2611
Effects of HIV-associated chronic inflammation on intracranial vessels using semi-automatic segmentation of MRA cerebrovascular features1Physics, University of Rochester, Rochester, NY, United States, 2Radiology, University of Rochester, Rochester, NY, United States, 3Neurology, University of Rochester, Rochester, NY, United States, 4Neurology-Stroke Division, University of Rochester, Rochester, NY, United States, 5Department of Electrical and Computer Engineering, University of Rochester, Rochester, NY, United States, 6Cardiology Research, University of Rochester, Rochester, NY, United States, 7Department of Electrical and Computer Engineering, University of Washington, Seattle, WA, United States, 8Biostatistics, University of Rochester, Rochester, NY, United States
Synopsis
Keywords: Neuroinflammation, Vessels, MRA, CSVD, HIV
HIV infected individuals (HIV+) are subjected to high risks of neurological complications, including cerebrovascular disease. Quantification of vascular features may provide a tool to investigate pathomechanisms and monitor cerebrovascular disease progression. In this study we used intracranial artery feature extraction (iCafe) to compare HIV+ with age matched controls.Introduction
Although human immunodeficiency virus (HIV) mainly affects the immune system, the virus can cross the blood-brain barrier and infect cells of the nervous system such as microglia, perivascular macrophages and in a restricted manner astrocytes and oligodendrocytes1,2. HIV-associated chronic inflammation persist despite the use of antiretroviral drugs, contributing to both large and small vessel disease3,. Despite the relevance of advancing cerebrovascular disease in HIV+, quantitative morphometry and intensity features of intracranial vessels are missing. In this study, we used iCafe to extract and quantify vascular features of magnetic resonance angiography (MRA) images4. In recent years, iCafe has been used in multiple cerebrovascular studies with good reproducibility. Icafe features such as branch number, vessel length, and tortuosity have been employed as reliable metrics to quantify the effects of hypertension and aging, and on the intracranial vessels5,6,7.Methods
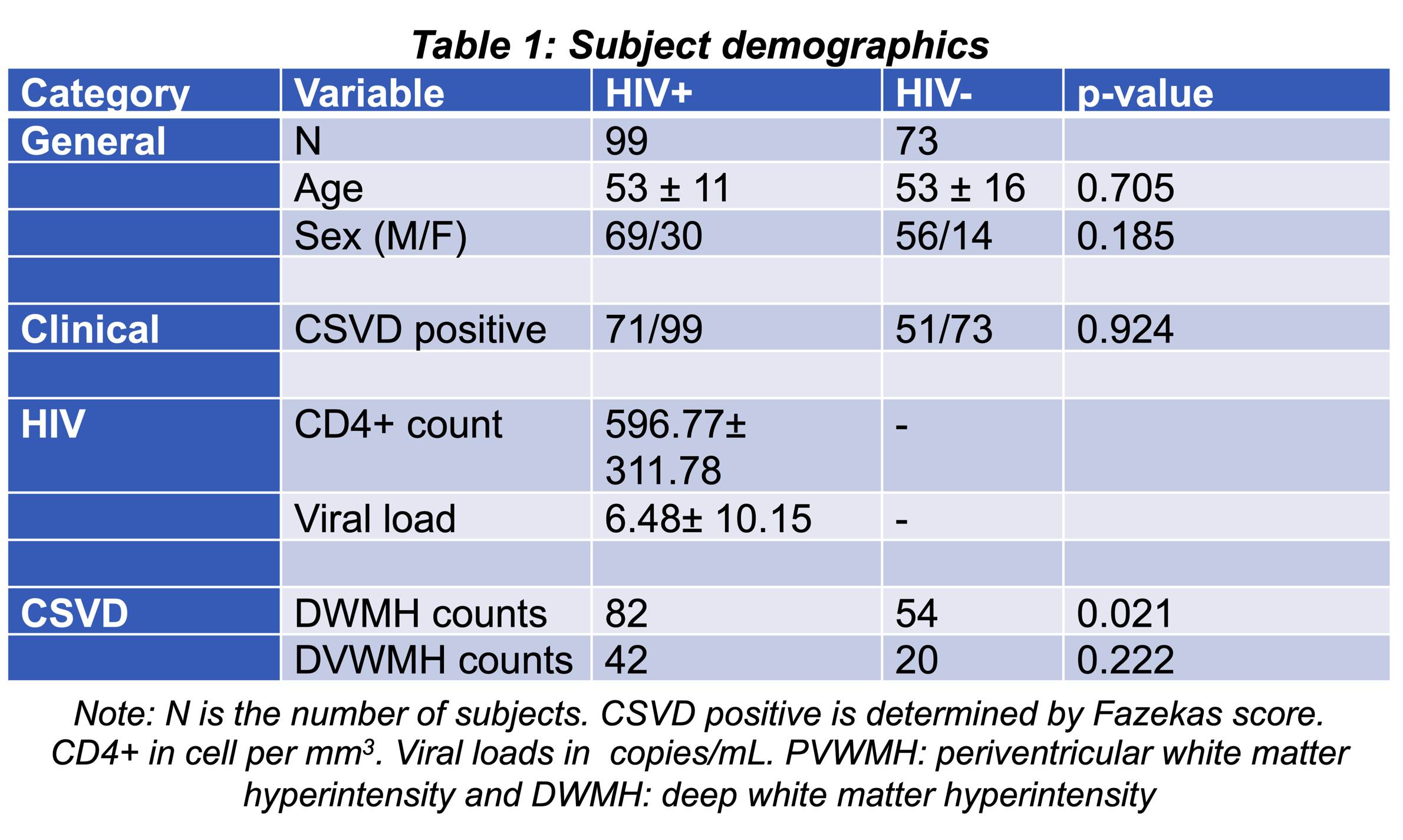
Participants: After obtaining written informed consents, 73 HIV- subjects (age = 53±16 years, female = 14) and 99 HIV+ subjects (age = 53 ± 11 years, female = 30) were selected from the University of Rochester ongoing CSVD protocols approved by the Research Subject Review Board. HIV+ CD4 counts were 596.769± 311.781 counts/mm3 and viral loads were 6.481± 10.145 copies/mL. An overview of the demographics is provided in Table 1.MR Imaging: A 3D TOF-MRA was performed on a 3T Siemens MAGNETOM PrismaFit whole-body scanner equipped with a 64-channel phased array, with the scan parameters: repetition time (TR)= 21 ms, echo time (TE)= 3.42 ms, flip angle= 20°, image resolution =0.52×0.52×0.52 mm3, acquisition time = 8:42 min.
