2552
Diagnostic value of 5b and 2b-value-DWI in breast tumors: comparison with combined MRI1Department of Diagnostic Imaging and Nuclear Medicine, Graduate School of Medicine, Kyoto University, Kyoto, Japan, 2Institute for Advancement of Clinical and Translational Science, Kyoto University Hospital, Kyoto, Japan, 3Department of Diagnostic Radiology, Kitano Hospital, Tazuke Kofukai Medical Research Institute, Osaka, Japan, 4Department of Breast Surgery, Kitano Hospital, The Tazuke Kofukai Medical Research Institute, Osaka, Japan, 5Department of Clinical Radiology Service, Kitano Hospital, The Tazuke Kofukai Medical Research Institute, Osaka, Japan, 6Department of Diagnostic Radiology, Kansai Electric Power Hospital, Osaka, Japan
Synopsis
Keywords: Breast, Diffusion/other diffusion imaging techniques
We propose a DWI-reading method based on the an adjusted BI-RADS lexicons using five b values of 0, 200, 800, 1000, and 1500 s/mm2 (5b-value-DWI). Diagnostic performance was evaluated in comparison with BI-RADS lexicons from standard BI-RADS DCE MRI and a DWI-reading method based on the adjusted BI-RADS lexicons using two b values of 0, 800 s/mm2 (2b-value-DWI).Our proposed DWI reading methods achieved diagnostic performance comparable to the standard BI-RADS. With higher sensitivity and NPV in 5b-value-DWI compared to 2b-value-DWI, DWI reading with 5b-values has the potential to increase diagnostic confidence in differentiating malignant and benign breast tumors.
Introduction
DWI has been widely used for the diagnosis and monitoring of breast lesions. Although DWI is routinely used for clinical breast MRI at many hospitals, it is not included in the BI-RADS-MRI assessment [1-3]. The integration of DWI and DCE has been shown to improve specificity rather than sensitivity [2,4]. Thus, we hypothesized that 5b-value-DWI might improve DWI sensitivity, and proposed a DWI-reading method based on an adjusted BI-RADS lexicon (e.g., a slight modification of the BI-RADS lexicon by adjusting to that of DWI [5]) using five b values of 0, 200, 800, 1000, and 1500 s/mm2 (5b-value-DWI). Its diagnostic performance was evaluated in comparison with BI-RADS lexicons from standard DCE MRI and a 2b-value-DWI-reading method based on adjusted BI-RADS lexicons using two b values of 0, 800 s/mm2 (2b-value-DWI). ADC values using b values of 0 and 800 s/mm2 (ADC0-800) and shifted ADC values using b values of 200 and 1500 s/mm2 (sADC200-1500) were also calculated, and compared between malignant and benign lesions.Material and Methods
Study population: This IRB-approved prospective study included 107 patients with suspected breast cancer. There were no lesions in 35 patients, whereas 23 patients had lesions in both breasts. Thus, lesions from 95 independent breasts (corresponding to 72 affected patients) were further analyzed.MRI acquisition: MR images were obtained on a 3-T MRI system (Achieva 3T;Philips) equipped with a dedicated 7-channel breast array coil. The imaging protocol included T1WI, fat-suppressed T2WI, DCE-T1WI, and DWI. Breast DW images were acquired using b values of 0, 200, 800, 1000, and 1500 s/mm2) on 3T MRI; repetition time/echo time, 12 500/79 ms; flip angle, 90°; field of view, 350×350 mm; matrix, 112×145; slice thickness, 4.0mm.
Qualitative assessment: Two independent radiologists, blinded to all other information, assessed the lesion category on the DW images on 2b and 5b-value-DWI according to an adjusted BI-RADS lexicon, with an interval of more than 2 weeks [5]. More than 2 weeks after DWI-based reading, they independently read breast MR images, including DCE T1WI, non-contrast T1WI,T2WI and 5b-value-DWI for the combined MRI. (Adjusted) BI-RADS categories of 1 through 3 were classified as negative (non-malignant), and categories of 4 and 5 were classified as positive for malignancy. ROC analysis was performed in lesion classification for 2b-value-DWI, 5b-value-DWI alone and in combination with the BI-RADS classification based on combined MRI. Sensitivity, specificity, PPV, NPV, and AUC were calculated using the Youden index, maximizing the sum of sensitivity and specificity.
