2489
Diagnostic Performances of PETRA-MRA, TOF-MRA, and CTA in Assessing Intracranial Arterial Stenosis with DSA as a Reference Standard1Department of Magnetic Resonance, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2Department of Magnetic Resonance Imaging, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 3Siemens Healthineers Ltd., Beijing, China
Synopsis
Keywords: Stroke, MR Value, Vessels
This study compared the performance of three noninvasive techniques, namely, 3D pointwise encoding time reduction magnetic resonance angiography (PETRA-MRA), 3D time-of-flight (TOF) MRA and computed tomography angiography (CTA) in accurately measuring the degree of stenosis and lesion length in patients with intracranial arterial stenosis using DSA as the reference standard. This study demonstrated that the estimation of intracranial stenosis and lesion length by PETRA-MRA was more accurate and comparable with DSA than TOF-MRA and CTA. Therefore, PETRA-MRA is a promising noninvasive tool for the accurate assessment of ICAS.Introduction
Clinical evaluation of intracranial atherosclerosis requires the accurate assessment of intracranial arterial stenosis (ICAS). Currently, digital subtraction angiography (DSA), an invasive modality, is the gold standard for assessing ICAS. In this study we compared the performances of three non-invasive modalities, namely, 3D pointwise encoding time reduction magnetic resonance angiography (PETRA-MRA), 3D time-of-flight (TOF) MRA, and computed tomography angiography (CTA) in accurately measuring the degree of stenosis and lesion length in comparison with DSA in patients with ICAS.Materials and Methods
This single-center, prospective study included 52 patients (mean age 57 ± 11 years; 27 males) with ICAS (n=90). The patients underwent PETRA-MRA, TOF-MRA, CTA, and DSA within one month. All the patients underwent PETRA and TOF MRAs in a 3.0 T system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with a 64-channel head-neck coil, CTA in a 128-multislice Siemens Somatom AS + scanner (Siemens Healthcare, Erlangen, Germany), and DSA with a Phillips FD 20 Artis fixed digital angiographic system (Phillips Healthcare, Best, The Netherlands). The TOF-MRA