2583
The value of ASL combined with DTI for detection of impaired renal allograft function1Department of Radiology, The First Affiliated Hospital of Soochow University, Suzhou, China, 2Department of Urology, The First Affiliated Hospital of Soochow University, Suzhou, China, 3Philips Healthcare, Shanghai, China
Synopsis
Keywords: Arterial spin labelling, Kidney
Allograft injury continues to be a major problem in renal allograft recipients, which leads to eventual graft loss. Non-invasive and reliable detection of impaired renal allograft function is crucial to preventing irreversible nephron loss and graft failure. This study aims to investigate the value of ASL combined with DTI for the detection of impaired renal allograft function. Results showed that a higher diagnostic efficacy could be achieved through the combined use of ASL and DTI.Introduction
Kidney transplantation is the therapy of choice for patients with end-stage renal disease, which provides improved long-term outcomes and better quality of life when compared to dialysis. Nevertheless, despite the improvement of surgical techniques and immunosuppressive therapy, allograft injury after transplantation is relatively common and may lead to graft loss in the long term1. Allograft biopsy is still the gold standard for the diagnosis of allograft injury. However, biopsy is an invasive method which may increase the risk of complications including bleeding, infection, and even graft loss. Magnetic resonance imaging (MRI) has the potential to provide not only morphological but also functional information of renal allografts. Arterial spin labeling (ASL) MRI uses blood as an endogenous contrast agent, allowing perfusion measurements without the administration of exogenous contrast2. Diffusion tensor imaging (DTI) provides information about not only diffusion but also the anisotropy of diffusion, which is quantified by the fractional anisotropy (FA)3, 4. The purpose of this study was to investigate the clinical value of ASL and DTI in the detection of impaired renal allograft function.Methods
Eighty-four patients with renal transplantation in our hospital were recruited in the study. Patients were assigned into two groups according to estimated glomerular filtration rate(eGFR): forty-two patients with good renal function (eGFR≥60 mL/min/1.73 m2, 21 male, mean age, 40 years; range, 23-67 years) and forty-two patients with impaired renal function (eGFR<60 mL/min/1.73 m2, 30 male, mean age, 46 years; range, 21-63 years). All patients performed MR examinations on a 1.5 T MR scanner (Ingenia Ambition, Philips Healthcare, Best, the Netherlands). The MR protocol includes ASL, DTI, T1 weighted (T1WI) and