2557
MultiBand Acquisition for Breast Restriction Spectrum Imaging1Radiology, University of California, San Diego, San Diego, CA, United States, 2Global MR Application and Workflow, GE Healthcare, Boston, MA, United States, 3Radiation medicine, University of California, San Diego, San Diego, CA, United States, 4Bioengineering, University of California, San Diego, San Diego, CA, United States, 5Neurosciences, University of California, San Diego, San Diego, CA, United States
Synopsis
Keywords: Breast, Diffusion/other diffusion imaging techniques
Diffusion-weighted imaging holds great potential in improving specificity in breast cancer MRI, potentially reducing the number of unnecessary biopsies. Additionally, breast cancer screening protocols would benefit from high-resolution DWI acquisitions, especially in the through-plane direction. In this abstract we explore multi-slice excitation as a promising parallel-imaging tool to improve through-plane image resolution.Introduction
Diffusion-weighted imaging (DWI-MRI) has potential for screening for breast cancer without IV contrast, and for improving specificity in exams with contrast. Existing diffusion protocols often focus on high in-plane resolution with low through plane resolution1. Diffusion would be more useful for breast imaging with isotropic high resolution. More advanced DWI models, such as restriction spectrum imaging (RSI), aims at separating information in tissues in pools of different diffusion degrees. Recently, a breast-specific RSI model has been developed for breast lesion characterization2,3. Such acquisitions require using high b-values (typically up to 3,000-4,000 s/mm2) which can take time, driving increased slice thickness. Relatively large slice thickness (~4 – 6 mm)4 is a common problem not only for RSI but for all diffusion imaging techniques. Consequently, there is a need for high-resolution isotropic DWI in screening protocols. Achieving high in-plane resolutions has been achieved5. However, improving through-plane resolution is challenging. One of the promising parallel-imaging solutions to keep thin slices and cover the whole breasts in an acceptable time (approximately 5 minutes) is multi-slice excitation, MultiBand (MB). The purpose of the study is to explore isotropic high-resolution MB-DWI as a potential direction for breast cancer screening protocols in all three imaging planes. Image quality will be assessed and compared to conventional DWI acquisitions and to previous RSI studies.Methods
All images were acquired on a 3.0T scanner (GE Healthcare, USA) with a Sentinel 16-channel breast coil on two healthy patients.- Anatomical axial T2-weighted FSE images were acquired with the following parameters: TE/TR (ms): 105.8/4400; FOV: 360x360; matrix: 512x320; in-plane resolution: 0.703x1.125mm2; slice thickness: 3mm; Nslices: 50; acq time: 5min 04s.
- Conventional axial DWI images were acquired using Array coil Spatial Sensitivity Encoding (ASSET) with following parameters: TE/TR (ms): 58.5/4075; b-values (N directions): 0 (1), 100 (1), 600 (1), 800 (1) s/mm2; FOV: 340x340mm2; matrix: 128x128; in-plane resolution: 2.7x2.7mm2; slice thickness: 5mm; Nslices: 40; Z-dir coverage: 20cm; acq time: 3min 56s.
- Multi-shell DWI for RSI images were acquired using Echo-Planar Imaging (EPI) with the following parameters: TE/TR (ms): 82.7/9200; b-values (N directions): 0 (2), 500 (6), 1500 (6), 4000 (15) s/mm2; MB factor: 3; FOV: 320x320mm2; matrix: 96x96; in-plane resolution: 3.33x3.33mm2; slice thickness: 5mm; Nslices: 40; Z-dir coverage: 20cm; acq time: 4min 36s. ·
- High-resolution DWI-MB acquisition parameters were set as follows: TE/TR (ms): 79.6/9000; b-values (N directions): 0 (1), 800 (4), 1500 (4), 3000 (4) s/mm2; MB factor: 3; FOV: 360x360mm2; matrix: 180x180; in-plane resolution: 2.0x2.0mm2; slice thickness: 2mm; Nslices: 111; Z-dir coverage: 22.2cm; acq time: 4min 48s. Phase encoding direction: LR.
$$SNR_{S_0} = \frac{S_0}{\sqrt{\frac{2}{4-π}}σ_{noise}}$$
Where S0 is the signal intensity and σnoise is the standard deviation of the noise.
