2472
Examination of the optimal imaging parameters for intracranial vessel wall bone-like imaging using FRACTURE
Keita Fukushima1, Miho Gomyo2, Kazuhiro Tsuchiya2,3, Shun Saito1, Tatsuya Yoshioka1, Takahiro Arai1, Takayuki Yonaha1, Ayaka Negishi1, Kosuke Sakaguchi1, Yuma Kumagai1, Makoto Obara4, Masatoshi Honda4, Takashi Namiki4, Yoshiyuki Nishimura4, Akihito Nakanishi1, and Kenichi Yokoyama2
1Section of Radiology, Kyorin University Hospital, Tokyo, Japan, 2Department of Radiology, Faculty of Medicine, Kyorin University, Tokyo, Japan, 3Department of Radiology, JR Tokyo General Hospital, Tokyo, Japan, 4Philips Japan, Ltd., Tokyo, Japan
1Section of Radiology, Kyorin University Hospital, Tokyo, Japan, 2Department of Radiology, Faculty of Medicine, Kyorin University, Tokyo, Japan, 3Department of Radiology, JR Tokyo General Hospital, Tokyo, Japan, 4Philips Japan, Ltd., Tokyo, Japan
Synopsis
Keywords: Blood vessels, Bone, bone-like imaging
Fast field echo resembling a CT using restricted echo-spacing (FRACTURE), which has been recently developed, has enabled visualization of calcification as well as cortical and spongy bones. However, it cannot be applied to intracranial vessel wall imaging due to insufficient suppression of cerebrospinal fluid (CSF) signal and intra-arterial flow artifact. In this study, by performing scans of an original phantom and healthy volunteers, we reveal that the application of multi-chunk and magnetization transfer contrast pulse to FRACTURE can suppress CSF signal and intra-arterial flow artifact and that FRACTURE can be efficiently applied to vessel wall bone-like imaging.Introduction
Traditional vessel wall imaging (VWI) cannot visualize calcified plaques due to low proton density and very short T2- and T2* values. A novel MR bone-like image, fast field echo resembling a CT using restricted echo-spacing (FRACTURE1), can visualize calcification, and cortical and spongy bones. However, this sequence cannot be applied to intracranial VWI due to insufficient suppression of cerebrospinal fluid (CSF) signal and intra-arterial flow artifact. This study aims to examine the optimal imaging parameters for applying the FRACTURE sequence to intracranial vessel wall bone-like imaging that can visualize calcified plaques.Methods
Our original phantom study and volunteer scan were performed using a 3-T MRI scanner (Ingenia Elition 3.0T X; Philips Healthcare, Best, the Netherlands) with a dS Head 32ch coil. The three-dimensional first field echo sequence (repetition time, 14 msec; echo time, 4.6~11.5 msec; echo interval, 2.3 msec; total echo, 4 echoes; flip angle, 15°; field of view, 150×150 mm; matrix size, 150×150; slice thickness, 1 mm; the number of slices, 120; the number of chunks, 1) was used as the original parameter for FRACTURE. First, we changed the number of chunks of the original parameters to multi chunks, then added a magnetization transfer contrast (MTC) pulse, and under each condition, the original phantom scan was performed 10 times, and the volunteer scan was performed on 10 healthy volunteers (8 men and 2 women; age, 30.4±3.3 years). Obtained images were grayscale inverted. The original phantom was made by placing a simulated vessel in the center of a 20 cm polyethylene case filled with a superabsorbent polymer and surrounding it with three layers simulating bone, brain parenchyma, and CSF. A simulated vessel was created by running water through a 3.1 mm tube at a speed of 60 cm/s to reproduce the intracranial major arteries. Gypsum (T1 value, 1888 msec; T2 value, no signal)2 was used for the simulated bone, 0.2 mmol/l gadolinium contrast medium dilution (T1 value, 766 msec; T2 value, 121 msec) was used for the simulated brain parenchyma, and 50-fold dilution of manganese chloride tetrahydrate (Bothdel Oral Solution 10) (T1 value, 766 msec; T2 value, 121 msec) was used for the simulated CSF (Figure 1). In the original phantom, regions of interest (ROI) were placed on three layers and simulated vessels. In the volunteer scan, ROIs were set to arteries (the middle cerebral artery, internal carotid artery [ICA], and basilar artery), bones (the clivus and mandibular head), CSF (the basilar and prepontine cisterns), and normal white matter as background noise. Furthermore, in the volunteer scan, we qualitatively evaluated both the signal uniformity of the ICA and the ability to visualization of the posterior edge of the dorsum sellae in contact with the CSF using a 5-point visual score (Figure 2). Under three imaging conditions: original, multi-chunks and multi-chunks combined with MTC pulse, contrast ratio (CR), and contrast-to-noise ratio (CNR) between bone and vessel and between bone and CSF were calculated in both the original phantom study and volunteer scan. The Kruskal-Wallis test was used for statistical analysis.Results
In the phantom study (Figure 1), the CR between bone and vessel using multi-chunks (4.78±0.23) and multi-chunks combined with MTC pulse (4.74±0.65) were significantly greater than that of the original parameter (3.43±0.18) (p < 0.05). Both CR and CNR between bone and CSF using multi-chunks combined with MTC pulse (CR, 1.52±0.07; CNR, 27.21±1.17) were significantly greater than those of using the original parameter (CR, 1.39±0.02; CNR, 22.38±0.11) and using multi-chunks (CR, 1.39±0.01; CNR, 21.00±1.77) (p < 0.05). In the volunteer study (Figures 3, 4), the CRs between bone and arteries using multi-chunks and multi-chunks combined with MTC pulse were significantly greater than that of using the original parameter. Both the CR and CNR between bone and CSF using multi-chunks combined MTC pulse were significantly greater than those of using the original parameter and using multi-chunks. In visual assessment (Figure 2), the score of signal uniformity of the ICA using multi-chunks combined with MTC pulse (3.9±0.5) was significantly higher than that of using the original parameter (1.5±0.1) and multi-chunks (1.9±0.2) (p < 0.05). The score of the depiction of the posterior margin of the dorsum sellae using multi-chunks combined with MTC pulse (5.0±0.0) was significantly higher than that of using the original parameter (1.5±1.0) and with multi-chunks (1.6±1.0) (p < 0.05).Discussion
The increase in CR of the vessel by using multi-chunks is presumably due to a decrease in the blood flow saturation effect and an increase in the in-flow effect. The use of MTC pulse caused a decrease in vascular signals due to a decrease in high-frequency pulses to the blood, a decrease in signals in the brain parenchyma, and accordingly a relative decrease in CSF signal. FRACTURE using multi-chunks combined with MTC pulse enables visualization of intracranial arterial calcifications (Figure 5).Conclusion
By combined use of multi-chunks and MTC pulse, FRACTURE can be efficiently applied as the intracranial vessel wall bone-like imaging.Acknowledgements
No acknowledgement found.References
- Johnson B, Alizai H, Dempsey M. Fast field echo resembling a CT using restricted echo-spacing (FRACTURE): a novel MRI technique with superior bone contrast. Skeletal Radiol. 2021;50(8):1705-1713.
- Niebuhr NI, Johnen W, Echner G, et al. The ADAM-pelvis phantom-an anthropomorphic, deformable and multimodal phantom for MRgRT. Phys Med Biol. 2019;64(4):04NT05.