T2 weighted (T2WI) imaging sequences. Axial turbo spin-echo T1-weighted images and coronal fat-saturated turbo spin-echo T2-weighted images were acquired for anatomical evaluation of the transplanted kidney. For ASL, images were acquired using a pulsed-continuous arterial spin labeling (pCASL) and 3-dimensional GRAdient and Spin Echo (GRASE) scheme. The imaging parameters were as follows: TR = 3963 ms; TE = 15 ms; voxel size = 3.75 × 3.75 × 8 mm3; FOV = 240 × 240 × 88 mm3; TSE factor = 20; EPI factor = 15; eight dynamics. For DTI, the imaging parameters were as follows: diffusion directions=15; b values = 0 and 600 s/mm2; TR = 2300 ms; TE = 67 ms; 20 slices with slice thickness/gap = 5.0/1.0 mm; voxel size=2.5×2.5×5 mm3; FOV=320 × 400 mm2. Apparent diffusion coefficient (ADC), fractional anisotropy (FA) from DTI, and renal blood flow (RBF) from ASL were calculated in the workstation (Intellispace Portal; v10; Philips Healthcare). For DTI, several regions of interest (ROIs) were placed in the renal cortex and medulla regions. For ASL, several ROIs were placed in the renal cortex region. Kolmogorov-Smirnov test was used to test whether the data conformed to normal distribution. Independent-sample t-test was used to compare the differences of mean eGFR, RBF, ADC values, and FA values between the two groups. Correlation analysis (Pearson) between all parameters and the eGFR value of patients were conducted in SPSS 25.0 software. The receiver operating characteristic (ROC) curve and binary logistic regression analyses were performed to assess the diagnostic efficiency of RBF, ADC, FA in distinguishing allografts with impaired function from those with normal function.Results
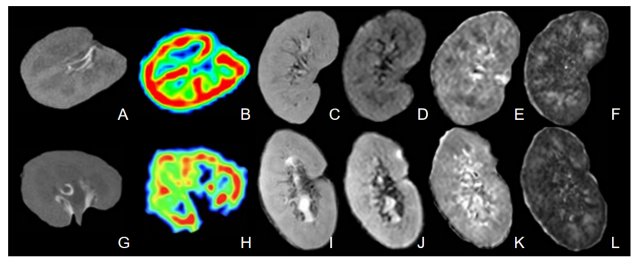
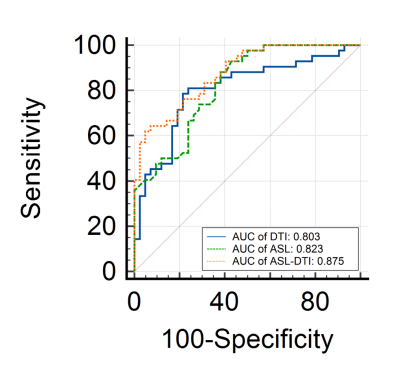
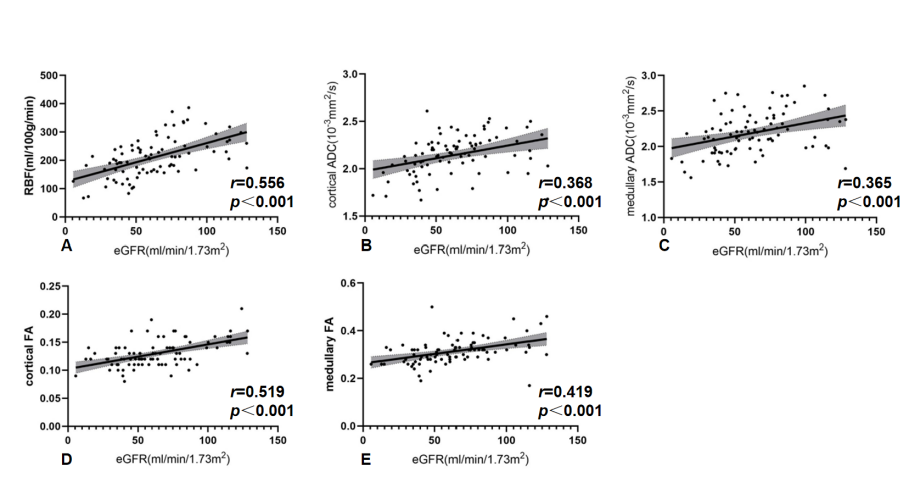
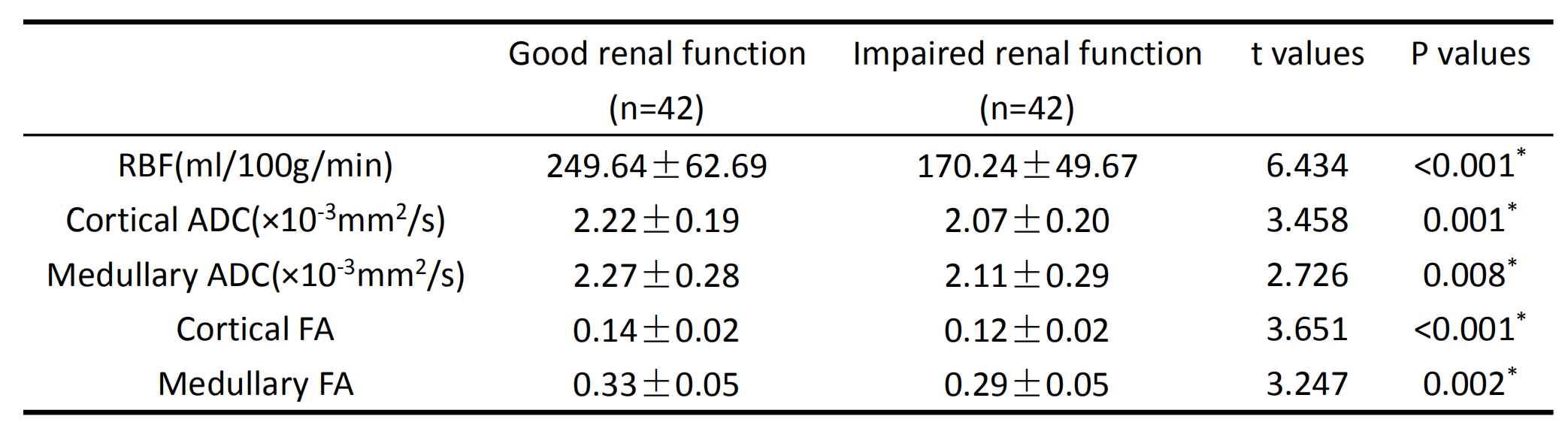
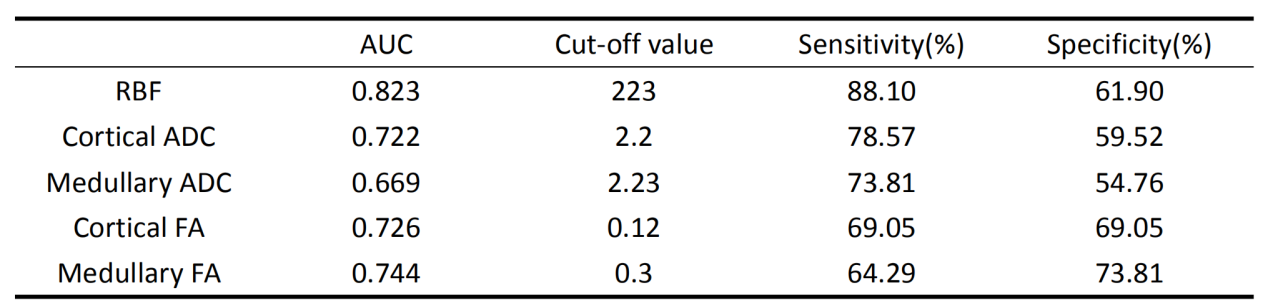
Representative images for a 26-year-old man with good allograft function and a 48-year-old man with impaired allograft function are shown in Figure 1. The RBF, ADC, FA values from patients with good renal function were higher than those from patients with impaired renal function, the difference was statistically significant (p < 0.05) (Table 1). As shown in Figure 3, there was a positive correlation between eGFR and RBF, cortical ADC, medullary ADC, cortical FA and medullary FA. RBF value had the highest AUC (AUC=0.823) to discriminate between the two groups (Table 2). The combined use of ASL and DTI showed significantly improved differential diagnosis efficacy between patients with good and impaired renal function (Figure 2).Discussion