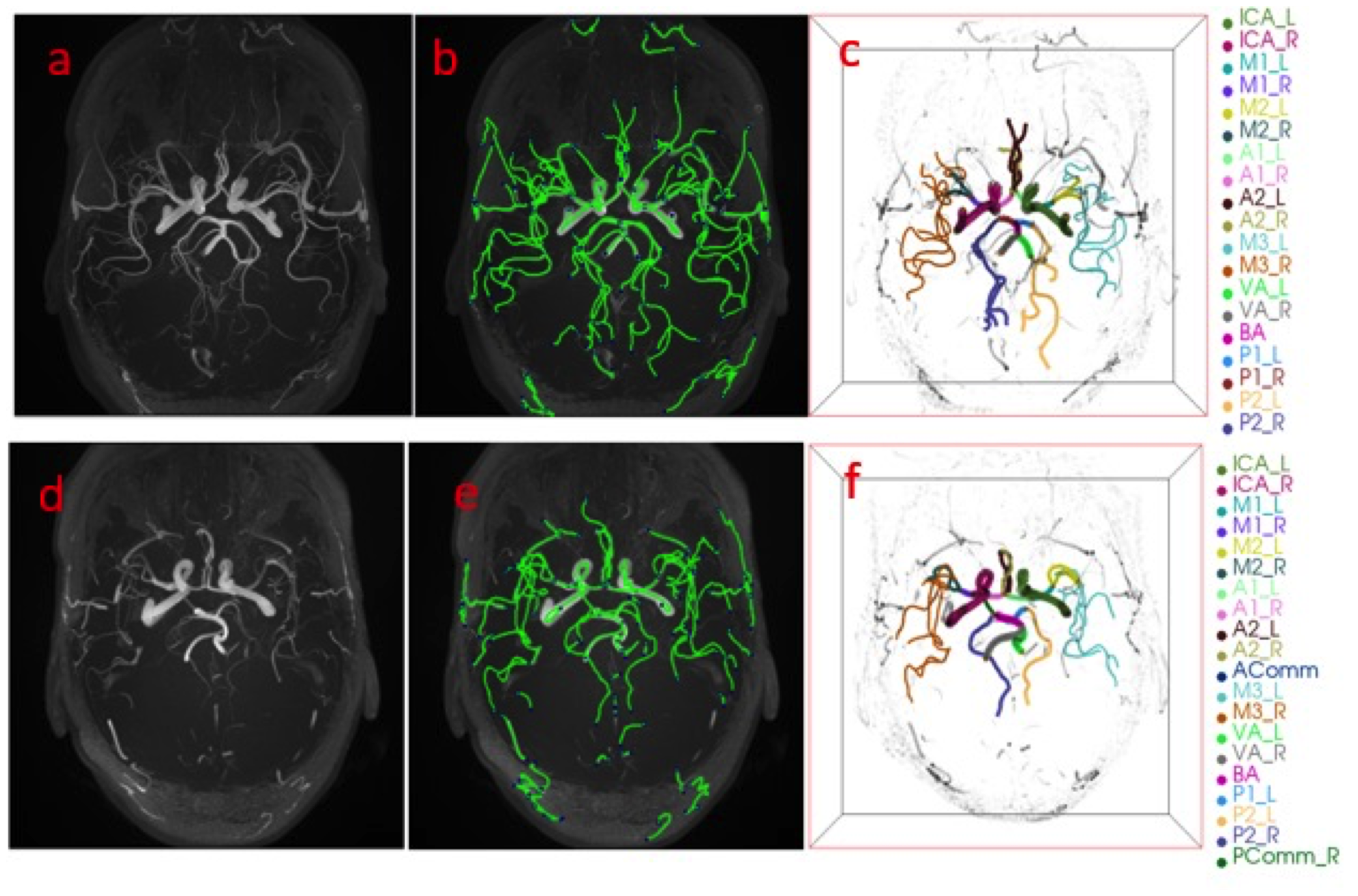
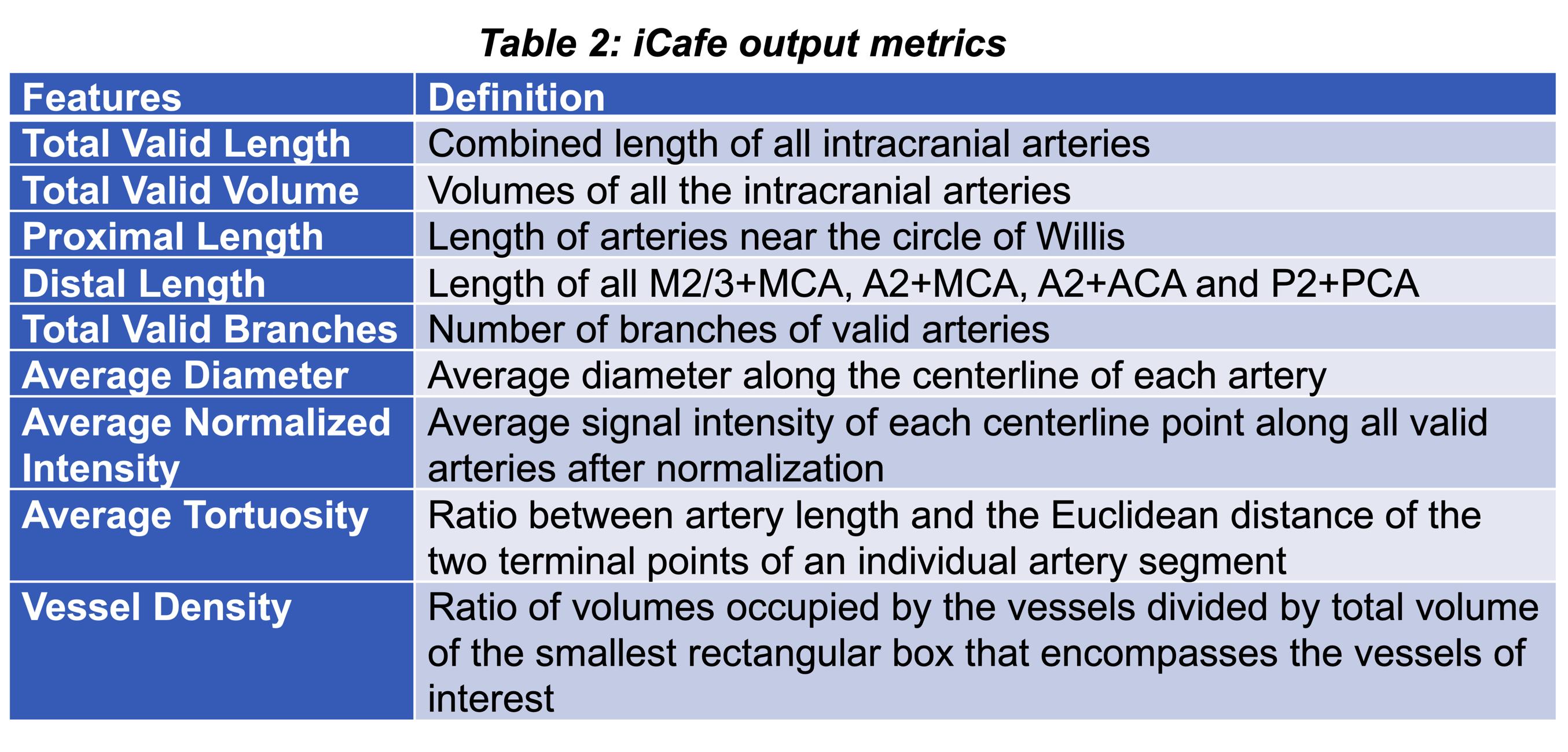
iCafe feature extraction: All subjects are analyzed using iCafe which employs an active contour model to trace vessels in MRA images and reconstructs them as skeleton vascular tubes using a maximum-a-posteriori estimation4. The reconstructed vessels are then labeled based on 22 arterial regions in the circle of Willis (CoW). The tracing and reconstruction of vessels in iCafe is semi-automatic and needs human correction to remove faulty reconstructed or mislabeled vessels. An example of the final output of iCafe tracing after correction is shown in Figure 1, and major iCafe output metrics are provided in Table 2.
Statistical analysis: Vascular morphometry difference between iCafe outputs of HIV+ and HIV- were assessed by unpaired t-test and a W-test. For statistical considerations, features with a two-tailed p-value below 0.05 are considered significant. Additionally, both age and gender’s influence on vessel morphometry were considered and adjusted for in all statistical calculations.
Results
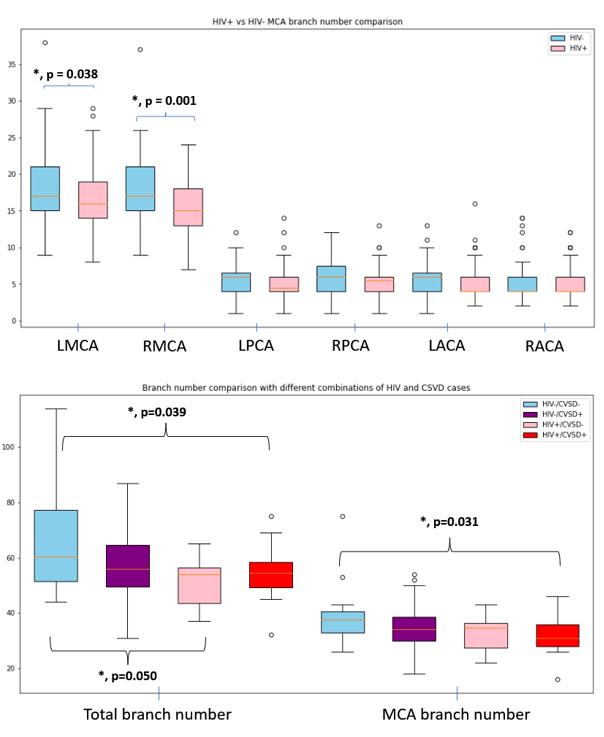