parameters were as follows: TR/TE=20/3.69 ms; acquisition plane=axial; FOV=200 × 160 mm2; slice thickness=0.6 mm; and acquisition time=3 minutes 29 seconds. The PETRA-MRA parameters were as follows: TR/TE=3.32/0.07 ms; FOV=300 × 300 mm2; slice thickness=0.9 mm; and number of slices=320. The labeled scan was acquired with a saturation band proximal to the imaging volume. The control scan was acquired without the slice-selective saturation band. The total acquisition time of PETRA-MRA was 9 minutes 20 seconds. The PETRA-MRA images were subtracted from the two scans (control-labeled). The CTA scan parameters were as follows: quality reference=250 mA; tube voltage=120 kV; pitch=0.9; rotation time=0.5; collimation=128 × 0.6 mm2; slice thickness=0.6 mm; FOV=300 × 300 mm2. The DSA scan parameters were as follows: FOV=320 × 320 mm2; matrix=1024 × 1024. Four-vessel angiography was performed for all the patients and standard anteroposterior, oblique, and lateral views were acquired for all the arteries being investigated. The maximum intensity projections (MIPs) of the MRA and CTA images were performed at the Siemens workstation and evaluated using a 4-point scale (4=excellent, 1=not recognizable) by two radiologists with over 10 and 8 years of experience, respectively. The datasets with poor image quality (score ≤2) were excluded from the analyses. The degree of stenosis and lesion length estimates for all four imaging methods were measured independently by the two radiologists, who were blinded to the clinical information of the patients. The degree of stenosis was measured according to warfarin–aspirin symptomatic intracranial disease criteria1 as Stenosis (%) = (1−d/D) × 100%, where d is the diameter at maximal stenosis, and D is the diameter of the proximal normal segment. The lesion length was measured as stenosis length on the MRAs, CTA, and DSA. The normality of the continuous variables was analyzed using the Shapiro–Wilk’s test. The continuous variables were compared using the independent-samples t-test or the Mann–Whitney U test. The image quality scores were compared using the Kruskal–Wallis test. The intraclass correlation coefficients (ICCs) were used to assess the agreement between