2445
Feasibility of Routine Abdominal MR Imaging in Patients at 0.55T: Comparison with 1.5 and 3T1Radiology, University of Michigan, Ann Arbor, MI, United States, 2University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: Liver, Low-Field MRI, Abdomen
Abdominal MRI performed in 51 patients on a commercial 0.55T system were retrospectively and independently rated by two radiologists for diagnostic performance and image quality (IQ). Twenty-eight patients had comparison scans performed at higher field strengths. The clinical question was answered by both radiologists in all 51 cases performed at 0.55T, and the average IQ of all sequences was acceptable. In the subset of patients with comparison studies, the average IQ scores were significantly higher at 0.55T for DWI. No statistically significant difference was seen in IQ for the other sequences. Total acquisition time was almost double at 0.55T.Introduction
There is increasing interest in the MR community in scanners operating at field strengths lower than 1.5T, driven by cost, access, bore size and artifact reduction considerations. However, the lower intrinsic signal-to-noise ratio (SNR) poses a major technical and clinical hurdle1. The utility of recently introduced commercial 0.55T MR scanners for routine clinical imaging is yet to be explored, particularly for abdominal imaging for multiple reasons including breath-hold needs, susceptibility differences between tissues, physiological motion, and the need for large fields of view at high resolution 2,3 . Following initial work done to optimize the abdominal sequences in healthy volunteers, we initiated use of a 0.55T clinical scanner for routine abdominal MRI indications. The purpose of this study is to determine the feasibility of routine abdominal imaging on a commercial 0.55 T MRI system (MAGNETOM Free.Max, Siemens Healthineers) by assessing ability of the radiologist to answer the clinical question based on 0.55T images, evaluating the image quality of all sequences collected at 0.55T, and comparing the image quality to those of images acquired at higher field strengths in the subset of patients who had comparison imaging.Materials and Methods
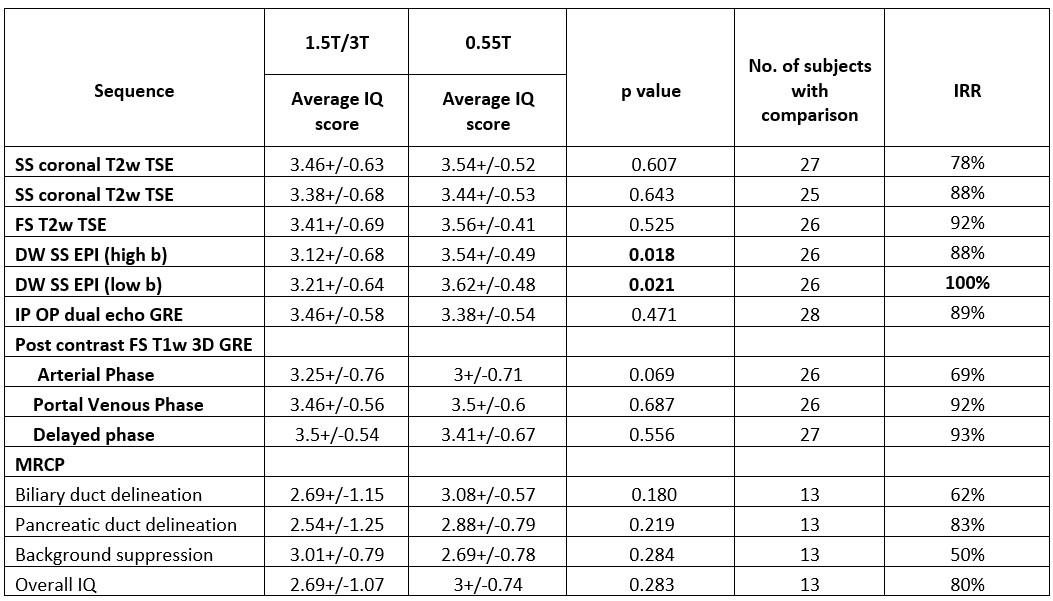
