2697
Optimized model architecture and generalization for deep learning-based SAR prediction (MRSaiFE)
Mina Chookhachizadeh Moghadam1, Nawal Panjwani2, Elizaveta Motovilova1, Mengying Zhang 1, Fraser Robb3, Adrian Hoang1, Tasmia Afrin1, and Simone Angela Winkler1
1Radiology, Weill Cornell Medicine, New York, NY, United States, 2Tandon School of Engineering, New York University, New York, NY, United States, 3GE Healthcare, Aurora, OH, United States
1Radiology, Weill Cornell Medicine, New York, NY, United States, 2Tandon School of Engineering, New York University, New York, NY, United States, 3GE Healthcare, Aurora, OH, United States
Synopsis
Keywords: Safety, High-Field MRI, Deep Learning, SAR prediction, Tissue heating
Predicting the SAR distribution in ultra-high field MRI is a crucial task to prevent tissue damage due to the hotspots, though it is challenging. The MRSaiFE deep learning framework predicts SAR based on anatomical images, but it does not guarantee model generalization due to data leakage in the training process. To improve the model, we extended the UNet architecture to include residual and inception modules in its encoder part. Further, we implemented customized loss functions, and evaluation metrics to improve the predictive performance. The results show that the model predicts SAR with an SSIM=86% and MSE=0.14% for unseen body models.INTRODUCTION
Ultra-High Field (UHF) magnetic resonance imaging (MRI) promises increased signal-to-noise ratio (SNR)1, enabling improved imaging performance. Increasing the field strength, however, results in non-uniform deposition of radiofrequency power in the body, quantified using the specific absorption rate (SAR)2-3. This non-uniformity can result in hotspots and localized tissue heating referred to as ‘local SAR’4-11.To date, there is no in vivo real-time SAR monitoring capability – predicting local SAR and thus potential hotspots is therefore crucial to the success of the technology. This can be challenging due to its dependence on anatomical and positional differences between patients and hardware. Machine learning (ML) has been introduced to predict local SAR12-17. In our group, Gokyar et. al. proposed the deep learning (DL) framework MRSaiFE1 to predict SAR from simulated anatomical images. Here, we extend the MRSaiFE framework optimizing the model architecture, loss functions, and evaluation metrics (Fig.1). We also remove possible data leakage during training, allowing to predict SAR in new, “unseen” patients. We obtain a SSIM of approximately 86% and a mean square error (MSE) of 0.14% in unseen body models.
METHODS
Dataset. As previously reported17, the dataset includes 2D slices of five different body models from the Sim4Life18 virtual population19 (Duke, Ella, and pregnant women at gestational ages of 3, 5, and 7 months, respectively), using anatomical input images, weighted with an unloaded B1+ map for positional encoding, and simulated output SAR images.Network Architecture. The DL architecture in MRSaiFE17 is expanded by implementing UNet20 models with various encoder backbones (Fig.2). While the (1) simple UNet uses only convoluted neural network (CNN) modules for the encoder, the (2) Res-UNet21-23 uses residual blocks, thereby taking advantage of skip connections that allow to capture long-term dependencies existing in the input images. Further, we expand (2) to form the (3) InceptionRes-UNet architecture, in which we use kernels with varied dimensions of 1x1, 3x3, and 5x5 to extract features at varying scales from the input dataset24.
We further extend our 2D network to a (4)2.5D network, which allows for the use of multiple adjacent anatomical image slices as inputs. Specifically, we stack tuples of three adjacent MRI slices to predict the SAR distribution for the middle slice (Fig.3).
Training Process. To avoid data leakage, we train our network using four out of the five simulated body models and reserve the fifth for testing. MSE, SSIM25, soft DICE scores, and Focal Tversky26 loss functions are used. A customized loss function (Eq.1) is implemented to optimize the ‘weighted SSIM’, with as the percentage of background voxels in each 2D slice, and the hyperparameter α tunable to reduce significance of background voxels in training. The Adam optimizer27 is used to minimize the above loss functions using batch normalization28 and He initialization.
(1) Costomized loss function = 1 - α × ω × SSIM
Evaluation. The SSIM metric does not carry information about class imbalance, i.e. the ratio of non-background to background voxels for each slice, which could result in artificially high SSIM for slices with more background. We implement a new MRI-realistic metric “non-background SSIM” (SSIM-nb). This metric generates different masks for each 2D slice to include only the anatomical portion of the image in evaluation.
