2566
Synthetic high-b-value reduced field-of-view DWIs in breast cancer elevates lesion clarity and CNR1Department of Radiology,Taihe hospital, Hubei, China, 2GE Healthcare, MR Research, Beijing, China
Synopsis
Keywords: Breast, Diffusion/other diffusion imaging techniques
Our study showed synthetic DW images (syDWIs) with high b-value provided better lesion conspicuity, image quality and contrast to noise (CNR), reduce scan time of DWI acquisitions especially at very high b-value, and improved lesion visualization particularly in dense breast. Moreover, derived ADC values showed good consistency between scanned and synthetic DWIs. Therefore, syDWIs with b value of 800 s/mm2 have great potential in elevation of diagnosis confidence and efficacy on tumors and high repeatability of ADC values is helpful in replacement of scanned high-b-value DWIs in clinics despite existed intra-modality, but not inter-modality, difference of manual ROI measures.Introduction
Clinically-used diffusion-weighted imaging with b-value 800 s/mm2 is used to grade tumors without the use of contrast agents [1] and showed the same sensitivity to breast lesions as contrast-enhanced MRI. Tissues with high limited diffusion, such as most malignant breast tumors, appear relatively visible and bright on high b-value DWIs. However, a higher b-value leads to an increase in imaging artifacts and noise as well as a decrease in signal-to-noise ratio (SNR) and a prolonged scan time [2]. Image quality directly affects the reliability and repeatability of ADC values due to edge delineation of ROIs[3,4]. Synthetic DW images (syDWIs) with high b-value provide better lesion conspicuity, image quality and tumor-to-tissue contrast (SIR), reduce scan time of DWI acquisitions especially at very high b-value, and improve lesion visualization particularly in dense breast [2,5,6]. Better fat suppression and less artifact can be achieved on 1.5T compared to 3T, and thus our study was to explore the feasibility of syDWIs on 1.5T, including the diagnostic quality, discrimination efficiency of tumors on syDWIs and repeatability of ADC values for setting up a breast cancer protocol.Methods
