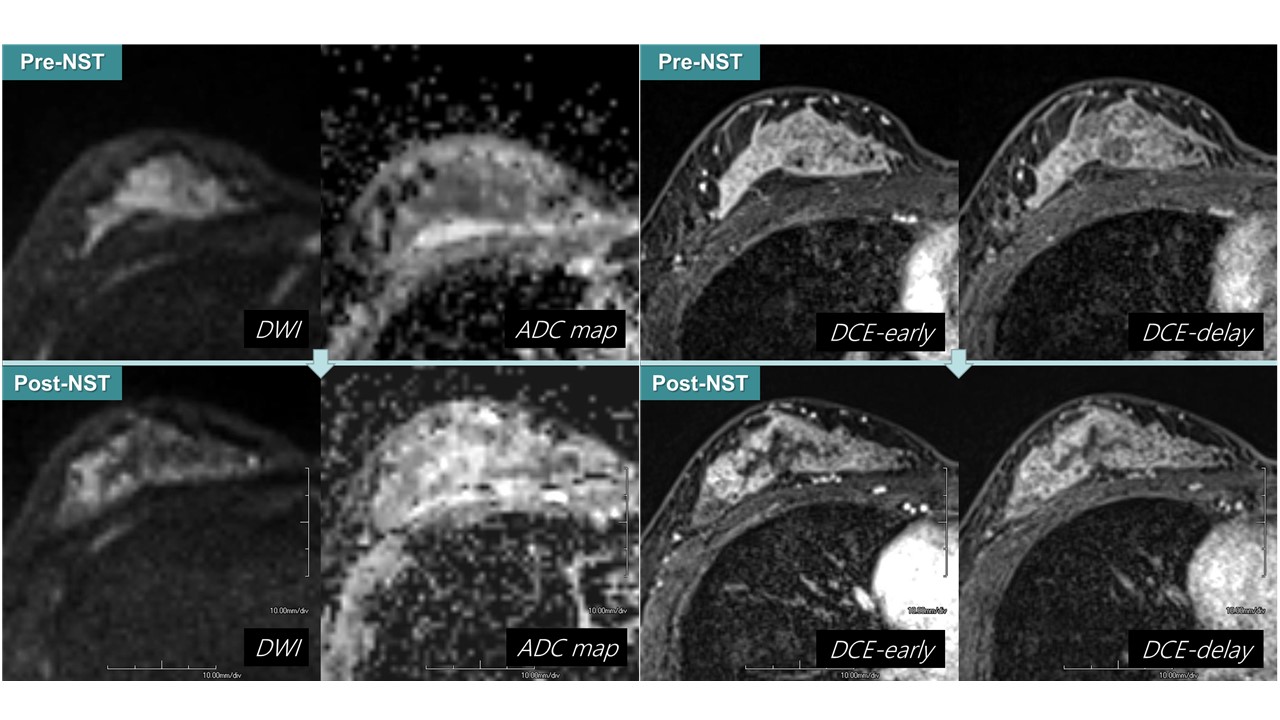
Figure 5. Representative case
A patient in her 40th with triple-negative breast cancer who underwent NST (Eribulin+Capecitabin x 6). Pre-treatment MRI(Pre-NST: upper row) showed a 9 cm non-mass lesion on DWI and DCE-MRI. Post-treatment MRI (Post-NST: lower row) showed lesions with high signal intensity on DWI, with enhancement of washout kinetic pattern on DCE-MRI. The DWI score was 2 and the kinetic score was 3. The patient underwent surgery and found the residual disease (non-pCR). After 8 months, She had a recurrence in the supraclavicular lymph nodes.