RESULTS
The optimization of the loss function determines L1 and L2 loss as the best option for SAR image mapping. Table1(a) shows the prediction results on unseen body models for the 4 proposed DL architectures. The results show that the (1) UNet architecture results in an SSIM of 83.5% and an SSIM_nb of 72% on average. Further, the (2) Res-UNet model shows an improved predictive performance with an SSIM of 86.0% and an SSIM_nb of 75%, while the (3) InceptionRes-UNet shows less improvement, with an SSIM of 85% and an SSIM_nb of 73%.Table2(b) shows the results for the (4) 2.5D network implemented based on the UNet and Res-UNet architectures. Comparing the UNet architectures in both 2D and 2.5D networks, the UNet 2.5D networks shows a slightly improved SSIM of 85%. The Res-UNet 2.5D, on the other hand, shows a maintained SSIM of around 86% and SSIM_nb of around 75%. Fig.4 shows the ground-truth and the predicted SAR for the body model Duke.
DISCUSSION
The moderate performance increases shown here are expected to significantly improve with a larger and more diverse training dataset in current/future work. Loss functions affect segmentation and image mapping problems differently. We thus hypothesize that the prediction of hotspots as opposed to full SAR images could benefit from loss functions other than L1/L2 – a subject of current and future work.CONCLUSION
In this work, we extend the MRSaiFE DL framework to mitigate data leakage in order to accurately predict the SAR distribution from anatomical MRI images of unseen body models. Our extended model predicts SAR with an SSIM=86% and MSE=0.14% for five unseen body models. The results show that we can potentially improve the predictive performance by using a combination of a more powerful encoding system, a better loss function, as well as by including adjacent slices via a 2.5D model. Future work will include training the optimized model using a large dataset of both simulated and experimental image and SAR data.Acknowledgements
The authors have nothing to declare.References
- Springer, E, Dymerska, B, Cardoso, PL, et al. Comparison of Routine Brain Imaging at 3 T and 7 T. Investigative Radiology 2016;51(8):469-482.
- Kraff O and Quick HH, “7T: Physics, safety, and potential clinical applications,” (in en), Journal of Magnetic Resonance Imaging, vol. 46, no. 6, pp. 1573–1589, 2017. [PubMed: 28370675]
- Collins CM and Smith MB, “Calculations of B1 distribution, SNR, and SAR for a surface coil adjacent to an anatomically-accurate human body model,” Magnetic Resonance in Medicine, vol. 45, no. 4, pp. 692–699, 2001. [PubMed: 11283998]
- Thornton MM, Picot PA, Rutt B, and Winkler S, “Method and System for Estimating the Specific Absorption Rate of a Tissue Region Prior to a Magnetic Resonance Imaging Scan,” US, 2015.
- Winkler SA, Picot PA, Thornton MM, and Rutt BK, “Direct SAR mapping by thermoacoustic imaging: A feasibility study,” Magnetic Resonance in Medicine, vol. 78, no. 4, pp. 1599–1606, 2017. [PubMed: 27779779]
- Hand JW, Lau RW, Lagendijk JJW, Ling J, Burl M, and Young IR, “Electromagnetic and thermal modeling of SAR and temperature fields in tissue due to an RF decoupling coil,” Magnetic Resonance in Medicine, vol. 42, no. 1, pp. 183–192, 1999. [PubMed: 10398965]
- Gandhi OP and Chen XB, “Specific absorption rates and induced current densities for an anatomy-based model of the human for exposure to time-varying magnetic fields of MRI,” Magnetic Resonance in Medicine, vol. 41, no. 4, pp. 816–823, 1999. [PubMed: 10332859]
- Simunic D, Wach P, Renhart W, and Stollberger R, “Spatial distribution of high-frequency electromagnetic energy in human head during MRI: numerical results and measurements,” IEEE Transactions on Biomedical Engineering, vol. 43, no. 1, p. 88, 1996. [PubMed: 8567009]
- Oh S, Ryu Y-C, Carluccio G, Sica CT, and Collins CM, “Measurement of SAR-induced temperature increase in a phantom and in vivo with comparison to numerical simulation,” Magnetic Resonance in Medicine, vol. 71, no. 5, pp. 1923–1931, 2014. [PubMed: 23804188]
- Katscher U, Voigt T, Findeklee C, Vernickel P, Nehrke K, and Dossel O, “Determination of Electric Conductivity and Local SAR Via B1 Mapping,” IEEE Transactions on Medical Imaging, vol. 28, no. 9, pp. 1365–1374, 2009. [PubMed: 19369153]
- Winkler SA and Rutt BK, “Practical methods for improving B1+ homogeneity in 3 tesla breast imaging,” Journal of Magnetic Resonance Imaging, vol. 41, no. 4, pp. 992–999, 2015. [PubMed: 24723508]
- Meliadò EF et al., “A deep learning method for image-based subject-specific local SAR assessment,” (in en), Magnetic Resonance in Medicine, vol. 83, no. 2, pp. 695–711, 2020 2020. [PubMed: 31483521]
- Meliadò EF, Van Den Berg CAT, Luijten PR, and Raaijmakers AJE, “Intersubject specific absorption rate variability analysis through construction of 23 realistic body models for prostate imaging at 7T,” Magnetic Resonance in Medicine, vol. 81, no. 3, pp. 2106–2119, 2019. [PubMed: 30414210]
- Mandija S, Meliadò EF, Huttinga NRF, Luijten PR, and Van Den Berg CAT, “Opening a new window on MR-based Electrical Properties Tomography with deep learning,” Scientific Reports, vol. 9, no. 1, 2019.