In this IRB approved study, a retrospective review of 51 routine abdominal MRI studies performed at 0.55T between Nov 2021 and Sep 2022 was conducted. The indications were to evaluate liver, renal, biliary, and pancreatic pathologies. The routine abdominal MRI protocol included the following sequences: Single Shot (SS) coronal and axial T2w TSE, fat Saturated (FS) T2w TSE, DW SS-EPI, IP-OP dual-echo GRE, pre and multiphase (arterial, venous, delayed) post contrast FS T1w 3D GRE. 3D MRCP was performed when indicated clinically. The ability to answer the clinical question (yes/no) on 0.55T was documented. Images were rated independently by two abdominal radiologists with 17 and 13 yrs of experience. The overall image quality (IQ) of all sequences was rated on a scale of 1-4 (1: extremely poor, 2: poor, 3: good, 4: excellent) and the presence and type of artifacts documented. MRCP images were rated for IQ and delineation of biliary and pancreatic ducts. In the 28 patients who had comparison MRI studies at 1.5T (n=21) and 3T (n=7), the images were evaluated similarly. IQ rating of ≥3 was considered acceptable. Wilcoxon signed rank test was used to test for significant difference between the paired ratings. Interrater reliability (IRR) was assessed using percentage of times both readers provided concordant results for the same sequence.Results
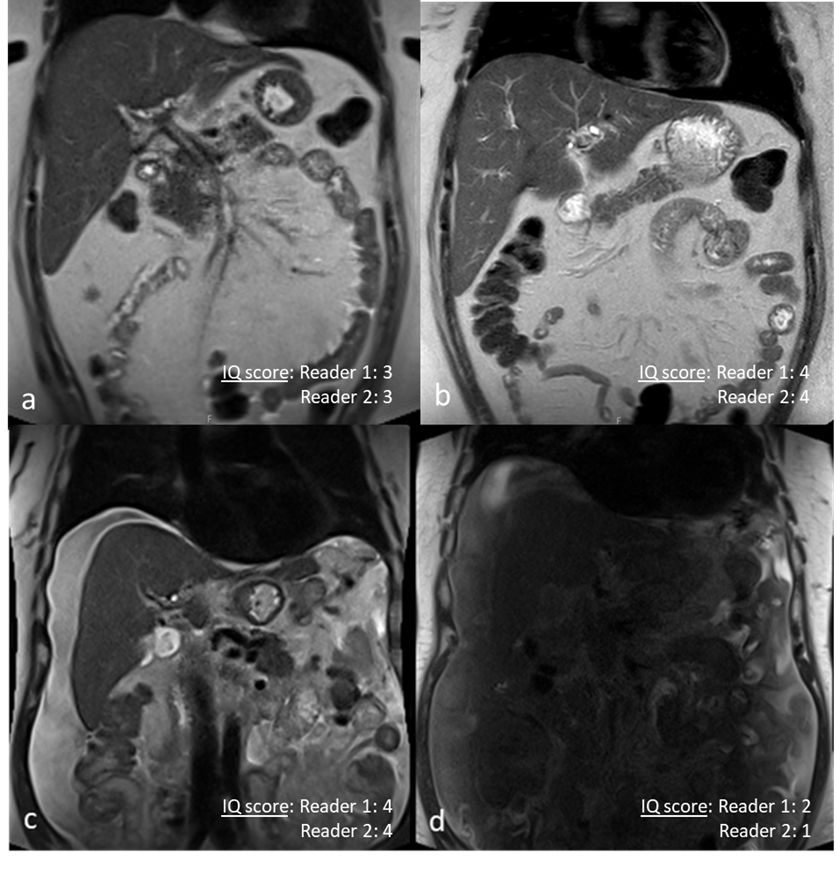
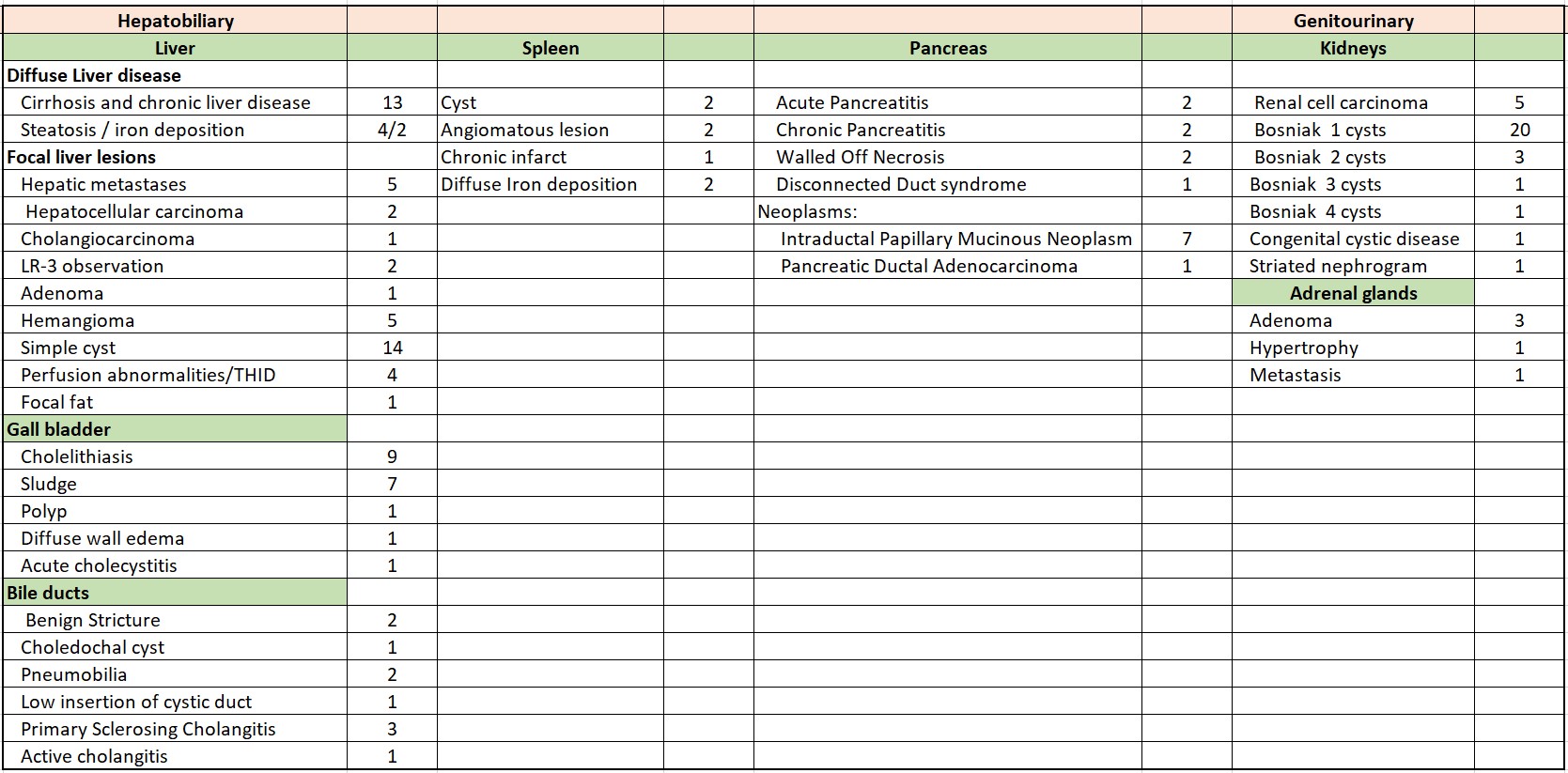
The clinical question was answered by both radiologists in all 51 cases. The questions were characterization of mass(es) in liver(n=20), pancreas(n=8) and kidneys(n=5), portal vein thrombosis(n=2), pancreatitis(n=3), post treatment surveillance of renal mass(n=2), choledocholithiasis(n=11), and cholangitis(n=3). Summary of findings is shown in Figure 1. Acceptable (≥3) average overall IQ ratings were assigned to all sequences obtained at 0.55T (Figure 2). In the subset with comparison studies at higher field strengths (n=28), the average study acquisition time was 54±10 min vs. 36 ± 11 min at higher field strengths. In this subset, statistically significant higher average IQ ratings were assigned to high and low b value DWI images at 0.55T (Figure 3). Higher ratings were assigned at 0.55T to SS coronal and axial T2w TSE, FS T2w TSE, and post contrast venous phase (none statistically significant); Lower ratings at 0.55T were assigned to IP-OP dual-echo GRE, post contrast arterial and delayed phases (none statistically significant). 