the MRAs or the CTA and the DSA measurements, and the inter-reader variabilities. The ICC value>0.80 indicated excellent agreement. The agreement of data was assessed further by the Bland–Altman analysis. The Spearman’s correlation coefficients were used to assess the agreements between the MRAs or CTA and the DSA measurements.Results
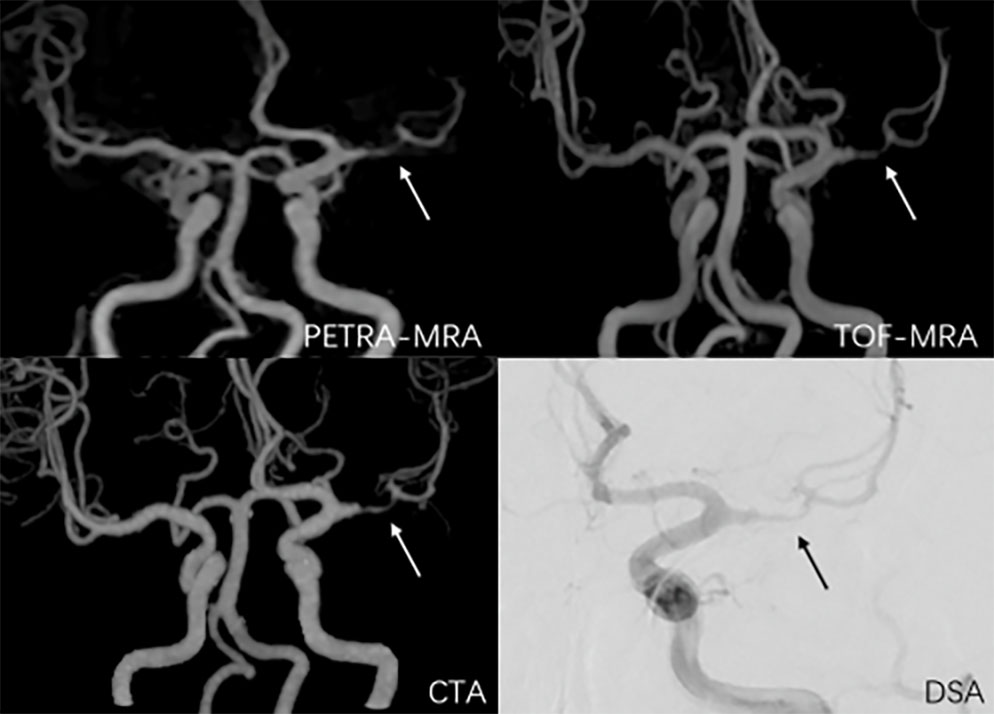
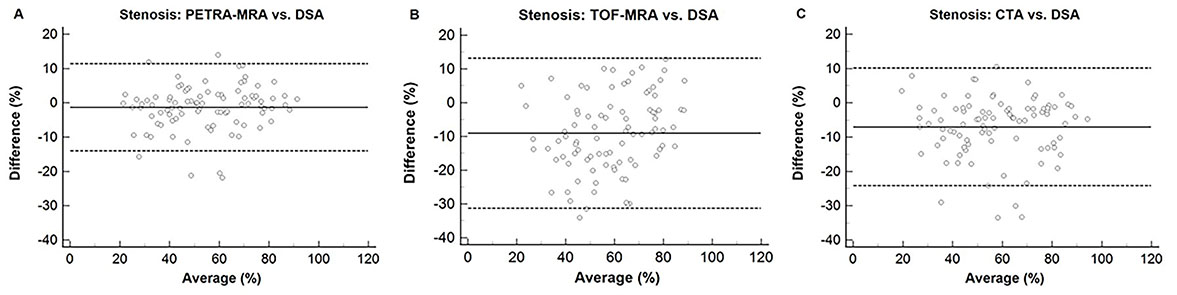
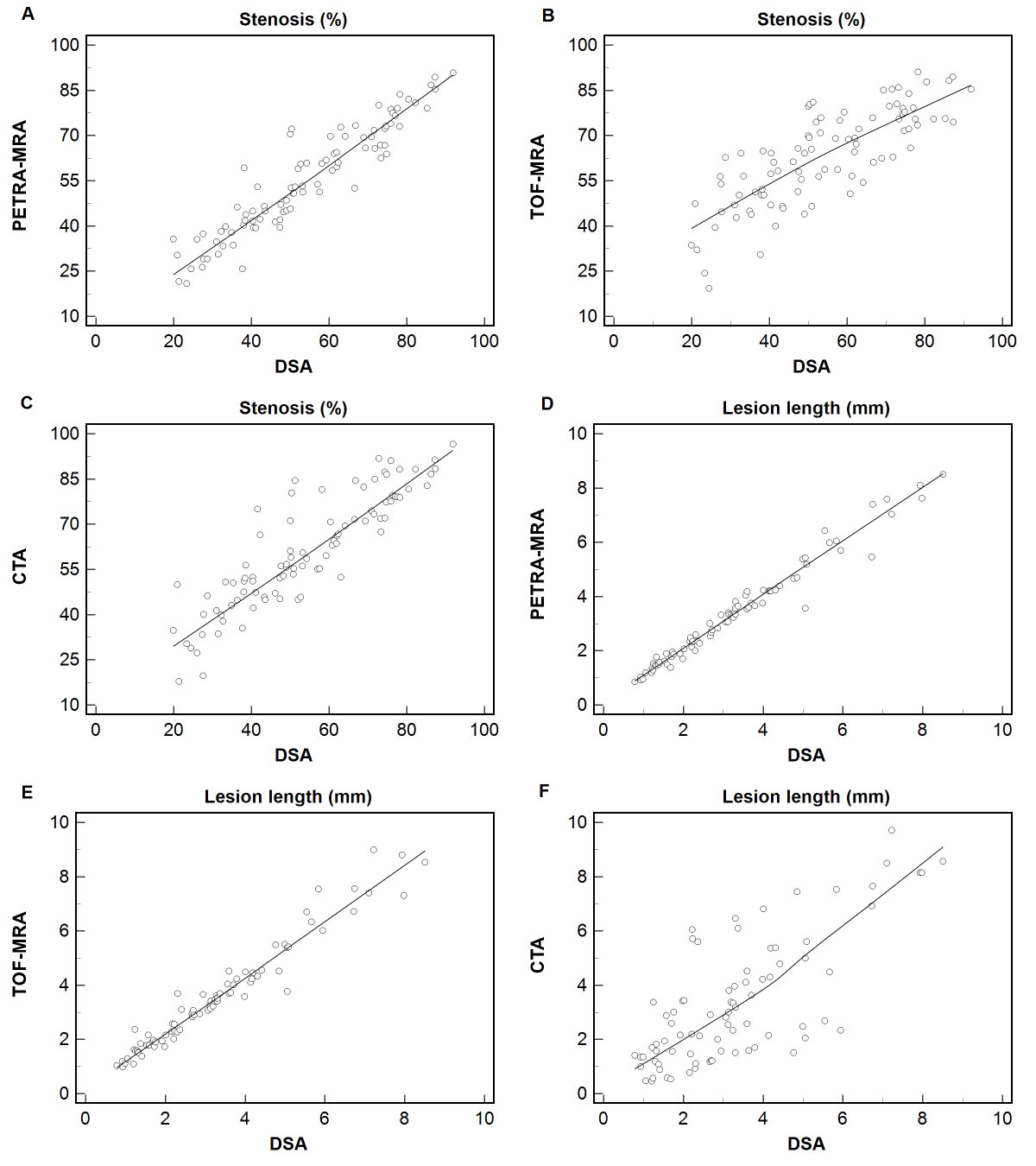
The inter-reader agreement for all the four imaging methods were excellent (ICCs > 0.80). PETRA-MRA, TOF-MRA, and CTA showed high image quality without any significant differences (P = 0.69) (Figure 1). Compared with DSA, PETRA-MRA was more consistent than TOF-MRA and CTA in measuring the degree of stenosis and the lesion length (Figure 2, 3). TOF-MRA and CTA significantly overestimated the degree of stenosis compared to the DSA (P <0.05 for both). However, PETRA-MRA did not overestimate the degree of stenosis compared to the DSA (P = 0.63).Discussion
This study showed that CTA and TOF-MRA overestimated the degree of stenosis compared to the DSA and PETRA-MRA. CTA measurements are highly sensitive to intracranial atherosclerotic plaque calcification and eddy current effects in the stenosis area, which increase the volume estimates from the local images2-4. TOF-MRA measurements are sensitive to the flow velocity and direction of blood flow5-7. In contrast, the PETRA-MRA sequence is less prone to flow artifacts and achieves highly homogeneous signals and increased SNR by combining the radial and Cartesian acquisitions of the k-space8,9. Furthermore, the echo time (TE<100 μs) was significantly shorter in the PETRA-MRA acquisitions to avoid phase dispersion errors, which are observed with longer TE10,11.Conclusion
PETRA-MRA is more accurate than TOF-MRA and CTA for evaluating intracranial stenosis and lesion length in ICAS patients when using DSA as a reference standard. Therefore, PETRA-MRA is a promising noninvasive tool for assessing ICAS.Acknowledgements
We are grateful to our patients and their families for their continued support during our study. At the same time, we acknowledge all the colleagues in this hospital for their support.References
