2449
De-streaking effect Deep Learning Reconstruction in free-breathing dynamic contrast enhanced Liver MRI1Department of Radiology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea, Republic of, 2GE Healthcare, Seoul, Korea, Republic of, 3GE Healthcare, Houston, TX, United States, 4GE Healthcare, Boston, MA, United States
Synopsis
Keywords: Liver, Liver
In dynamic contrast enhanced (DCE) liver MRI, fast image acquisition with free breathing comes in expense of artifacts and noise, the most notably streak artifacts. In our study, we evaluated de-streaking effect and image quality of free-breathing stack of star liver MRI acquisition with deep learning reconstruction. Application of deep learning reconstruction (DLR) provides improved image quality by removing streak artifact and noise in liver MR images.Introduction
Dynamic contrast-enhanced (DCE) imaging is crucial in liver MRI for the detection and characterization of hepatic lesion1. However, the acquisition of multiple phases with breath holds is challenging for some patients, especially in old ages and those with a severe medical condition, resulting in motion artifacts causing deterioration of image quality, leading to limitations in interpretation. Differential subsampling with Cartesian ordering (DISCO)-Star is a stack-of-star acquisition method that can be used in the free-breathing acquisition of DCE-MRI, using the Cartesian sampling along the z-axis and concurrent radial sampling along the x,y-plane, resulting in increased spatiotemporal-resolution. However, relative degradation of image quality, caused by noise and streak artifacts from under-sampling of radial sampling is a major drawback of the stack-of-star acquisition method2. The application of deep learning reconstruction (DLR) can improve image quality by reducing streak artifacts and noise, providing better image quality of the DCE-MRI. The purpose of this study was to compare the conventional DISCO-Star DCE-MRI of the liver and corresponding DLR images in view of overall quality and artifacts.Methods
This retrospective study included 27 patients (mean age, 70.7 ± 9.66, 11 men and 16 women) who underwent Liver DCE-MRI with DISCO-star sequences between February 2021 and March 2022. Scans were acquired using a 3T MRI scanner (SIGNA™ Architect, GE Healthcare, Waukesha, USA) with two 30-channel surface coils (AIR™ anterior array coil). The axial DISCO-Star sequence with fat suppression(ASPIR) was acquired continuously obtaining 840 spokes for about 3 minutes 15 seconds after 1 mask-phase with 336 spokes, and for frame rate reconstruction, 6 wash-in phases with 84 spokes per phase and 1 delayed phase with 336 spokes were reconstructed with temporal resolution 19.5 sec. The imaging parameters of DISCO-Star were as follows; Field-of-view = 40cm x 40cm, voxel size = 1.5 x 1.5 x 3.4 mm, flip angle = 12, TE = 1.9 ms, TR=4.0 ms, the number of excitation = 1, acceleration factor = 1.5 x 2, and temporal acceleration for wash-in phases = 4.A deep-learning network was trained from a database of over 10,000 images to reconstruct stack-of-star images with improved signal-to-noise ratio, improved spatial resolution, and reduced streak artifacts. A tunable noise reduction factor was offered to accommodate user preference. The deep-learning network was embedded into the reconstruction pathway to generate two sets of image series (conventional reconstructed and DL reconstructed images) from the same set of raw MR data.
Two radiologists independently reviewed the image with conventional reconstruction (CI) and with deep learning reconstruction (DLRI) for three phases including arterial phase (AP), portovenous phase (PVP), and delayed phase (DP). The images were separately scored with a 5-point Likert scale for overall image quality (5 = highest quality), respiratory or motion artifacts (5 = no artifacts), streak artifacts (5 = minimal artifacts), and liver edge sharpness (5 = no blurring in liver edge).