- Kabil JM, Geethanath S, and Vaughan JT, “Intra- and inter-brain RF heating prediction with the Non-Invasive Temperature Estimation (NITE) method,” 2020. Available: https://archive.ismrm.org/2020/4191.html
- Wyger M. Brink,Sahar Yousefi,Prernna Bhatnagar,Rob F. Remis,Marius Staring,Andrew G. Webb, “Personalized local SAR prediction for parallel transmit neuroimaging at 7T from a single T1-weighted dataset”, 2022, Available: https://doi.org/10.1002/mrm.29215
- Sayim Gokyar, Fraser J L Robb, Wolfgang Kainz, Akshay Chaudhari, Simone Angela Winkler “MRSaiFE: An AI-based Approach Towards the Real-Time Prediction of Specific Absorption Rate”, 2021, DOI: 10.1109/access.2021.3118290
- https://zmt.swiss/sim4life, Sim4Life, Zurich Med Tech, Zürich, Switzerland. Accessed July 10, 2022.
- https://itis.swiss/virtual-population, IT’IS Foundation, Zürich, Switzerland. Accessed July 11, 2022.
- Olaf Ronneberger, Philipp Fischer, Thomas Brox, “U-Net: Convolutional Networks for Biomedical Image Segmentation”, 2015, https://doi.org/10.48550/arXiv.1505.04597
- Foivos I. Diakogiannis, François Waldner, Peter Caccetta, Chen Wu, “ResUNet-a: a deep learning framework for semantic segmentation of remotely sensed data”, 2019, https://doi.org/10.48550/arXiv.1904.00592.
- Zhengxin Zhang, Qingjie Liu, Yunhong Wang, “Road Extraction by Deep Residual U-Net”, 2017, https://doi.org/10.48550/arXiv.1711.10684
- Kaiming He, Xiangyu Zhang, Shaoqing Ren, Jian Sun, “Deep Residual Learning for Image Recognition”, 2015, https://doi.org/10.48550/arXiv.1512.03385.
- Christian Szegedy, Vincent Vanhoucke, Sergey Ioffe, Jon Shlens, Zbigniew Wojna, “Rethinking the Inception Architecture for Computer Vision”, Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), 2016, pp. 2818-2826.
- Wang Z, Bovik AC, Sheikh HR, and Simoncelli EP, “Image Quality Assessment: From Error Visibility to Structural Similarity,” IEEE Transactions on Image Processing, vol. 13, no. 4, pp. 600–612, 2004. [PubMed: 15376593]
- Abdel Aziz Taha & Allan Hanbury, “Metrics for evaluating 3D medical image segmentation: analysis, selection, and tool”, BMC Medical Imaging, 2015.
- Kingma DP and Ba JL, “Adam: A Method for Stochastic Optimization,” arXiv pre-print server, 2017.
- Ioffe S and Szegedy C, “Batch Normalization: Accelerating Deep Network Training by Reducing Internal Covariate Shift,” arXiv pre-print server, 2015.
