2510
A novel VR based and motion tolerant capability for MR imaging of awake young children1Department of Perinatal Imaging, Centre for the Developing Brain, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Biomedical Image Technologies, ETSI Telecomunicación, Universidad Politécnica de Madrid and CIBER-BBN, ISCIII, Madrid, Spain, 3Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom, 4MRC Centre for Neurodevelopmental Disorders, King's College London, London, United Kingdom
Synopsis
Keywords: Normal development, New Devices
MRI examinations in young children are typically performed during natural or induced sleep to reduce distress and movement artefacts. However, those approaches have high failure rate and/or carry risks. We describe a system for MR imaging in awake children which combines immersive and interactive MR compatible virtual reality, eye tracking, and robust post-acquisition motion correction. We demonstrate effectiveness in a pilot study with a 2 year old child who used the system on 3 occasions for average 19.5 minutes. The described approach opens new possibilities for awake MR studies in young children for both clinical and research purposes.Introduction
A major challenge for MRI is the noisy and claustrophobic environment which makes it difficult to acquire images from specific populations, particularly young children who may become distressed or struggle to keep still. Scans are therefore often performed during sleep which is time-consuming and has high failure rates 1. In clinical practice, an alternative approach is to use sedation or anesthesia, both of which carry their own risks and require specialist resources 2. A further consideration for developmental neuroscience research is that imaging in induced or natural sleep precludes studies of the brain activity associated with awake behavior with methods like fMRI. Approaches to overcome this have included practice with mock scanners 3 or with in-bore video displays 4. However, those approaches have mixed success and ultimately do not remove the harsh realities of the MR examination itself, with the child still acutely aware of their surroundings in the scanner 5.With these challenges in mind, we have recently developed a novel Virtual Reality (VR) system which can immerse a child in an interactive virtual world during scanning 6. A key property of the system is that unusual sensations during scanning (such as scanner gradient noise or table movement) are incorporated into the VR experience, to avoid surprise or distress. The system also uses eye tracking and an adaptive calibration free gaze estimation algorithm that is robust to subject movement, which facilitates continuous interaction with the VR environment 6 and allows measurement of visual attention for fMRI analysis. Although this interaction method aims to reduce a child’s tendency to move, some degree of head movement will likely remain. To overcome the resulting image degradation, we have recently developed the DISORDER method which performs robust motion toleration image reconstruction 7. Putting these innovations together enables creation of a new system that can acquire high quality brain MR images from awake young children.