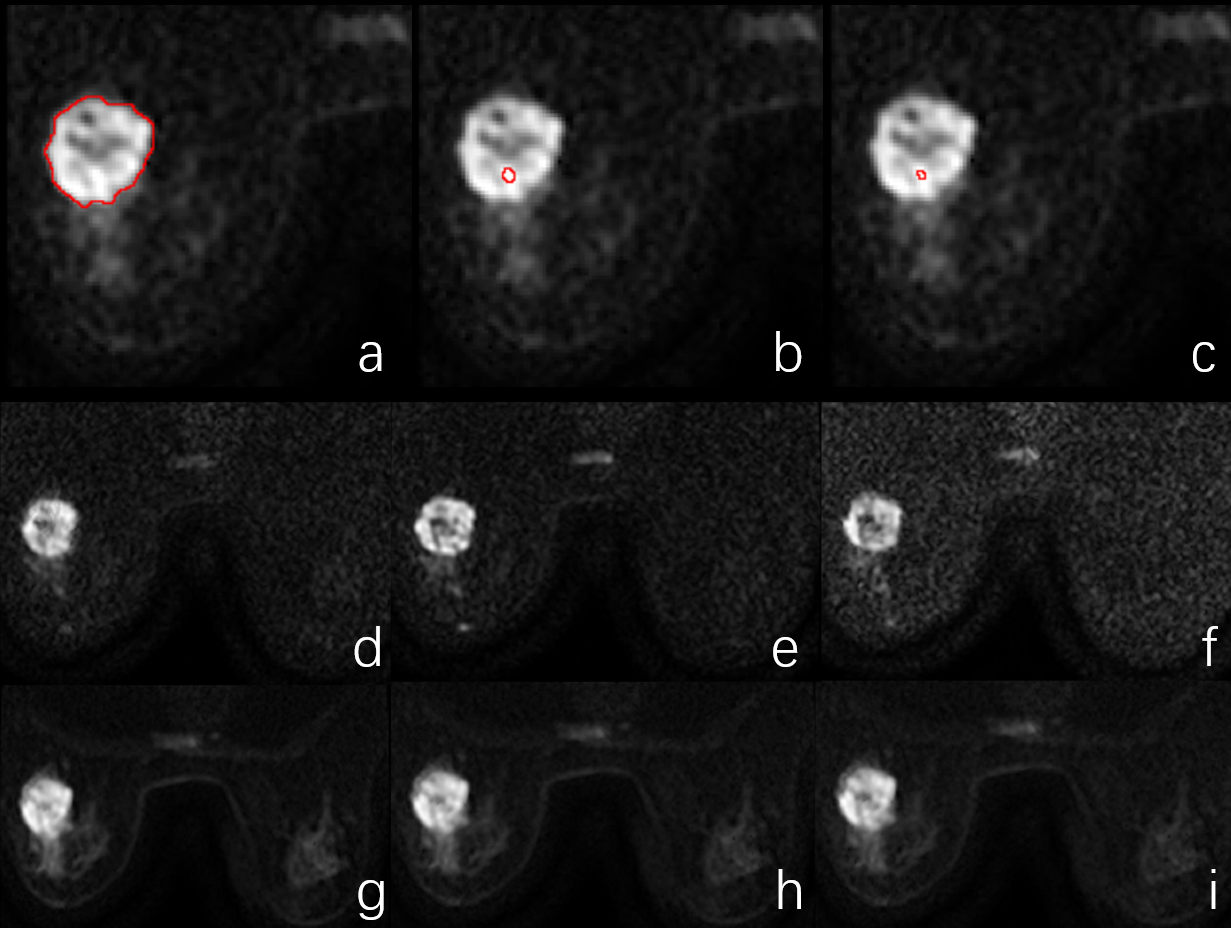
23 females with ultrasound-suspected breast cancer at the average age of(48.52±11.63)years were recruited for totally 32 lesions and underwent MR examination on 1.5T MR scanner (Voyager,GE Healthcare,Milwaukee, U.S.A) using 8-channel breast coils. Single-shot spin echo echo-planar diffusion weighted imaging was conduct with the following parameters: TR/TE = 4000/50 ms, field of view = 40 cm, slice thickness/gap = 4/0, matrix size = 288 *120, 5 b-values = [0, 50, 100, 400, 800], 12 b-values = [0,50,100-400.800-2400]. Two radiologists independently subjectively assessed every lesion at five-point visual grading characteristic (VCG) score. The same-sized ROI was placed on the largest cross-section tumor DWIs with b values (800,1000 and1200 s/mm2) to obtain SNR (SIlesion/SDbackground), CNR (SIlesion - SIlesion/SDobturator internus), and SIR (signal-intensity-ratio = SIlesion/SDconlateral normal breast tissue). Three ROIs with size of the whole lesion, 10 mm2 as a part-lesion type and 3 mm2 as a point-type were placed on the largest cross-section tumor, contralateral normal gland, ipsilateral normal gland 2-centimeter-distal to lesions in avoidance of cysts, necrosis, and hemorrhage to retrieve ADC values computed based on scanned and synthetic DWIs with any two b values [0, (800, 1000, 1200) s/mm2]. Illustration of ROI position was shown in Figure 1(a-c). Statistics analysis was performed using SPSS 22.0. Intraclass correlation coefficient or Cohen’s Kappa was used to check interobserver consistency of objective and subjective assessment. Paired t or Wilcoxon signed test were tested for ADC values depending on data normality. P < 0.05 was considered statistically significant.Results
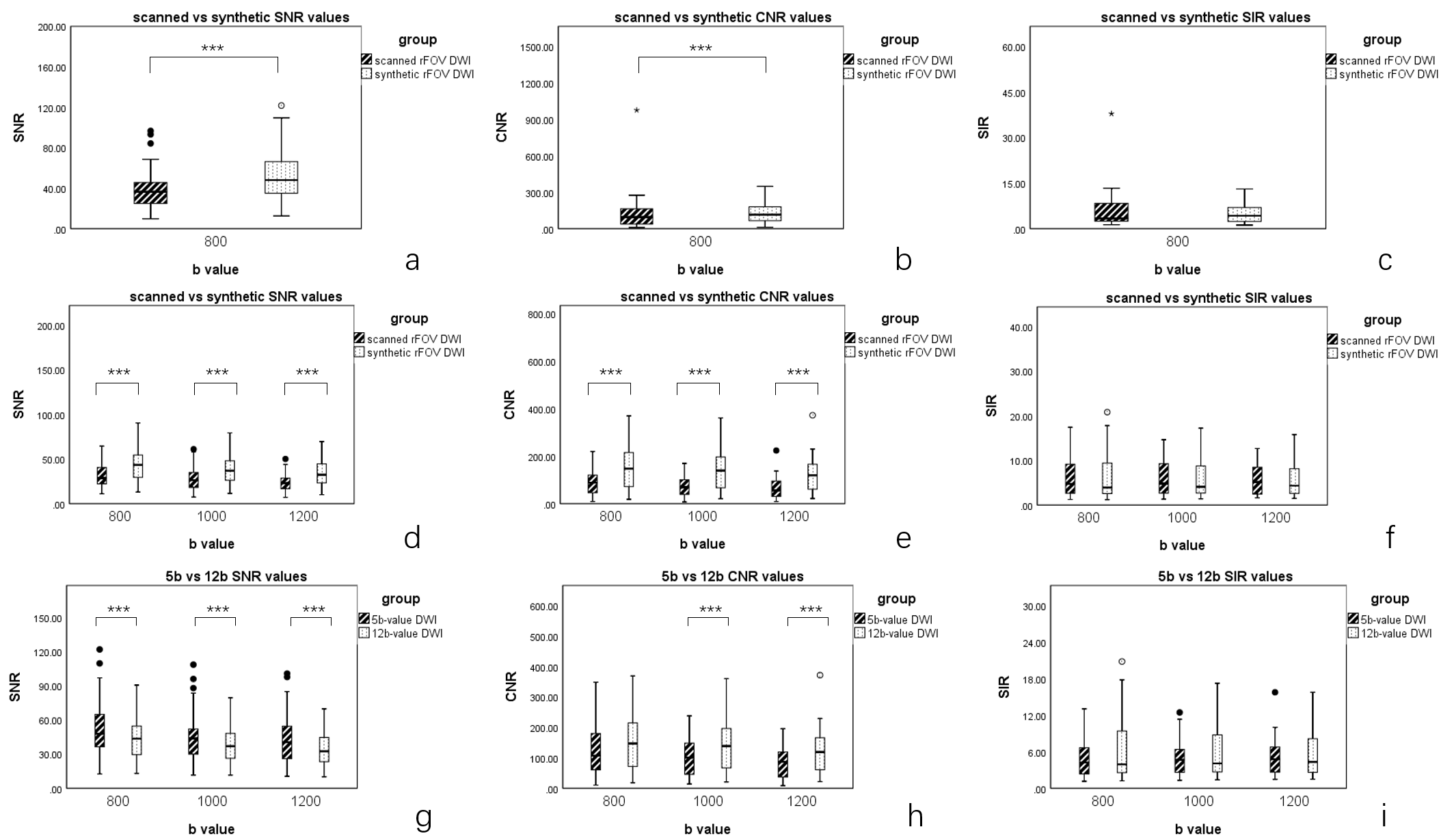
