2434
Preoperative gadoxetic acid-enhanced MRI combined with MVI can effectively predicte early recurrence in hepatocellular carcinoma1Affiliated Nantong Hospital 3 of Nantong University, Nantong, Jiangsu Province, China, 2Philips Healthcare, Shanghai, China
Synopsis
Keywords: Liver, Tumor, early recurrence
Synopsis: The purpose of this study is to determine whether preoperative gadoxetic acid-enhanced MRI combined with microvascular invasion can effectively improve the predictive efficacy of early recurrence in HCC. We retrospectively reviewed patients with HBV who underwent curative resection for HCC, analysed preoperative factors to develop a preoperative model, and analysed both preoperative factors and microvascular invasion to develop a pre-/postoperative prediction model. Our study showed that the preoperative and pre-/postoperative prediction models demonstrate good performance for predicting early recurrence, the AUC of the two prediction model better than only the MVI risk factor.
Introduction
Hepatic resection is one of the most important treatment methods for hepatocellular carcinoma patients, unfortunately patients with HCC undergoing partial hepatectomy also have considerable recurrence rates 1. Almost 80% of recurrent tumours have intrahepatic recurrence within 2 years, which defined as early recurrence for HCC after partial hepatectomy2-4. Therefore, it is necessary to understand and predict the risk of postoperative tumour recurrence to guide further surveillance and treatment. Microvascular invasion, is an expression of aggressive biological behavior by the tumor and is currently one of the most critical factors predictive of HCC recurrence 5. However HCC without MVI still has early recurrence after hepatectomy, therefore we hypothesized whether preoperative gadoxetic acid-enhanced MRI combined with MVI can effectively improve the predictive efficacy of early recurrence in HCC after curative resection. The purpose of this study was to investigate the value of preoperative MRI combined with MVI in predicting early recurrence after hepatectomy.Methods
This is a retrospective two-center study, patients underwent surgery for HCC with preoperative gadoxetate disodium (EOB)-enhanced MR were enrolled, to training and testing sets. Multivariate Cox regression analyses of preoperative and postoperative high risk predictors of early recurrence were performed. Preoperative and pre-/postoperative prediction models were constructed. In the training sets and testing sets, using the time-dependent receiver operating characteristic(ROC) curves to evaluate the discrimination of the two prediction models, area under curves (AUC) were calculated. The diagnostic performance of each risk features (NHHN, non-smooth tumour margin, peritumoural hypointensity on HBP, MVI) and combine features were also calculated.Results
1. Three MRI features were independently associated with early recurrence: nonhypervascular hepatobiliary phase(HBP) hypointense nodule (NHHN) (Hazard Ratio(HR) =3.700), non-smooth tumour margin (HR=2.781), and hepatobiliary phase (HBP) peritumoural hypointensity (HR=2.614). After adding MVI, MVI and one MRI features were independently associated with early recurrence: MVI (HR=3.885), NHHN (HR=4.320). Fig 1.2. In the training sets, AUCs for the two models were 0.821 (preoperative prediction models), 0.890 (pre-/postoperative prediction models). In the testing sets, AUCs for the two models were 0.748 (preoperative prediction models), 0.794 (pre-/postoperative prediction models).Table 1.
3. The diagnostic performance of each risk factor and combine factors were all lower than the two prediction models. Table 1.
Conclusions
In this two-center study, the preoperative and pre-/postoperative prediction models demonstrate good performance for predicting early recurrence, the AUC of the two prediction model better than only the MVI risk factor. In the preoperative prediction model, NHHN, non-smooth tumour margin, and HBP peritumoural hypointensity can be used preoperatively to estimate the risk of early recurrence after resection of a single HCC. Such models might be useful to guide treatment strategies and enable a step forward for precise medicine.Discussion
The prediction model using preoperative MRI features, including NHHN, non-smooth tumour margin, and peritumoural hypointensity on HBP could estimate early recurrence after resection of a single HCC. The predictive efficacy was good. Consistent with previous studies 5,6,8-13 we showed that MVI was significantly correlated with early recurrence. But in fact MVI can only be confirmed by postoperative pathology, so we can't use the presence of MVI to select a treatment before surgery. Also we used only MVI to predict early recurrence, the AUC was lower than the two predication models. NHHNs may represent borderline hepatocellular nodules including high-grade dysplastic nodules or early HCC 11-12. Toyoda et al 7, 13suggested that the presence of NHHN may indicate enhanced hepatocarcinogenesis even when the nodule itself does not progress to HCC, and may be more likely in patients with more severe liver fibrosis. Our findings support the hypothesis that recurrence is more likely to be caused by multicentric tumours or de novo cancer formation from underlying liver hepatitis and cirrhosis 1,3,14-15. To date, there is no report on the association between viral load and NHHN, although overexpression of hepatitis B spliced protein in HCC cells reportedly increases cell invasion and motility 16. HBV positivity may be an important factor associated with NHHNs, particularly in patients with hepatitis B virus-positive chronic hepatitis cirrhosis. Non-smooth tumour margin and peritumoural hypointensity on HBP were also independent risk factors for early recurrence,the same as previous studies17-18.This study showed that preoperative gadoxetic acid-enhanced MRI combined with MVI can effectively improve the predictive efficacy of early recurrence in HCC after hepatectomy. Our results suggest that a prediction model using preoperative MR imaging features may identify high-risk patients, for whom alternative treatment options may be considered, such as liver transplantation or more extensive resection.