Results
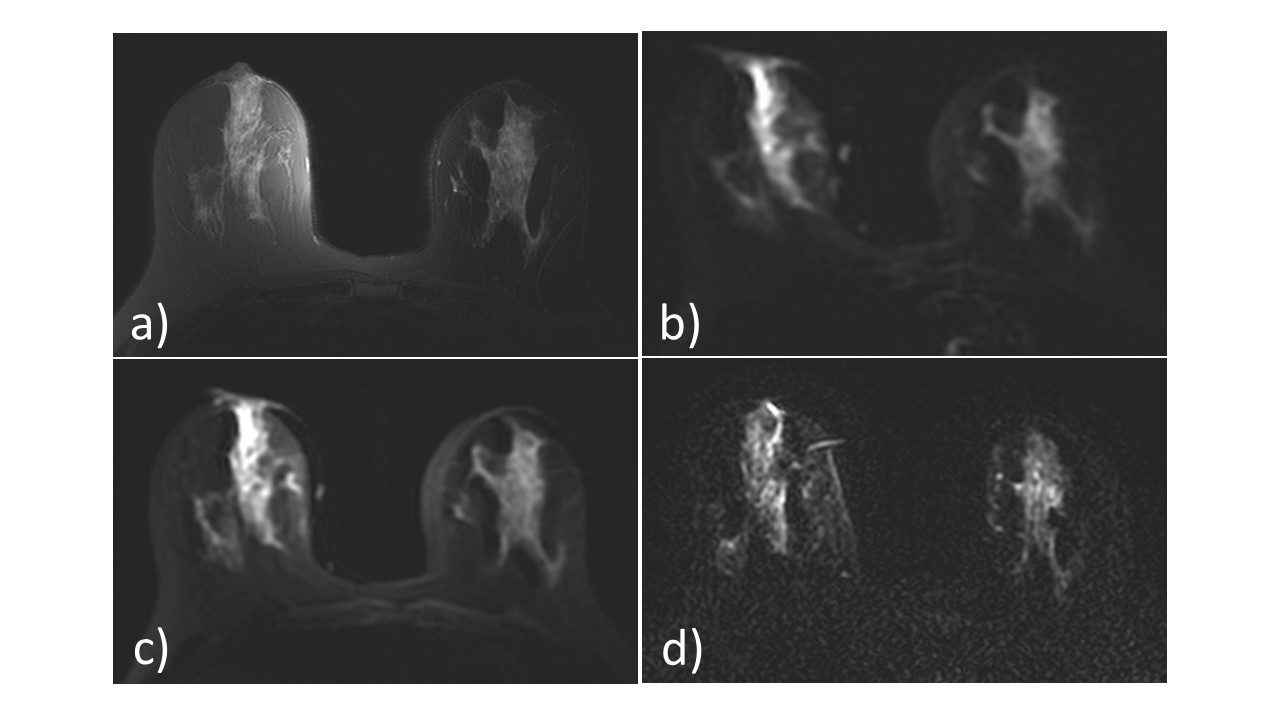
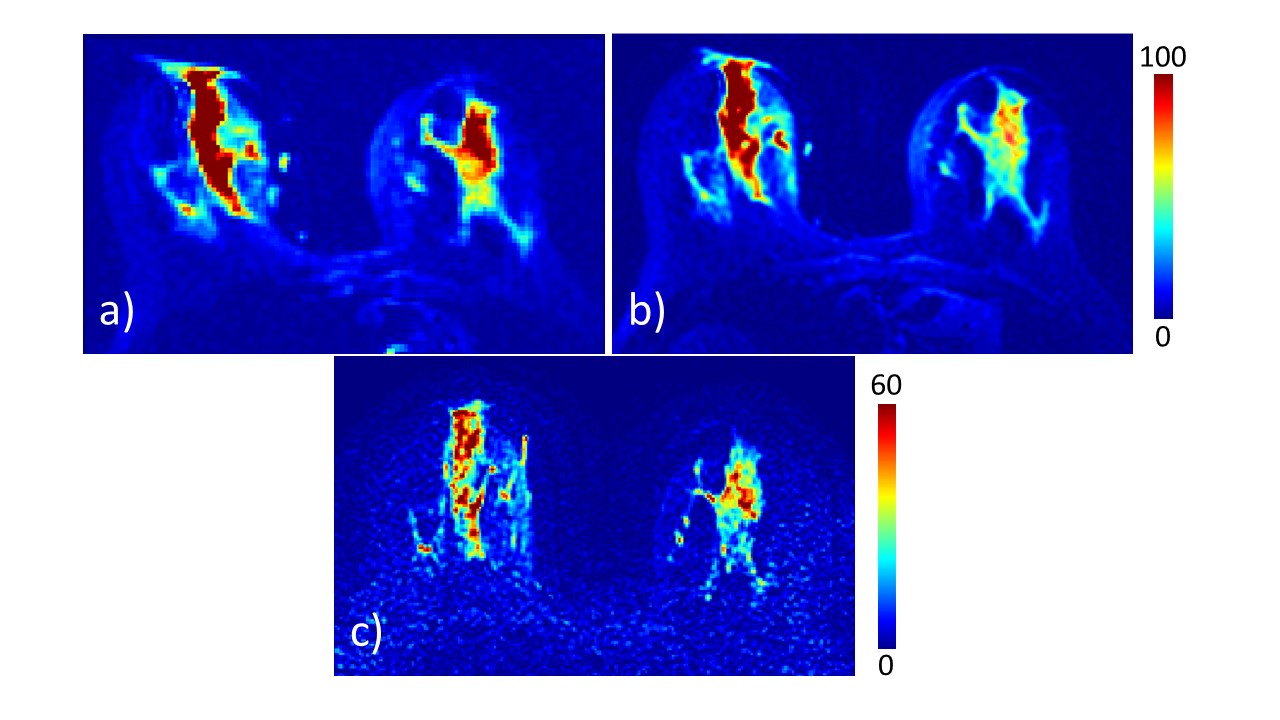
Figure 1 shows anatomical T2, Full FOV RSI, conventional DWI, as well as MB-DWI with LR phase encoding direction. All images represented are with b = 0 s/mm2. Voxel volumes were 36.45, 55.45 and 8mm3 for conventional, RSI and high-resolution MB-DWI. SNR maps for the different techniques are displayed on Figure 2.At b = 0 s/mm2, SNR was measured in fibroglandular tissue and was 99.2 ± 28.3 for full FOV RSI, 65.1 ± 9.7 for conventional DWI and 38.6 MB-DWI with LR phase encoding direction. Fat suppression was better in high-resolution MB-DWI.
Visually, MB-DWI images display good quality overall, with higher noise compared to the two other acquisitions, however.
Discussion
In this study, we propose an isotropic high-resolution DWI protocol for improved breast cancer diffusion weighted imaging. The methodology is based on multi-slice excitation, offering a solution to Z-direction breast coverage issues while using slices as thin as 2mm. In-plane resolution could be higher, and has been achieved before5. However, low through plane resolution limits the utility of the diffusion for breast imaging of small lesions. This is the first time 2mm slice thickness is performed for breast DWI in less than 5min and a valuable technique employ for future studies evaluation diffusion MRI in the screening population.One pitfall of higher resolution imaging is that the SNR decreases. Our high-resolution has voxels volumes 4 to 6 times smaller than with the two other methods, for a 2 to 3-fold decrease of the SNR. Adequate SNR along with high-resolution is mandatory for improving breast cancer diagnosis. This is a promising result. Moreover, reduced-FOV RSI has demonstrated better performances than full-FOV RSI2, so high-resolution rFOV should be implemented and tested as well.