Many complications including allograft rejection, acute tubular necrosis (ATN), immunological reactions and recurrence of primary nephropathy could contribute to the impairment of allograft function5. Impaired allograft function tends to be accompanied by decreased blood perfusion and disorder of microstructure. In this study, reduced renal blood flow measured by ASL was observed in patients with impaired renal function. Furthermore, renal blood flow positively correlated with eGFR, thus reaching the conclusion that renal perfusion measured by ASL reflected allograft function. FA was significantly reduced in patients with impaired renal function, thus suggesting alterations of renal microstructure. In addition, reduced tubular flow and microvascular perfusion in allografts with impaired function may also lead to lower FA values.Conclusion
The combined use of ASL and DTI can improve the sensitivity and accuracy of diagnosis for detection of impaired renal allograft function.Acknowledgements
No acknowledgement found.References
1. van Eijs MJM, van Zuilen AD, de Boer A, Froeling M, Nguyen TQ, Joles JA, Leiner T, Verhaar MC. Innovative Perspective: Gadolinium-Free Magnetic Resonance Imaging in Long-Term Follow-Up after Kidney Transplantation. Front Physiol. 2017 May 16;8:296. doi: 10.3389/fphys.2017.00296. PMID: 28559850; PMCID: PMC5432553.
2. Yu YM, Wang W, Wen J, Zhang Y, Lu GM, Zhang LJ. Detection of renal allograft fibrosis with MRI: arterial spin labeling outperforms reduced field-of-view IVIM. Eur Radiol. 2021 Sep;31(9):6696-6707. doi: 10.1007/s00330-021-07818-9. Epub 2021 Mar 18. PMID: 33738596.
3. Hueper K, Khalifa AA, Bräsen JH, Vo Chieu VD, Gutberlet M, Wintterle S, Lehner F, Richter N, Peperhove M, Tewes S, Weber K, Haller H, Wacker F, Gwinner W, Gueler F, Hartung D. Diffusion-Weighted imaging and diffusion tensor imaging detect delayed graft function and correlate with allograft fibrosis in patients early after kidney transplantation. J Magn Reson Imaging. 2016 Jul;44(1):112-21. doi: 10.1002/jmri.25158. Epub 2016 Jan 18. PMID: 26778459.
4. Adams LC, Bressem KK, Scheibl S, Nunninger M, Gentsch A, Fahlenkamp UL, Eckardt KU, Hamm B, Makowski MR. Multiparametric Assessment of Changes in Renal Tissue after Kidney Transplantation with Quantitative MR Relaxometry and Diffusion-Tensor Imaging at 3 T. J Clin Med. 2020 May 21;9(5):1551. doi: 10.3390/jcm9051551. PMID: 32455558; PMCID: PMC7290480.
5. Fan WJ, Ren T, Li Q, Zuo PL, Long MM, Mo CB, Chen LH, Huang LX, Shen W. Assessment of renal allograft function early after transplantation with isotropic resolution diffusion tensor imaging. Eur Radiol. 2016 Feb;26(2):567-75. doi: 10.1007/s00330-015-3841-x. Epub 2015 May 28. PMID: 26017738.
Figures