1. Samuels OB, Joseph GJ, Lynn MJ, et al. A standardized method for measuring intracranial arterial stenosis. AJNR Am J Neuroradiol. 2000;21(4):643-646.
2. Liu Q, Huang J, Degnan AJ, et al. Comparison of high-resolution MRI with CT angiography and digital subtraction angiography for the evaluation of middle cerebral artery atherosclerotic steno-occlusive disease. Int J Cardiovasc Imaging. 2013;29(7):1491-1498.
3. Baradaran H, Patel P, Gialdini G, et al. Association between Intracranial Atherosclerotic Calcium Burden and Angiographic Luminal Stenosis Measurements. AJNR Am J Neuroradiol. 2017;38(9):1723-1729.
4. Bash S, Villablanca JP, Jahan R, et al. Intracranial vascular stenosis and occlusive disease: evaluation with CT angiography, MR angiography, and digital subtraction angiography. AJNR Am J Neuroradiol. 2005;26(5):1012-1021.
5. Igase K, Igase M, Matsubara I, et al. Mismatch between TOF MR Angiography and CT Angiography of the Middle Cerebral Artery may be a Critical Sign in Cerebrovascular Dynamics. Yonsei Med J. 2018;59(1):80-84.
6. Stock KW, Wetzel S, Kirsch E, et al. Anatomic evaluation of the circle of Willis: MR angiography versus intraarterial digital subtraction angiography. AJNR Am J Neuroradiol. 1996;17(8):1495-1499.
7. Pedraza S, Silva Y, Mendez J, et al. Comparison of preperfusion and postperfusion magnetic resonance angiography in acute stroke. Stroke. 2004;35(9):2105-2110.
8. Fu Q, Zhang XY, Deng XB, et al. Clinical evaluation of subtracted pointwise encoding time reduction with radial acquisition-based magnetic resonance angiography compared to 3D time-of-flight magnetic resonance angiography for improved flow dephasing at 3 Tesla. Magn Reson Imaging. 2020; 73:104-110. 9. Grodzki DM, Jakob PM, Heismann B. Ultrashort echo time imaging using pointwise encoding time reduction with radial acquisition (PETRA). Magn Reson Med. 2012;67(2):510-518.
10.Huang SY, Seethamraju RT, Patel P, et al. Body MR Imaging: Artifacts, k-Space, and Solutions-Erratum. Radiographics. 2015;35(5):1624.
11.Nielsen HT, Gold GE, Olcott EW, et al. Ultra-short echo-time 2D time-of-flight MR angiography using a half-pulse excitation. Magn Reson Med. 1999;41(3):591-599.
Figures