iCafe Metrics and HIV status: A box and whisker plot of the iCafe branch metrics of the MCA, PCA and ACA is shown in figure 2. We found significant differences comparing the branch number, diameter, and vessel length between the two cohorts, particularly in the MCA and PCA regions, where branch numbers and length metrics were lower for HIV+ compared to HIV- (p value = 0.003). ICAs diameter were significantly lower for HIV+ (p value = 0.013).iCafe Metrics and sex differences: Analysis showed significant differences between male and female vascular diameters between the ICA and the M3 segments of the MCA. Females have wider M3 (p value <.001), while having narrower ICA diameters (p value = 0.037).
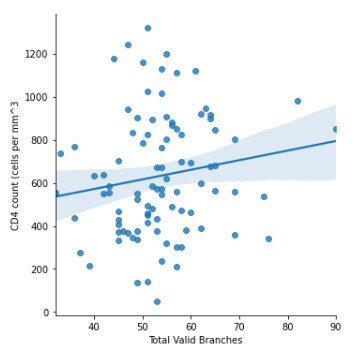
iCafe Metrics and CD4 count for HIV+ population: Using Pearson test, we found that the branch number, particularly in the MCA region, is positively correlated with CD4 counts for the HIV+/CSVD- case but not for HIV+/CSVD+ cases. Analysis showed no significant correlations between CD4 and vessel length in both cases. The correlation plot between total valid branch number and CD4 count for HIV+ is provided in figure 3.
iCafe Metrics and CSVD status: We studied the relationship between Icafe parameters and HIV/CSVD combinations. Our result, summarized in Figure 2, showed that the total and MCA branches number are significantly different between CSVD-/HIV- and CSVD+/HIV+ cases (p-value = 0.039). Lower branch numbers seem to correlate with both HIV and CSVD status, with HIV being the more influential factor.