Next steps of the project will include application of this technique on a larger patient population both for screening and for known diagnosis of breast cancer.
Acknowledgements
No acknowledgement found.References
1. Baltzer P, Mann RM, Iima M, et al. Diffusion-weighted imaging of the breast-a consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group. Eur Radiol. 2020;30(3):1436-1450. doi:10.1007/s00330-019-06510-3
2. Rodríguez-Soto AE, Fang LK, Holland D, et al. Correction of Artifacts Induced by B0 Inhomogeneities in Breast MRI Using Reduced-Field-of-View Echo-Planar Imaging and Enhanced Reversed Polarity Gradient Method. J Magn Reson Imaging. 2021;53(5):1581-1591. doi:10.1002/jmri.27566
3. Andreassen MMS, Rodríguez-Soto AE, Conlin CC, et al. Discrimination of Breast Cancer from Healthy Breast Tissue Using a Three-component Diffusion-weighted MRI Model. Clin Cancer Res. 2021;27(4):1094-1104. doi:10.1158/1078-0432.CCR-20-2017
4. Partridge SC, McDonald ES. Diffusion weighted MRI of the breast: Protocol optimization, guidelines for interpretation, and potential clinical applications. Magn Reson Imaging Clin N Am. 2013;21(3):601-624. doi:10.1016/j.mric.2013.04.007
5. Taviani V, Alley MT, Banerjee S, et al. High-resolution diffusion-weighted imaging of the breast with multiband 2D radiofrequency pulses and a generalized parallel imaging reconstruction. Magn Reson Med. 2017;77(1):209-220. doi:10.1002/mrm.26110
6. Dietrich O, Raya JG, Reeder SB, Reiser MF, Schoenberg SO. Measurement of signal-to-noise ratios in MR images: Influence of multichannel coils, parallel imaging, and reconstruction filters. J Magn Reson Imaging. 2007;26(2):375-385. doi:10.1002/jmri.20969
Figures