For subjective and objective evaluation on image quality, inter-observer and inter-modality consistency of scanned and synthetic DWIs with three different b-values was respectively moderate to good (Table 1), and overall subjective and objective assessment for image quality was higher on synthetic DWIs than scanned DWIs (Figure 1-2). SNR and CNR reduced as b-value increased (Figure 2). For quantitative assessment of ADC maps, histogram-derived parameters such as mean and median on lesions showed significant difference between scanned and synthetic DWIs (p < 0.05) (Table 2-3). Significant different ADC values were found between 5 b-value scanned and synthetic DWIs, 12 b-value scanned and synthetic DWIs and also 5 b-value synthetic and 12 b-value synthetic DWIs using different ROI measurements (Table 2-3). There was no significant difference between ipsilateral and contralateral normal breast tissues (Table 4). Different ROI measurement derived ADC values on the same DWIs showed significantly different mean and median (Table 2-3).Discussion
Our main findings showed better image quality, including subjective and objective assessment, of high-b-value syDWIs and manually-ROI-derived ADC values varied within the same DWIs and between scanned and synthetic DWIs. These results strengthen diagnosis confidence and elevate lesion detection rate. As shown in Figure 1(d-i), more clear breast structures were demonstrated on syDWIs due to computed with low-b-value DWI images. For lesions, ADC and computed using scanned and synthetic DWIs showed moderate to good consistency. SNR and CNR of synthetic DWIs were higher than scanned ones. On synthetic DWIs, less noise in normal breast tissue and more homogeneous gland particularly dense breast lowered missing breast cancer rate [5]. Consistent ADC and values could be used to determine benign or malignant tumors. In spite of several limitations in our study including small sample size, no exam for diagnosis performance, synthetic DWIs possess good features of scanned DWIs such as high signal intensity (SI) in display of tumor and can-be-used ADC and values.Acknowledgements
No acknowledgement found.References
[1] Baltzer P, Mann R M, Iima M, et al. Diffusion-weighted imaging of the breast-a consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group[J]. Eur Radiol, 2020, 30(3): 1436-1450.