Figures
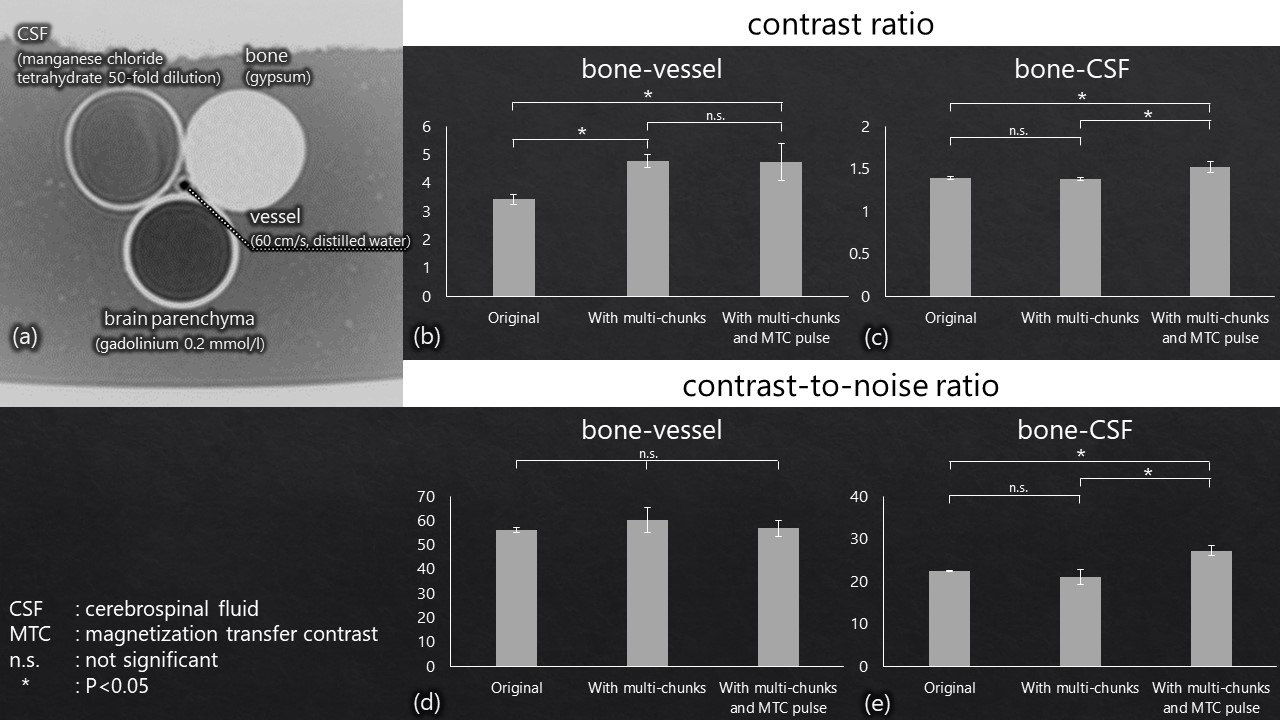
Figure 1: The
original phantom (a)
simulated vessel, bone, brain parenchyma, and cerebrospinal fluid (CSF). Between bone and vessel, the contrast ratio
(CR) using multi-chunks and multi-chunks
combined with MTC pulse are significantly
greater than that of the original parameter (p < 0.05) (b), but no
significant difference was noted in the contrast-to-noise ratio (CNR) among
them (d). Both the CR and CNR between bone and CSF using multi-chunks
combined with MTC pulse are significantly greater than those of using the original parameter and
using multi-chunks (p < 0.05) (c, e).
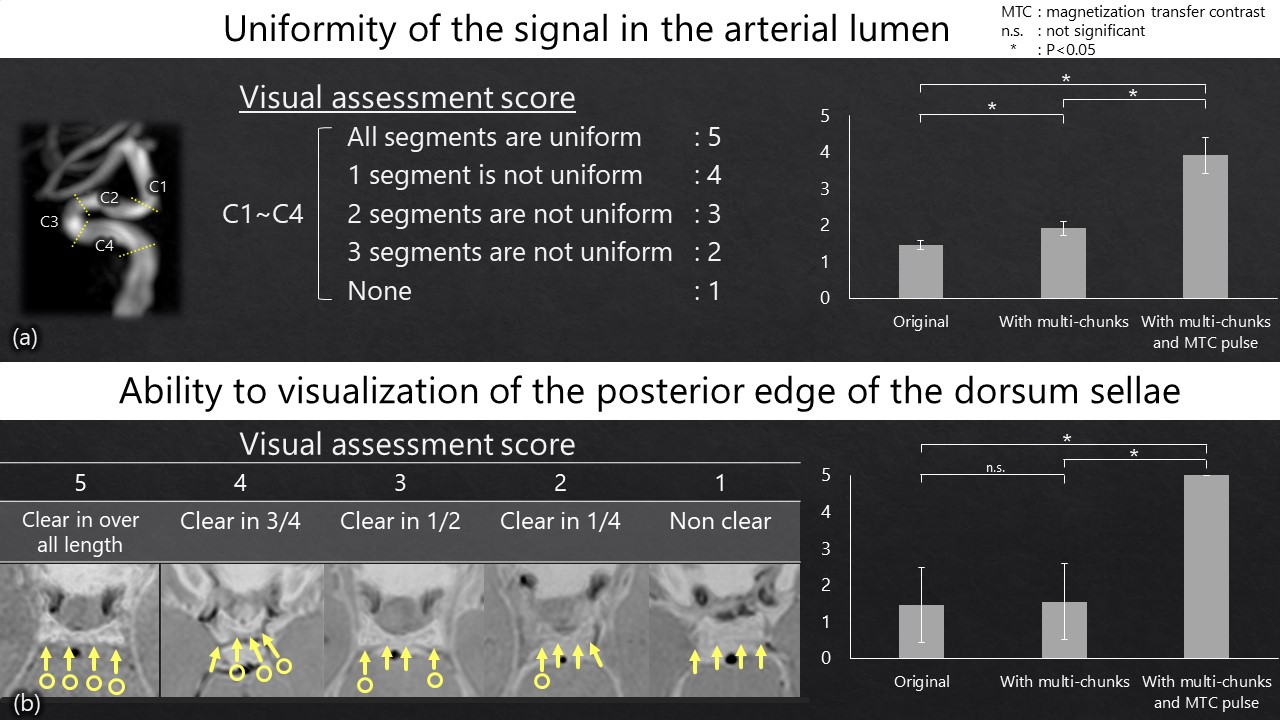
Figure 2: The visual assessment score of signal uniformity of the internal carotid artery
(a)
using multi-chunks
combined with magnetization
transfer contrast (MTC)
pulse is significantly higher than that of using the original parameter and