3D MRCP had higher average ratings at 0.55T for overall IQ and delineation of biliary and pancreatic ducts, although ratings for background suppression were lower. Common artifacts at 0.55T were residual aliasing and central noise enhancement related to parallel imaging (n= 48), respiratory motion (n=43) and signal loss in left hepatic lobe on DWI (n=45). Susceptibility artifacts (n=6) were like those at higher field strengths.Discussion
Our results confirm feasibility of routine abdominal imaging on a commercial 0.55T MRI system. The clinical question was answered in all the 51 cases and the average image quality of all sequences were rated acceptable. Lower overall IQ ratings of some of the sequences performed on 0.55T compared to those acquired at higher field strengths were due to lower SNR, often necessitating an increase in scan time to gain back some signal and increase spatial resolution. Parallel imaging artifacts at 0.55T were likely exacerbated by the lower SNR, and respiratory motion artifacts due to longer breath holds. The latter issue applies specially to contrast-enhanced sequences where Dixon methods are used rather than fat suppression pulses. Despite lower SNR and artifacts, diagnostic capability was maintained at 0.55T. Of interest, higher overall IQ ratings were assigned to high and low b value DWI images and 3D MRCP on 0.55T and EPI related distortions were much less pronounced at 0.55T. Higher MRCP ratings related to better visualization of second and higher order intrahepatic ducts. Patients with large abdominal girth and large volume ascites received higher rating at 0.55T on SS coronal and axial and FS T2w TSE, due to less signal drop from standing wave effects. While these differences were systematic, they did not reach statistical significance.Conclusion
Diagnostic quality abdominal scans can be obtained at 0.55T with longer acquisition times than at higher field strengths.Acknowledgements
Research Grant Support from Siemens HealthineersReferences
1. Smith HJ. The history of magnetic resonance imaging and its reflections in Acta Radiologica. Acta Radiol. 2021 Nov;62(11):1481–98.