[2] Bickel H, Polanec S H, Wengert G, et al. Diffusion-Weighted MRI of Breast Cancer: Improved Lesion Visibility and Image Quality Using Synthetic b-Values[J]. J Magn Reson Imaging, 2019, 50(6): 1754-1761.
[3] Newitt D C, Zhang Z, Gibbs J E, et al. Test-retest repeatability and reproducibility of ADC measures by breast DWI: Results from the ACRIN 6698 trial[J]. J Magn Reson Imaging, 2019, 49(6): 1617-1628.
[4] Whisenant J G, Romanoff J, Rahbar H, et al. Factors Affecting Image Quality and Lesion Evaluability in Breast Diffusion-weighted MRI: Observations from the ECOG-ACRIN Cancer Research Group Multisite Trial (A6702)[J]. J Breast Imaging, 2021, 3(1): 44-56.
[5] Daimiel Naranjo I, Lo Gullo R, Saccarelli C, et al. Diagnostic value of diffusion-weighted imaging with synthetic b-values in breast tumors: comparison with dynamic contrast-enhanced and multiparametric MRI[J]. Eur Radiol, 2021, 31(1): 356-367.
[6] Sartoretti T, Sartoretti E, Wyss M, et al. Diffusion-weighted MRI of ischemic stroke at 3T: Value of synthetic b-values[J]. Br J Radiol, 2021, 94(1121): 20200869.
Figures
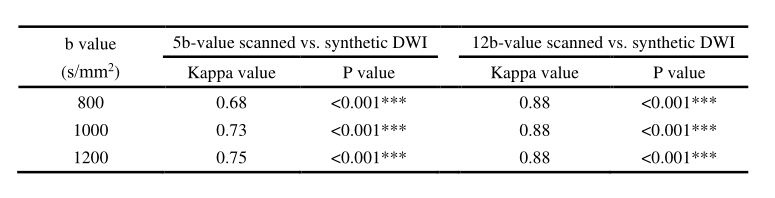
Table 1 Subjective evaluation of 5b- and 12b- scanned vs synthetic DWIs.
Note.—*, p<0.05; **, p<0.01; ***, p<0.001
Abbreviations: DWI, diffusion-weighted imaging.

Table 2 Comparison of ADC values measured at 3 ROIs with 5b-value DWI schemes (b=800 s/mm2)
Note.—*, p<0.05; **, p<0.01; ***, p<0.001
Abbreviations: DWI, diffusion-weighted imaging.