multi-chunks (p < 0.05). The visual assessment score of the depiction of the posterior margin of the dorsum sellae in contact with the cerebrospinal fluid (b)
using multi-chunks
combined with MTC pulse is significantly higher than that of using the original
parameter and with multi-chunks (p < 0.05).
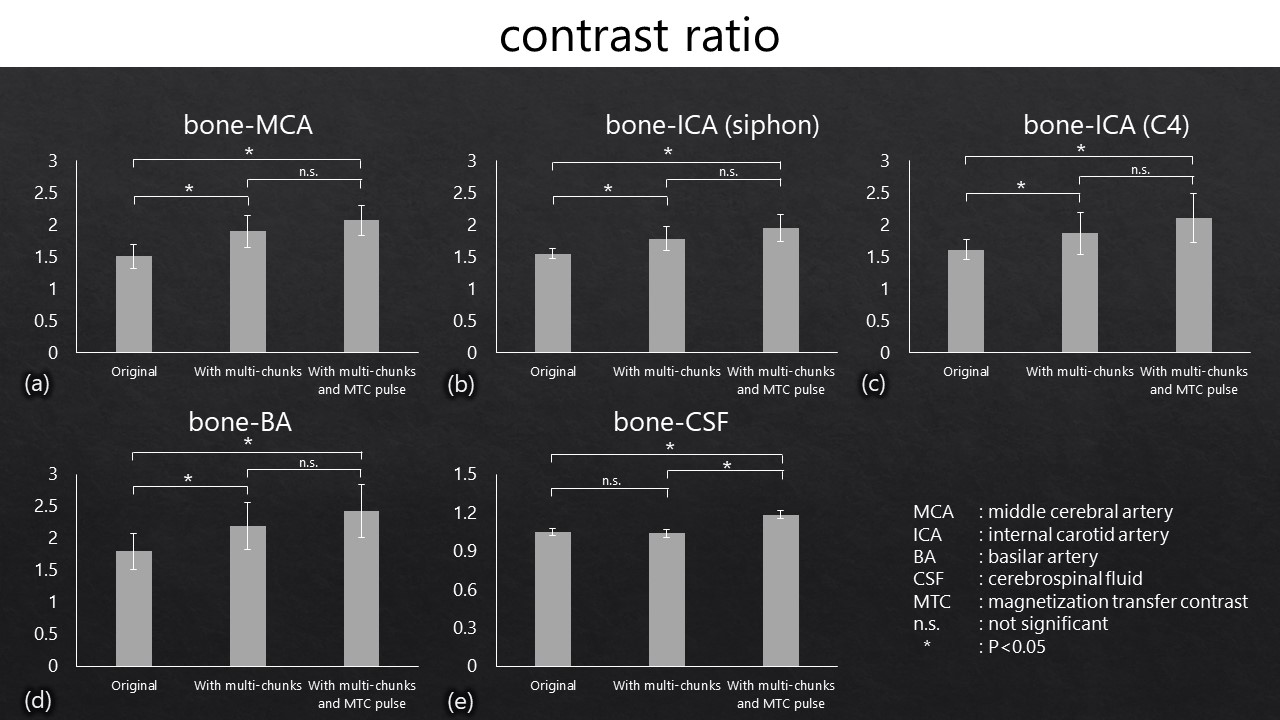
Figure 3: Bar graphs represent the contrast ratio (CR) between
bone and arteries (a-d) and between bone and cerebrospinal fluid (CSF) (e) in original,
multi-chunks, and multi-chunks combined with magnetization transfer contrast (MTC)
pulse. The
CRs between bone and arteries (a-d)
using multi-chunks and with multi-chunks combined with MTC pulse are significantly
greater than that of using the
original parameter (p < 0.05). The CR between bone and CSF (e) using
multi-chunks and MTC pulse is significantly greater than that of using the
original parameter and multi-chunks (p
< 0.05).