2. Chandarana H, Bagga B, Huang C, Dane B, Petrocelli R, Bruno M, et al. Diagnostic abdominal MR imaging on a prototype low-field 0.55 T scanner operating at two different gradient strengths. Abdom Radiol N Y. 2021 Dec;46(12):5772–80.
3. Campbell-Washburn AE, Ramasawmy R, Restivo MC, Bhattacharya I, Basar B, Herzka DA, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology. 2019 Nov;293(2):384–93.
Figures
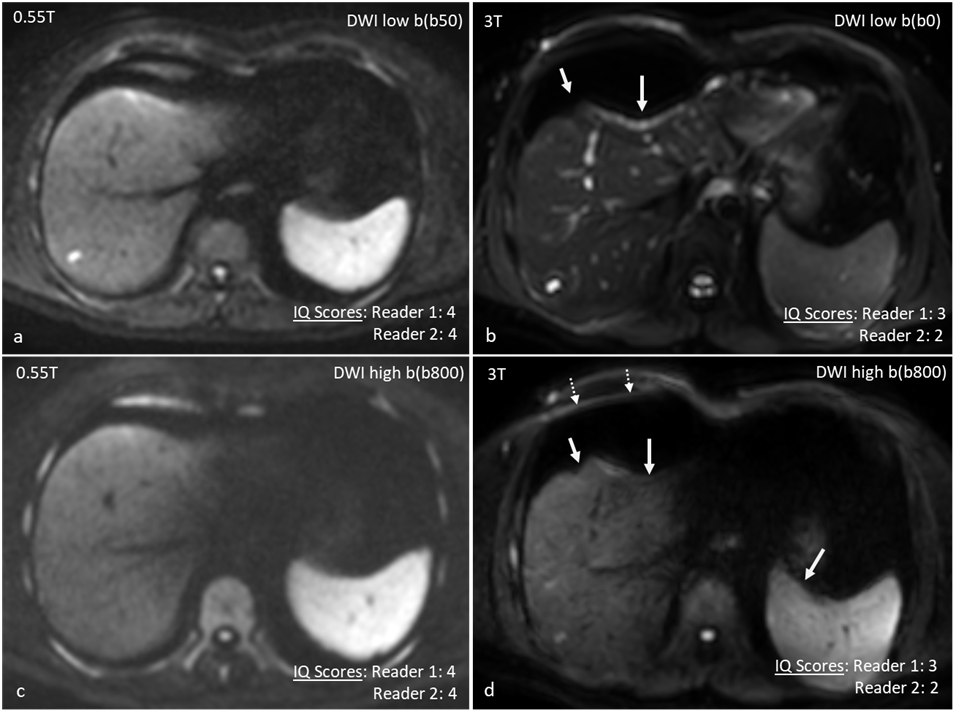
Representative images of DWI (high and low b values) that were rated higher at 0.55T. In comparison to 0.55T (a and c), images at 3T (b and d) had prominent anatomic distortion (solid arrows) and residual aliasing (dotted arrows). DWI was assigned lower scores at 3T by both readers.
DWI parameters at 0.55T: TR/TE= 6000/73 ms, slice thickness= 6mm, FA: 900, ETL:46
DWI parameters at 3T: TR/TE= 1704/68.8 ms, slice thickness= 6mm, FA: 900, ETL: 85