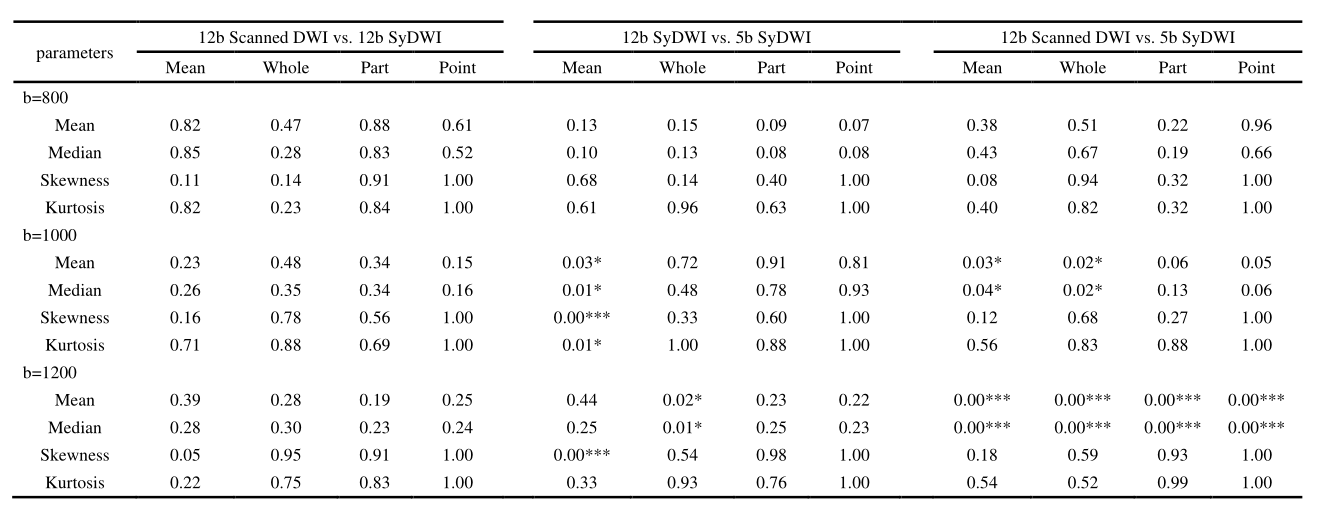
Table 3 Comparison of ADC values measured at 3 ROIs with 12b-value DWI schemes
Note.—*, p<0.05; **, p<0.01; ***, p<0.001
Abbreviations: DWI, diffusion-weighted imaging.
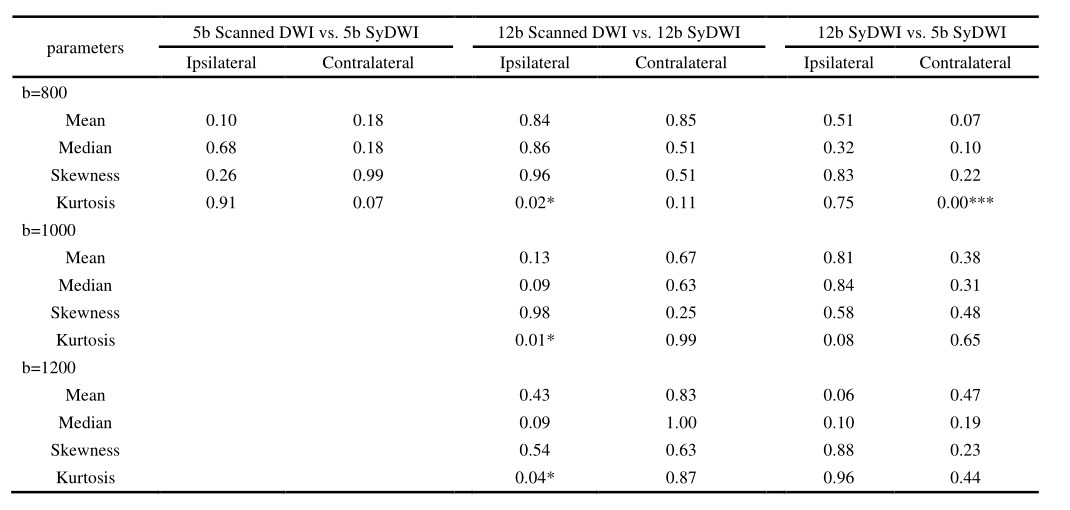
Table 4 Comparison of ADC values of normal glands measured at ROIs with different DWI schemes
Note.—*, p<0.05; **, p<0.01; ***, p<0.001
Abbreviations: DWI, diffusion-weighted imaging.