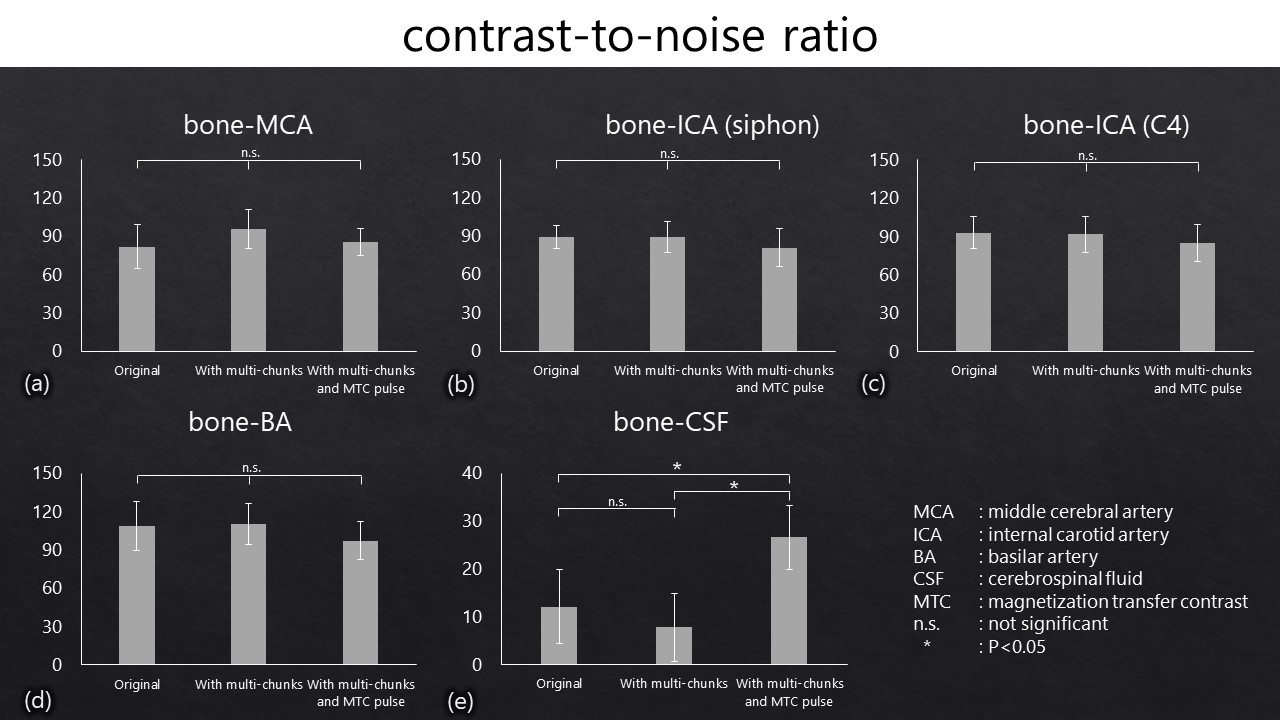
Figure 4: Bar graphs represent the contrast-to-noise
ratio (CNR) between bone and arteries
(a-d) and between bone
and cerebrospinal fluid (CSF)
(e) in the original parameter, multi-chunks and multi-chunks combined with magnetization
transfer contrast (MTC) pulse. Among
the three imaging conditions, no significant difference was noted in the CNR
between bone and arteries (a-d). The CNR between bone and CSF
(e) using multi-chunks combined
with MTC pulse is significantly greater than that of using the original
parameter and multi-chunks (p < 0.05).