Discussion
Our analysis shows that HIV-status is associated with differences in vascular morphometry. The main differences lie in the MCA regions, where the branch number and length were decreased compared to controls. The other significant findings were the diameter differences between HIV+ and controls, particularly in PCA and ICA. Of interest, this effect, seems to be mediated by sex differences with HIV+ having more than twice the number females than controls population (30 vs.14). Since HIV+ with and without CSVD have similar number of branches and length, but less than HIV- without CSVD, it suggests that HIV-associated chronic inflammation may play role independently of vascular risk factors. The trend in positive correlation between CD4 count and the number of branches would in part support this possibility.Conclusion
Our data suggest that HIV+ are more exposed than controls to cerebrovascular disease. iCafe metrics can be used to further investigate pathomechanisms such as contribution of vascular risk factors and as well as inflammatory biomarkers. Our ongoing analyses will further characterize the contribution of these additional factors.Acknowledgements
This work was supported by The National Institutes of Health (NIH; R01 MH099921, R01 AG054328, and R01 MH118020).References
1. Pasternak, O., Westin, C.-F., Dahlben, B., Bouix, S., & Kubicki, M. (2015). The Extent of Diffusion MRI Markers of Neuroinflammation and White Matter Deterioration in Chronic Schizophrenia. Schizophrenia Research, 161(1), 113–118. https://doi.org/10.1016/j.schres.2014.07.031
2. Pinto, A. N. (1996). AIDS and Cerebrovascular Disease. Stroke, 27(3), 538–543. https://doi.org/10.1161/01.STR.27.3.538
3. Murray, K. D., Singh, M. V., Zhuang, Y., Uddin, M. N., Qiu, X., Weber, M. T., Tivarus, M. E., Wang, H. Z., Sahin, B., Zhong, J., Maggirwar, S. B., & Schifitto, G. (2020). Pathomechanisms of HIV-Associated Cerebral Small Vessel Disease: A Comprehensive Clinical and Neuroimaging Protocol and Analysis Pipeline. Frontiers in Neurology, 11, 595463. https://doi.org/10.3389/fneur.2020.595463
4. Chen, L., Mossa-Basha, M., Balu, N., Canton, G., Sun, J., Pimentel, K., Hatsukami, T. S., Hwang, J.-N., & Yuan, C. (2018). Development of a Quantitative Intracranial Vascular Features Extraction Tool on 3D MRA Using Semi-automated Open-Curve Active Contour Vessel Tracing. Magnetic Resonance in Medicine, 79(6), 3229–3238. https://doi.org/10.1002/mrm.26961
5. Chen, L., Shaw, D. W. W., Dager, S. R., Corrigan, N. M., Chu, B., Kleinhans, N. M., Kuhl, P. K., Hwang, J.-N., & Yuan, C. (2021). Quantitative Assessment of the Intracranial Vasculature of Infants and Adults Using iCafe (Intracranial Artery Feature Extraction). Frontiers in Neurology, 12, 668298. https://doi.org/10.3389/fneur.2021.668298
6. Liu, W., Chen, Z., Ortega, D., Liu, X., Huang, X., Wang, L., Chen, L., Sun, J., Hatsukami, T. S., Yuan, C., Li, H., & Yang, J. (2021). Arterial elasticity, endothelial function and intracranial vascular health: A multimodal MRI study. Journal of Cerebral Blood Flow and Metabolism: Official Journal of the International Society of Cerebral Blood Flow and Metabolism, 41(6), 1390–1397. https://doi.org/10.1177/0271678X20956950
7. Liu, W., Huang, X., Liu, X., Ortega, D., Chen, L., Chen, Z., Sun, J., Wang, L., Hatsukami, T. S., Yuan, C., Li, H., & Yang, J. (2021). Uncontrolled hypertension associates with subclinical cerebrovascular health globally: A multimodal imaging study. European Radiology, 31(4), 2233–2241. https://doi.org/10.1007/s00330-020-07218-5
Figures