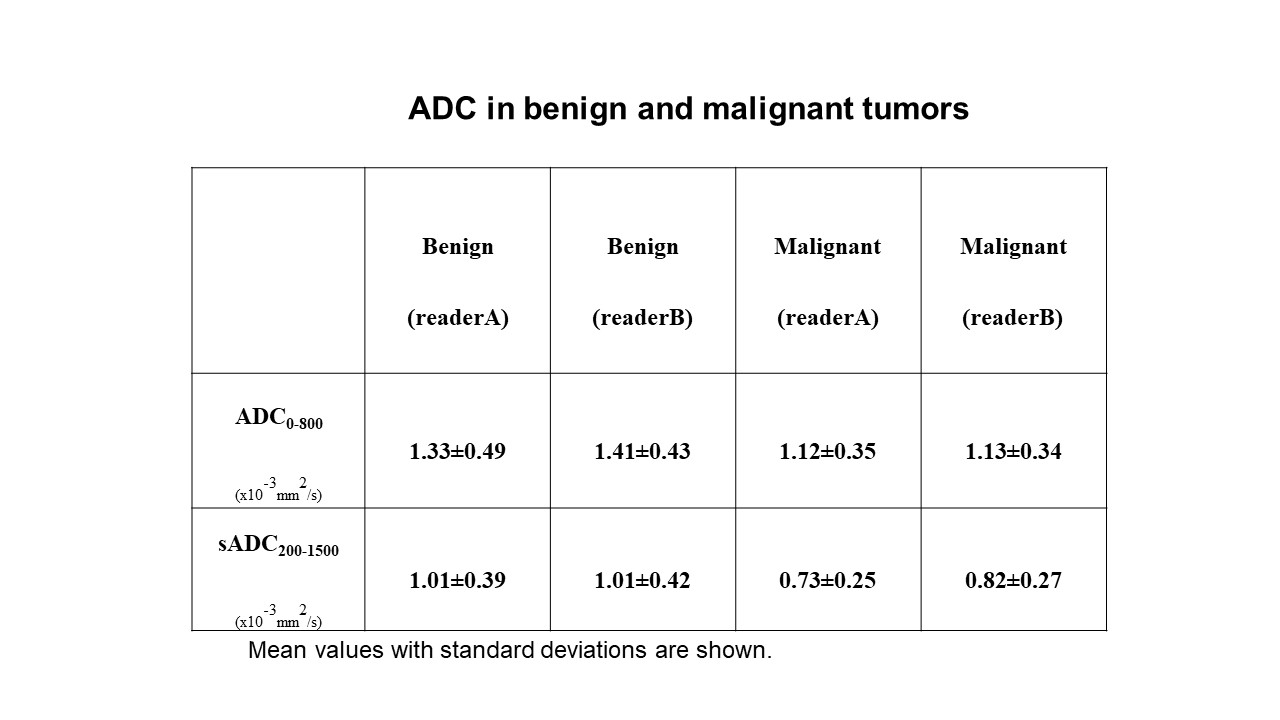
Quantitative assessment: ADC values using b values of 0 and 800 s/mm2 (ADC0-800) and shifted ADC values using b values of 200 and 1500 s/mm2 (sADC200-1500) were also calculated, and ADC values between malignant and benign lesions were compared using the Mann-Whitney test.
The statistical tests were performed using commercial software (Medcalc).
Results
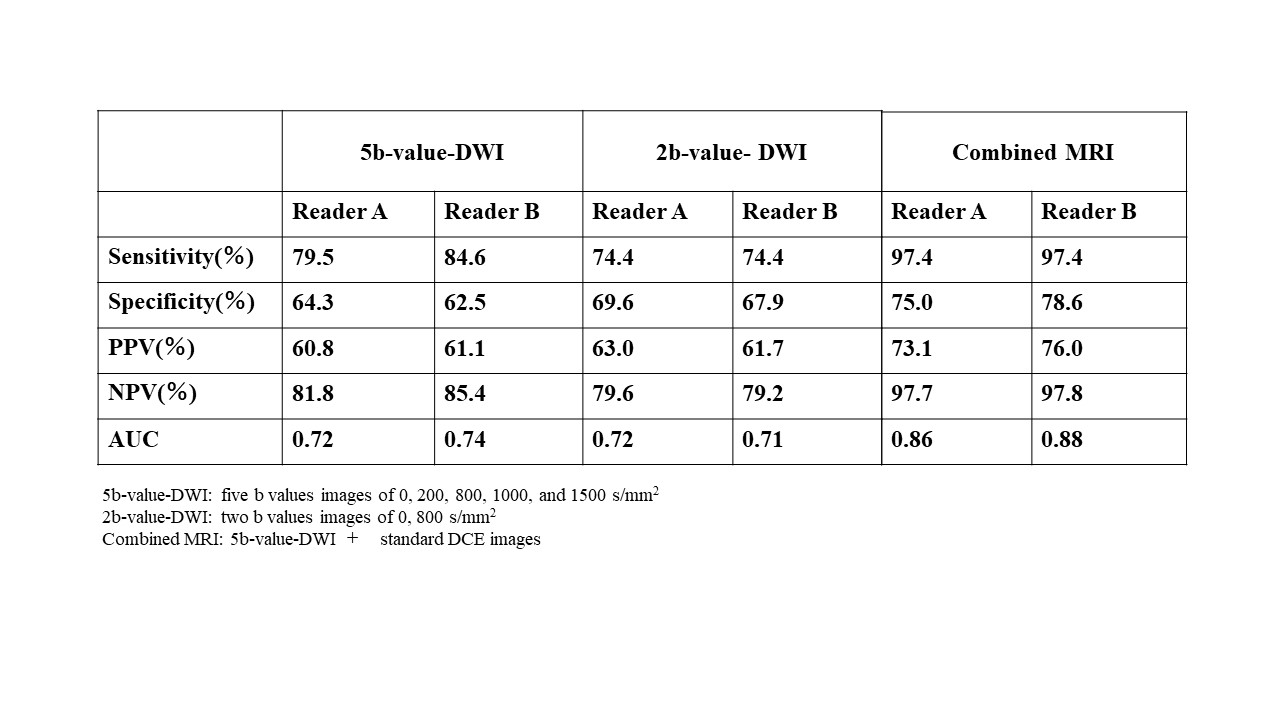
Ninety-five breast lesions (39 malignant and 56 benign) were evaluated. The diagnostic performance of readers A and B for 5b and 2b-value-DWI-based reading and combined MRI reading is summarized in Table 1. Representative cases are shown in Figure. A total of 13 and 9 lesions (for readers A and B) were detected only in combined MRI and were missed in 5b and 2b-value-DWI, and most cases were small and non-mass lesions. 12 and 13 lesions (for readers A and B) were detected using 5b-value-DWI, not found in combined MRI, which corresponded to false-positive lesions. Overall, the diagnostic performance of combined MRI (AUC:0.86-0.88) was significantly higher than 5b-value (0.72-0.74) or 2b-value (0.72-0.71) DWI (p<0.01). Sensitivity and NPV of 5b-value- DWI (79.5, 84.6% and 81.8, 85.4% for readers A and B, respectively) tended to be superior to 2b-value- DWI (74.4% for both readers, and 79.6, 79.2%, respectively). Specificity and PPV of 5b-value- DWI (64.3,62.5% and 60.8, 61.1%) tended to be inferior to 2b-value- DWI (69.6, 67.9%, 63.0, 61.7%, respectively). All ADC values differentiated malignant and benign breast lesions (p<0.01) (Table 2).Discussion & Conclusion
In this study, we qualitatively and quantitatively evaluated breast lesions using 5b-value-DWI (DW images with multiple b values) based on an adjusted DWI lexicon. Our proposed DWI reading methods achieved diagnostic performance comparable to the standard BI-RADS. The lesion detection rate increases when checking DW images at b = 800, 1000, and 1500s/mm2 continuously, as with increased b values, lesions might become more clearly visualized in contrast to the background on DW images, which might improve diagnostic performance in terms of lesion detection. 