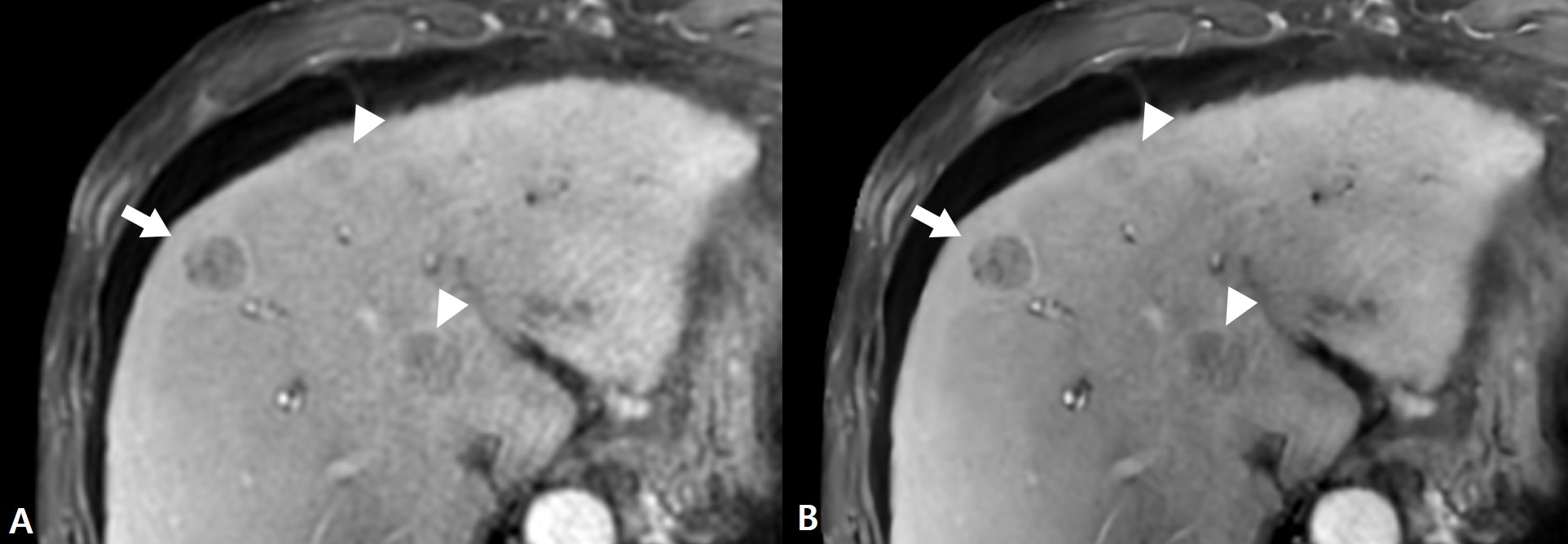
Hepatic lesion conspicuity was analyzed by the same 2 readers. Two radiologists counted and analyzed the hepatic lesions in DP images of DLRI and CI. They independently described the size, and location and scored the level of conspicuity by 5-point scale (5 = definitely distinct).
The mean value of scores was compared with paired Wilcoxon signed-rank test. A P value less than 0.05 were considered significant.
Results
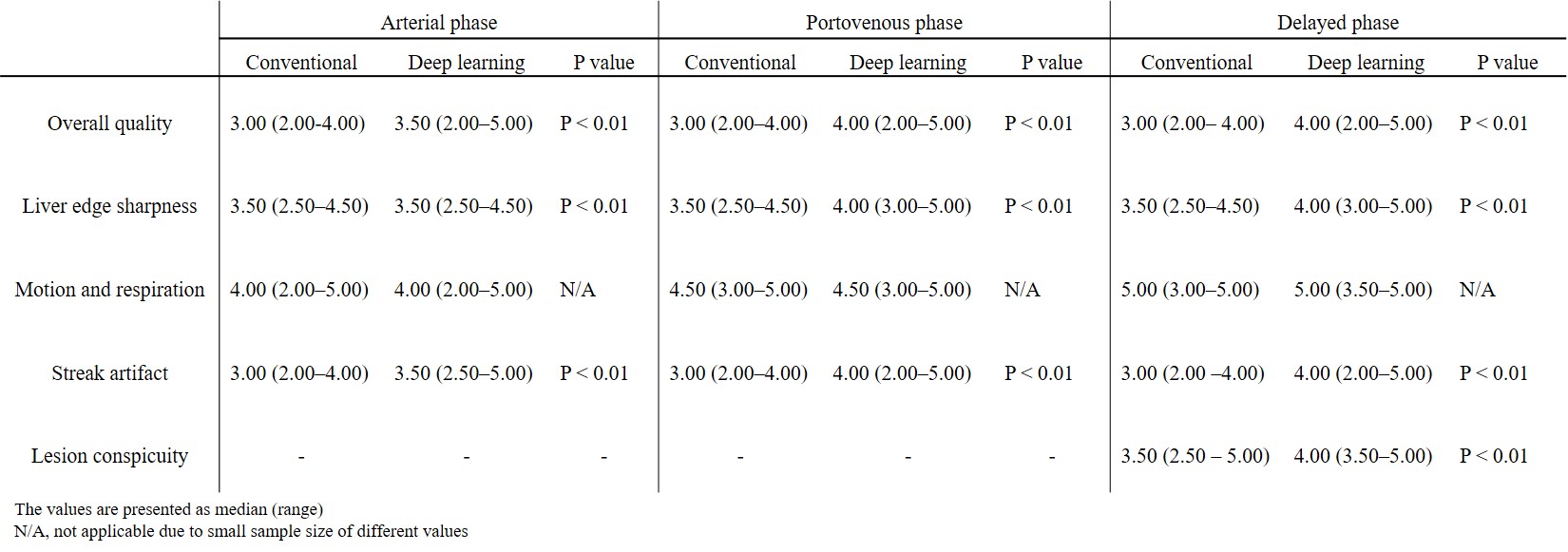
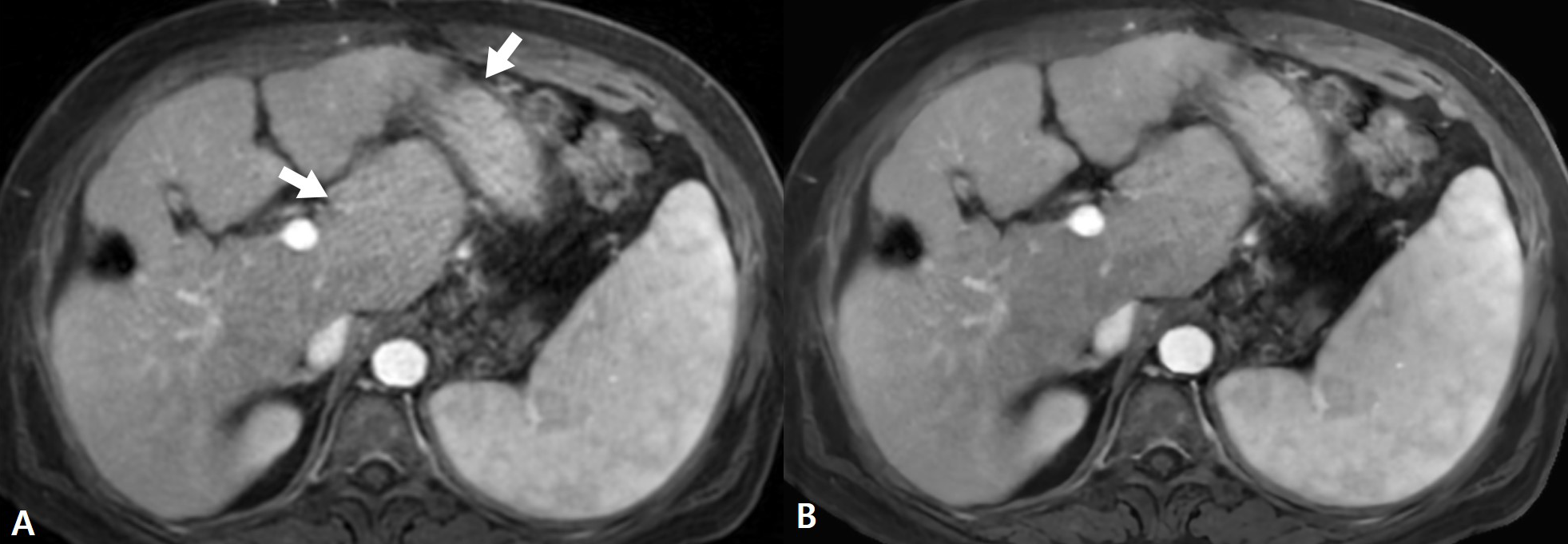
The DLRI showed significantly higher scores compared with CI in all three phases, in terms of overall image quality (median DLRI vs median CI, 3.5 vs 3.0 for AP, 4.0 vs 3.0 for PVP, 4.0 vs 3.0 for DP; P <0.01), liver margin sharpness (3.5 vs 3.5 for AP, 4.0 vs 3.5 for PVP, 4.0 vs 3.5 for DP; P<0.01) and streak artifact (3.5 vs 3.0 for AP, 4.0 vs 3.0 for PVP, 4.0 vs 3.0 for DP; P<0.001). The respiratory or motion artifact showed no significant difference between DLRI and CI in all phases. A total of 41 lesions were evaluated and showed significantly higher scores for lesion conspicuity in DLRI compared to CI (median DLRI vs median CI, 4.0 vs 3.5; P<0.01). The summarized results are presented in figure 1.Discussion