Figures
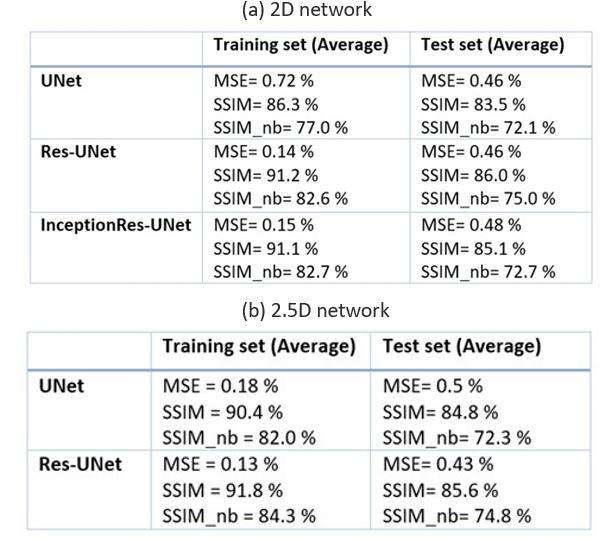
Table 1: (a) The performance of different DL models in SAR prediction on 5 different body
models. Res-UNet architectures result in better predictive performance with an
SSIM= 86% and SSIM_nb=75% on average. (b) The predictive performance of the 2.5D network utilizing either CNN or ResNet backbones. Compared to its 2D network, the 2.5D UNet shows a 2% improvement in the SSIM, while the 2.5D Res-UNet shows similar results.
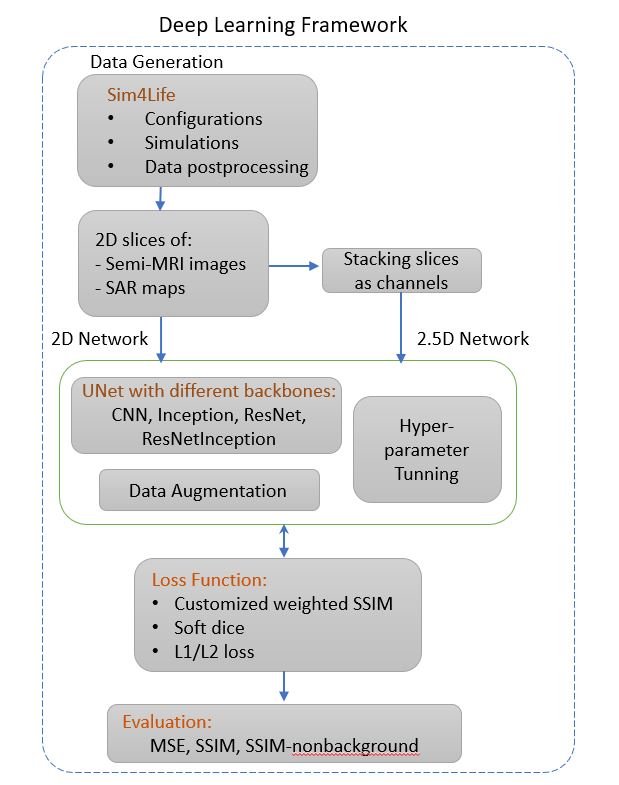
Figure 1: The overall flow of the extended MRSaiFE deep
learning framework to improve the model generalization to predict SAR
distribution from anatomical images for unseen patients.
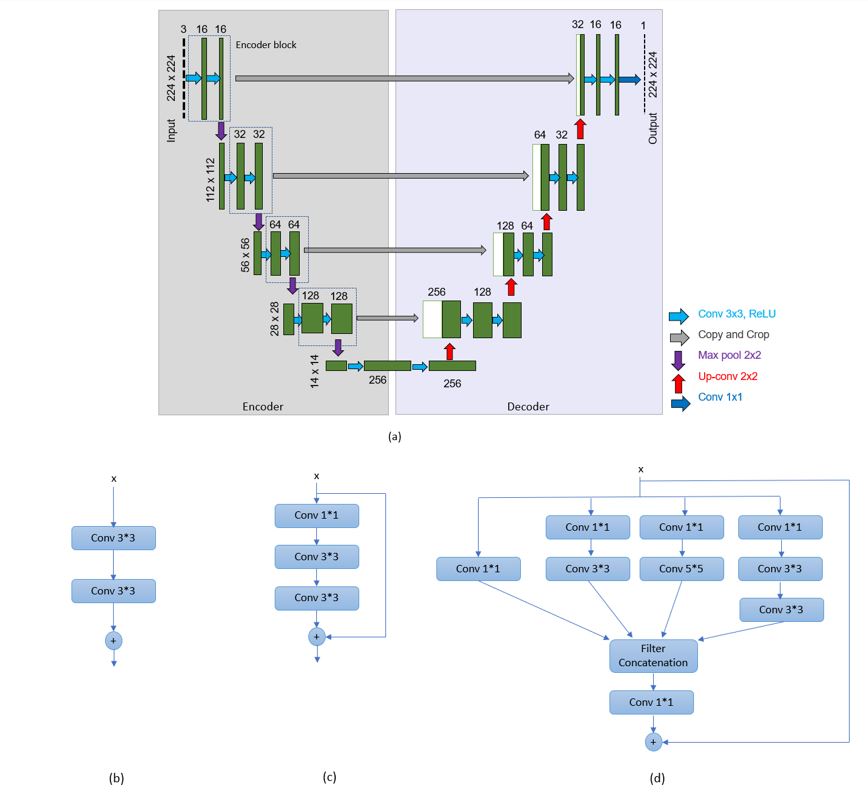
Figure
2: The extended deep learning
architecture used to predict SAR based on simulated anatomical images. The
overall architecture is a UNet (a) with three different blocks as its
backbones, i.e. CNNs, ResNets, and InceptionResNets. In its simplest form, the
basic encoding building blocks used in the UNet, Res-UNet, and
InceptionRes-UNet are shown in (b), (c) and (d) respectively.