Methods
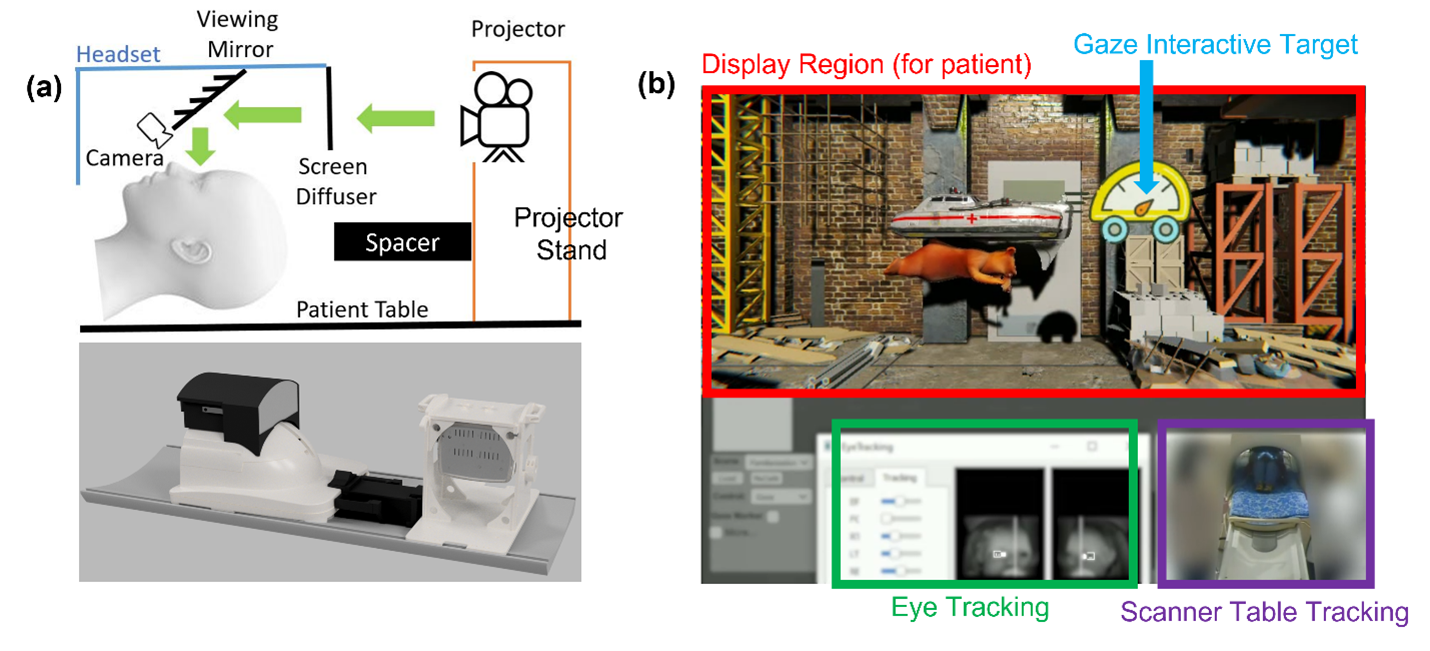
The VR system consists of a 3D printed coil top display (CTD) which mates precisely with the MR scanner head coil and is light-tight, thus preventing visual reminders of the child’s position in the scanner bore (figure 1). Two MR compatible video cameras (12M-I, MRC systems, Heidelberg DE) with infrared illuminator diodes are mounted inside the headset, and a wall mounted video camera in the MRI examination room monitors the patient table position. Video content is projected onto a diffuser screen in the CTD by a MRI compatible projector (SV-8000 MR-Mini, Avotec Inc, Florida USA) placed on the examination table behind the headset. Audio content is presented via optical noise cancelling headphones (OptoActive II, Optoacoustics Ltd, Israel).Once the child is positioned inside the head coil, they are immediately presented with immersive content which remains continuous throughout the examination. Content is developed using Unity (Unity Technologies) which enables easy customization for the preferences of each child. To interact, the child simply holds their gaze on items placed around the screen which trigger an action such as playing a game, watching a video, or interacting with a character or object. A progressive calibration algorithm which exploits the additional information from each new visual fixation ensures accurate gaze estimation even during head movement 8. To maintain congruence of the VR world with the child’s sensory experience, scanner table movement is reflected by a moving visual perspective in their VR experience and scanner gradient noise is matched by elements in the visual scene (such as a construction site). Motion correction of acquired images is performed retrospectively using the DISORDER framework which is based on distributed and incoherent sampling orders, enabling resilience to head motion by encoding redundancy in the data 7. Pilot data was collected using the described system with a 2 year old healthy male child using a Philips Achieva 3T scanner and a 32ch head coil (Phillips Healthcare, Best NL) (figure 2).
Results
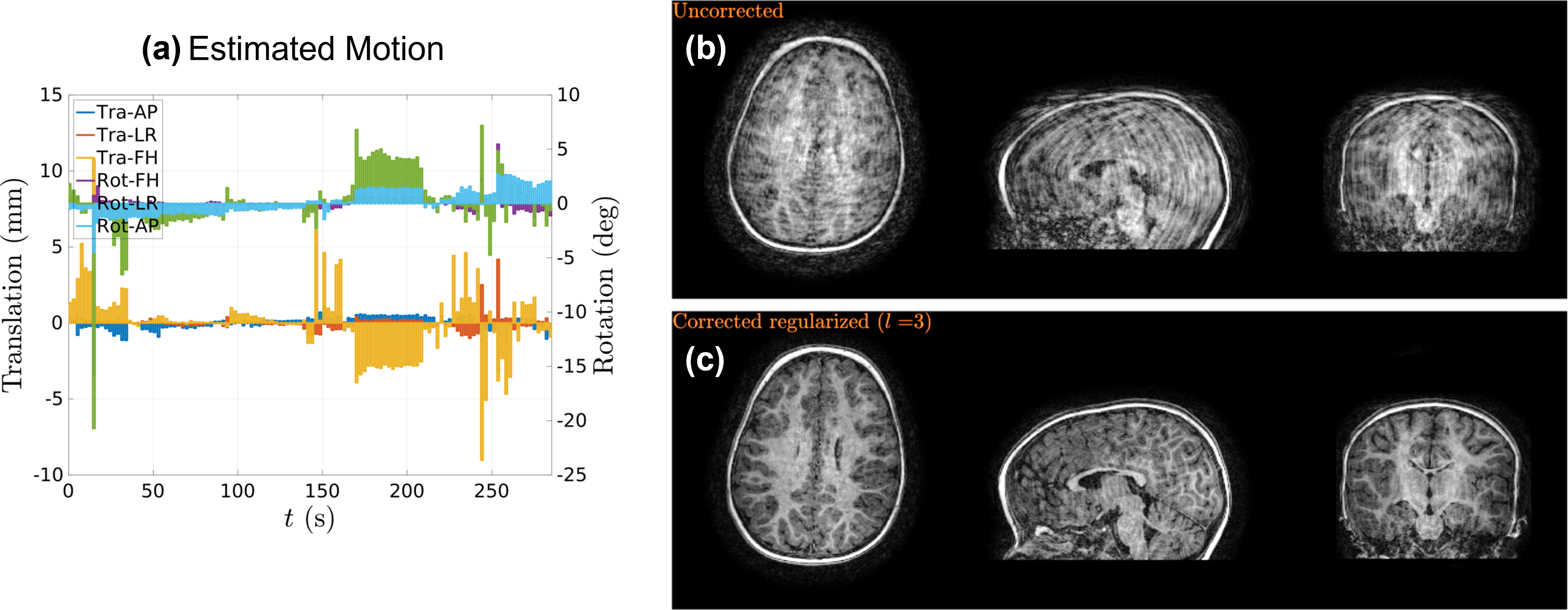
The child in our pilot study used the system inside the scanner bore in 2 sessions lasting 17 and 22 minutes each. He did not require instruction for how to use the system and was able to intuitively interact with and control it immediately after entering the VR world. He was not distressed at any point during use, so sessions were only stopped when it was noted that head movement had increased suggesting that he had become bored.In each session a high resolution MPRAGE scans, and two TSE T2-weighted images were acquired over ~16 minutes whilst the child used the system. Despite residual head movement during image acquisition (maximum displacement: >5mm translation and >5 degrees rotation), DISORDER reconstruction provided brain images suitable for clinical reporting and volumetric analysis (figure 3).