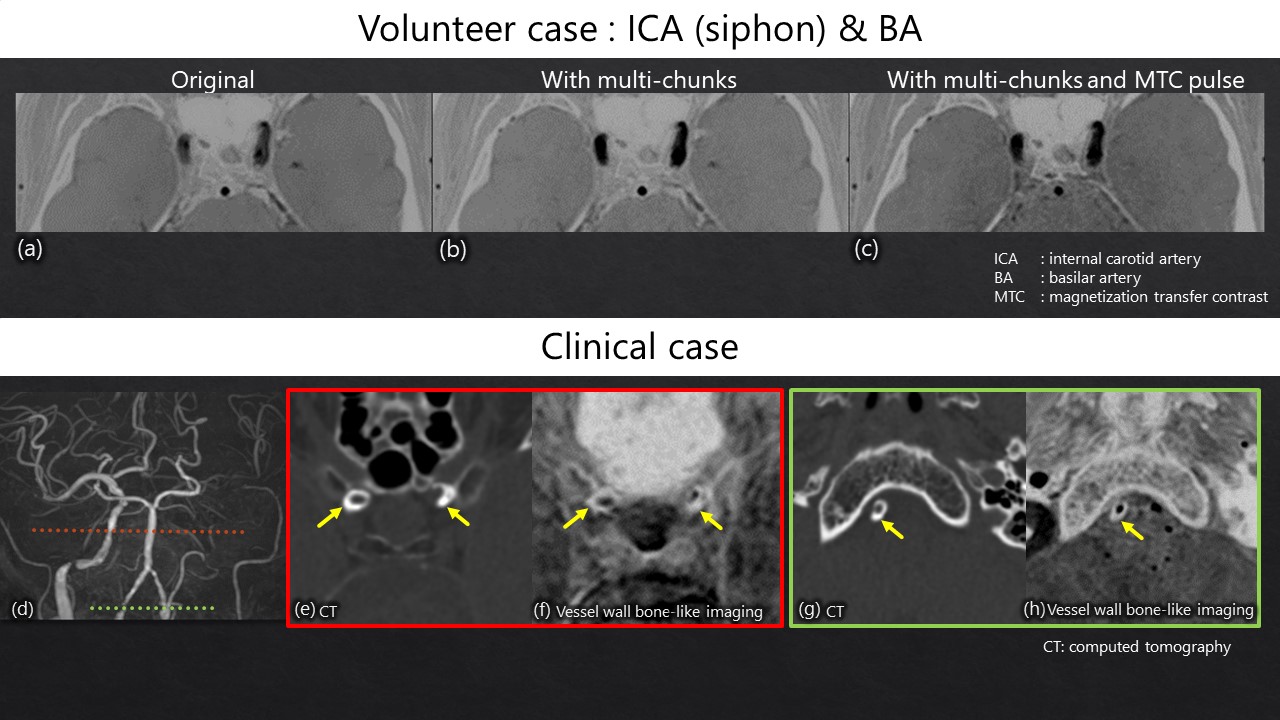
Figure 5: The upper column is one of the volunteer cases
acquired using the
original parameter (a), multi-chunks (b), and multi-chunks combined with MTC pulse (c). Using multi-chunks combined with an
MTC pulse can suppress intra-arterial and CSF flow artifacts, and CSF signal (c). The
lower column is the clinical case. The time-of-flight MR angiography (d) shows
the obstruction of the left ICA. FRACTURE using multi-chunks combined with MTC pulse can good depict
vessel-wall calcifications of bilateral ICA (arrows in e, f) and right
vertebral artery (arrows in g, h) consistent with CT.
DOI: https://doi.org/10.58530/2023/2472