Acknowledgements
No acknowledgement found.References
1. Poon RT, Fan ST, Lo CM, et al.Long-term survival and pattern of recurrence after resection of small hepatocellular carcinoma in patients with preserved liver function: implications for a strategy of salvage transplantation. Ann Surg. 235(3)(2002) :373-382.
2. Imamura H, Matsuyama Y, Tanaka E, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol.38(2)(2003):200-207.
3. Portolani N, Coniglio A, Ghidoni S, et al.Early and late recurrence after liver resection for hepatocellular carcinoma: prognostic and therapeutic implications. Ann Surg. 243(2) (2006) : 229-235.
4. Jung SM, Kim JM, Choi GS, et al. Characteristics of Early Recurrence After Curative Liver Resection for Solitary Hepatocellular Carcinoma. J Gastrointest Surg. 23(2)(2019) :304-311.
5. Rodríguez-Perálvarez M, Luong TV, Andreana L, Meyer T, Dhillon AP, Burroughs AK. A systematic review of microvascular invasion in hepatocellular carcinoma: diagnostic and prognostic variability. Ann Surg Oncol. 2013;20(1):325-339. doi:10.1245/s10434-012-2513-1.
6. Lee S, Kang TW, Song KD, et al. Effect of Microvascular Invasion Risk on Early Recurrence of Hepatocellular Carcinoma After Surgery and Radiofrequency Ablation. Ann Surg. 2021;273(3):564-571. doi:10.1097/SLA.0000000000003268.
7. Toyoda H, Tada T, Yasuda S, et al. The emergence of non-hypervascular hypointense nodules on Gd-EOB-DTPA-enhanced MRI in patients with chronic hepatitis C. Aliment Pharmacol Ther. 2019;50(11-12):1232-1238. doi:10.1111/apt.15490.
8. Wang X, Zhang Z, Zhou X, et al. Computational quantitative measures of Gd-EOB-DTPA enhanced MRI hepatobiliary phase images can predict microvascular invasion of small HCC. Eur J Radiol. (2020) 133:109361.
9. Ahn SJ, Kim JH, Park SJ, et al. Hepatocellular carcinoma: preoperative gadoxetic acid-enhanced MR imaging can predict early recurrence after curative resection using image features and texture analysis. Abdom Radiol (NY) .44(2)(2019) :539-548.
10. Lee DH, Lee JM, Kang TW, et al. Clinical Outcomes of Radiofrequency Ablation for Early Hypovascular HCC: A Multicenter Retrospective Study. Radiology 286(1)(2018):338-349.
11. Hwang J, Kim YK, Jeong WK, et al. Nonhypervascular Hypointense Nodules at Gadoxetic Acid-enhanced MR Imaging in Chronic Liver Disease: Diffusion-weighted Imaging for Characterization. Radiology.276(1)(2015):137-146.
12. Lee DH, Lee JM, Yu MH, et al. Non-hypervascular hepatobiliary phase hypointense nodules on gadoxetic acid-enhanced MR can help determine the treatment method for HCC. Eur Radiol. 29(6) (2019):3122-3131.
13. Toyoda H, Kumada T, Tada T, et al. Non-hypervascular hypointense nodules on Gd-EOB-DTPA-enhanced MRI as a predictor of outcomes for early-stage HCC. Hepatol Int. 9(1)(2105) :84-92.
14. Cheng Z, Yang P, Qu S, et al. Risk factors and management for early and late intrahepatic recurrence of solitary hepatocellular carcinoma after curative resection. HPB (Oxford). 17(5)(2015): 422-427.
15. Xu XF, Xing H, Han J, et al. Risk Factors, Patterns, and Outcomes of Late Recurrence After Liver Resection for Hepatocellular Carcinoma: A Multicenter Study From China. JAMA Surg.154(3)(2019) :209-217.