Discussion and Conclusions
We describe and demonstrate effectiveness of a novel framework which enables MRI scanning of awake young children based on an immersive VR experience and motion tolerant imaging methods. Our approach opens new possibilities for awake MR studies in young children for both clinical and research purposes, potentially reducing the need for non-trivial interventions like anesthesia and enabling a new generation of MR based studies of awake brain processing in this formative period of life.Acknowledgements
This work was supported by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London and/or the NIHR Clinical Research Facility. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health fand Social Care. TA was supported by funding from a Medical Research Council (MRC) Translation Support Award [MR/V036874/1]. ADE and TA received funding support from the MRC Centre for Neurodevelopmental Disorders, King’s College London [MR/N026063/1].References
[1]. Copeland A, Silver E, Korja R, et al. Infant and child MRI: a review of scanning procedures. Front Neurosci 2021; 15:666020.
[2]. Lawson GR. Controversy: sedation of children for magnetic resonance imaging. Arch Dis Child 2000; 82:150–3.
[3]. Suzuki A, Yamaguchi R, Kim L, Kawahara T, Ishii-Takahashi A. Effectiveness of mock scanners and preparation programs for successful magnetic resonance imaging: a systematic review and meta-analysis. Pediatr Radiol 2022; doi: 10.1007/s00247-022-05394-8.
[4]. Ellis CT, Skalaban LJ, Yates TS, Bejjanki VR, Cordova NI, Turk-Browne NB: Re-imagining fMRI for awake behaving infants. Nat Commun 2020, 11:4523.
[5]. Thieba C, Frayne A, Walton M, Mah A, Benischek A, Dewer D, Lebel C. Factors associated with successful MRI scanning in unsedated young children. Front Pediatr 2018; 6: 146.
[6]. Qian K, Arichi T, Price AN, Dall’Orso S, Eden J, Noh Y, Rhode K, Burdet E, Neil M, Edwards AD, Hajnal JV. An eye tracking based virtual reality system for use inside Magnetic Resonance imaging Systems. Scientific Reports 2021; 11: 16301(21).
[7]. Cordero-Grande L, Ferrazzi G, Teixeira RPAG, O'Muircheartaigh J, Price AN, Hajnal JV. Motion-corrected MRI with DISORDER: Distributed and incoherent sample orders for reconstruction deblurring using encoding redundancy. Magn Reson Med 2020 Aug;84(2):713-726.
[8]. Qian K, Arichi T, Edwards AD, Hajnal JV. A progressive calibration gaze interaction interface to enable to naturalistic fMRI experiments. Proceedings of the 29th ISMRM meeting, Vancouver Canada 2021.
Figures