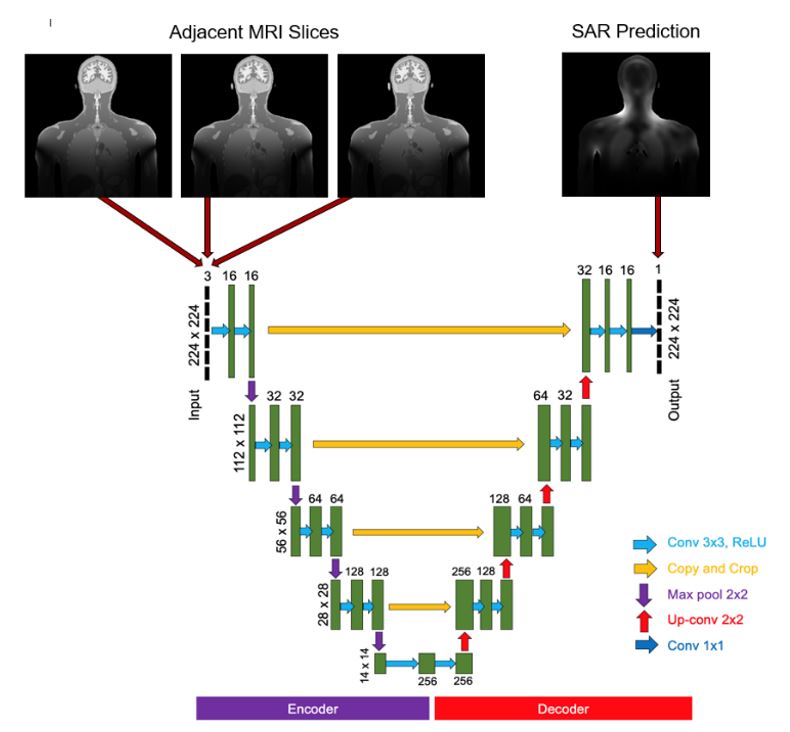
Figure 3: The 2.5D UNet architecture used to predict
the SAR distribution. The input takes three adjacent anatomical slices to
predict the SAR distribution for the middle slice.
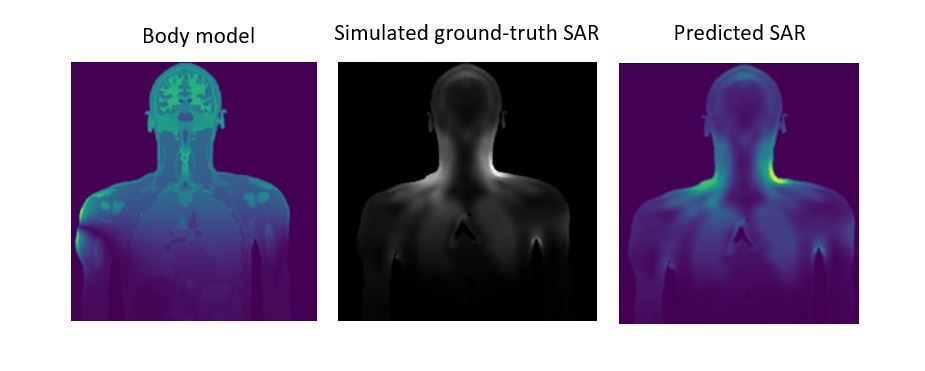
Figure 4: One MRI slice of the body model Duke, the simulated ground-truth SAR and the predicted SAR distribution.
DOI: https://doi.org/10.58530/2023/2697