Our study showed that DLR improved overall image quality by efficiently reducing streak artifacts and noise. DLR also improved hepatic lesion conspicuity. The free-breathing DCE-MRI of liver with DISCO-Star and DLR can provide solution for patients with poor breath-hold capacity.Conclusion
Use of DLR for free-breathing DCE-MRI of liver decreased streak artifact and improve image quality and lesion conspicuity of hepatic lesion.Acknowledgements
No acknowledgement found.References
1. Kim SS, Kim SH, Song KD, Choi SY, Heo NH. Value of gadoxetic acid-enhanced MRI and diffusion-weighted imaging in the differentiation of hypervascular hyperplastic nodule from small (<3 cm) hypervascular hepatocellular carcinoma in patients with alcoholic liver cirrhosis: A retrospective case-control study. J Magn Reson Imaging. 2020 Jan;51(1):70-80. https://doi.org/10.1002/jmri.26768.
2. Kaltenbach B, Roman A, Polkowski C, Gruber-Rouh T, Bauer RW, Hammerstingl R, Vogl TJ, Zangos S. Free-breathing dynamic liver examination using a radial 3D T1-weighted gradient echo sequence with moderate undersampling for patients with limited breath-holding capacity. Eur J Radiol. 2017;86:26-32. https://doi.org/10.1016/j.ejrad.2016.11.003.
Figures