5b-value-DWI tended to have higher sensitivity and NPV than 2b-value-DWI, while specificity and PPV tended to be inferior. Standard breast DWI (using 2b-values) has been known to have lower sensitivity and higher specificity compared to DCE-MRI [6], and 5b-DWI might have the potential to complement its diagnostic performance. All ADC values in malignant and benign breast lesions significantly differed, which might also improve the diagnostic performance using breast DWI. Lesion detection with 5b-value-DWI was inferior to that with combined MRI, possibly due to some small or non-mass lesions being missed on 5b-value- DWI. We have found a higher sensitivity and NPV of 5b-value-DWI than 2b-value-DWI without no significant difference, which requires further investigation to confirm this result. Still, 5b-value-DWI reading methods might increase diagnostic confidence in differentiating malignant and benign breast tumors.Acknowledgements
We would like to acknowledge Denis Le Bihan, MD, PhD , Rie Ota, MD, and Akane Ohashi MD, PhD for their valuable advice. This work was supported by AMED under Grant Number JP18ck0106454h0001.References
1. Shi, R.Y., et al., Breast Lesions: Diagnosis Using Diffusion Weighted Imaging at 1.5T and 3.0T-Systematic Review and Meta-analysis. Clin Breast Cancer, 2018. 18(3): p. e305-e320.
2. Zhang, L., et al., Accuracy of combined dynamic contrast-enhanced magnetic resonance imaging and diffusion-weighted imaging for breast cancer detection: a meta-analysis. Acta radiologica, 2016. 57(6): p. 651-660.
3. Iima, M., et al., Diffusion MRI of the breast: Current status and future directions. Journal of Magnetic Resonance Imaging, 2019.
4. Goto, M., et al., Adding a Model-free Diffusion MRI Marker to BI-RADS Assessment Improves Specificity for Diagnosing Breast Lesions. Radiology, 2019. 292(1): p. 84-93.
5. Kishimoto AO, Kataoka M, Iima M, et al. The comparison of high-resolution diffusion weighted imaging (DWI) with high-resolution contrast-enhanced MRI in the evaluation of breast cancers. Magnetic Resonance Imaging. 2020; 71:161-169.
6. Daimiel Naranjo, I., et al., Diagnostic value of diffusion-weighted imaging with synthetic b-values in breast tumors: comparison with dynamic contrast-enhanced and multiparametric MRI. European radiology, 2021. 31(1): p. 356-367.
Figures