16. Chen WN, Chen JY, Jiao BY, et al. Interaction of the hepatitis B spliced protein with cathepsin B promotes hepatoma cell migration and invasion. J Virol. 86(24)(2012) :13533-13541.
17. Raffetti E, Fattovich G, Donato F. Incidence of hepatocellular carcinoma in untreated subjects with chronic hepatitis B: a systematic review and meta-analysis. Liver Int.36(9)(2016) :1239-1251.
18. Choi SY, Kim SH, Park CK, et al. Imaging Features of Gadoxetic Acid-enhanced and Diffusion-weighted MR Imaging for Identifying Cytokeratin 19-positive Hepatocellular Carcinoma: A Retrospective Observational Study. Radiology.286(3) (2018):897-908.
Figures
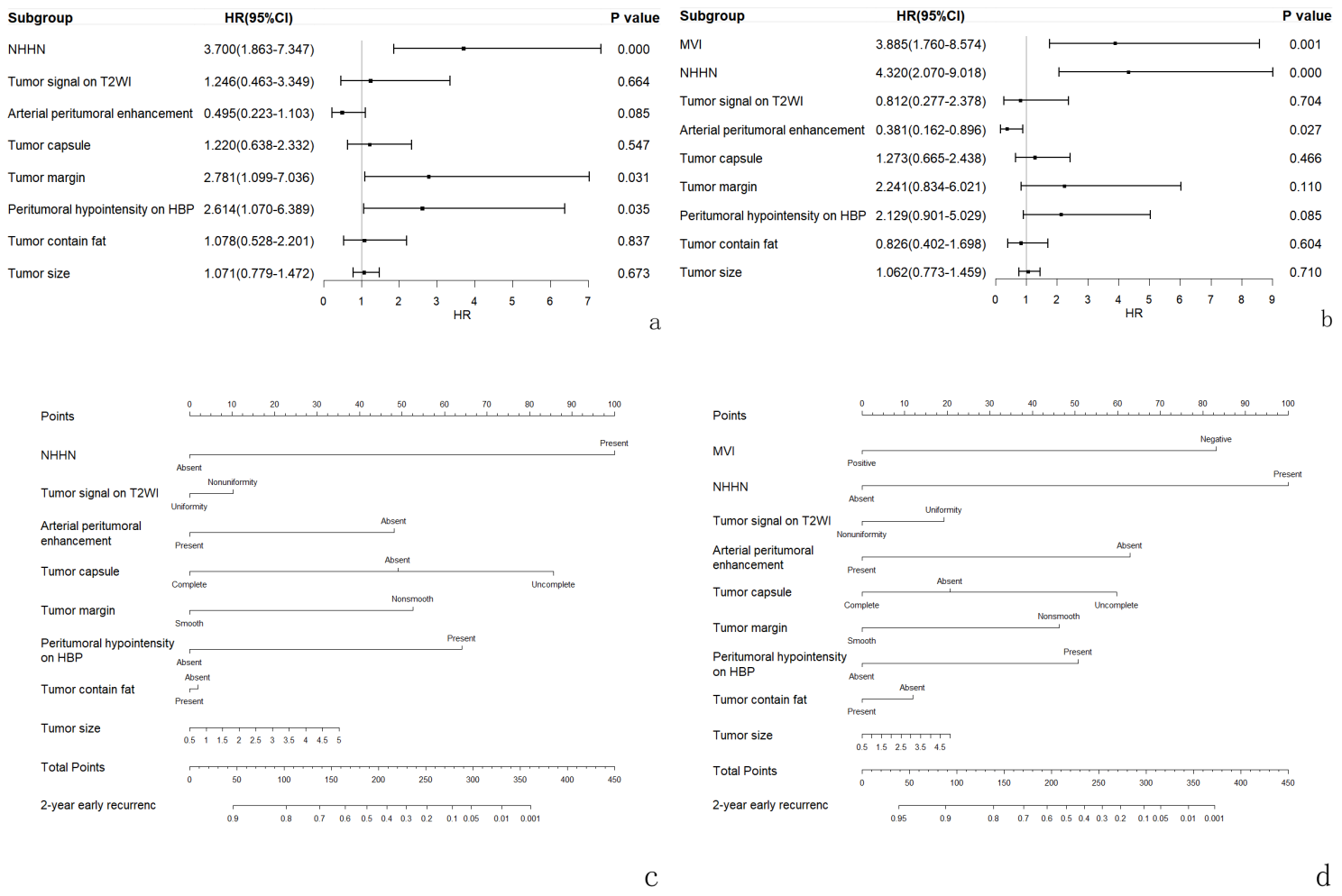
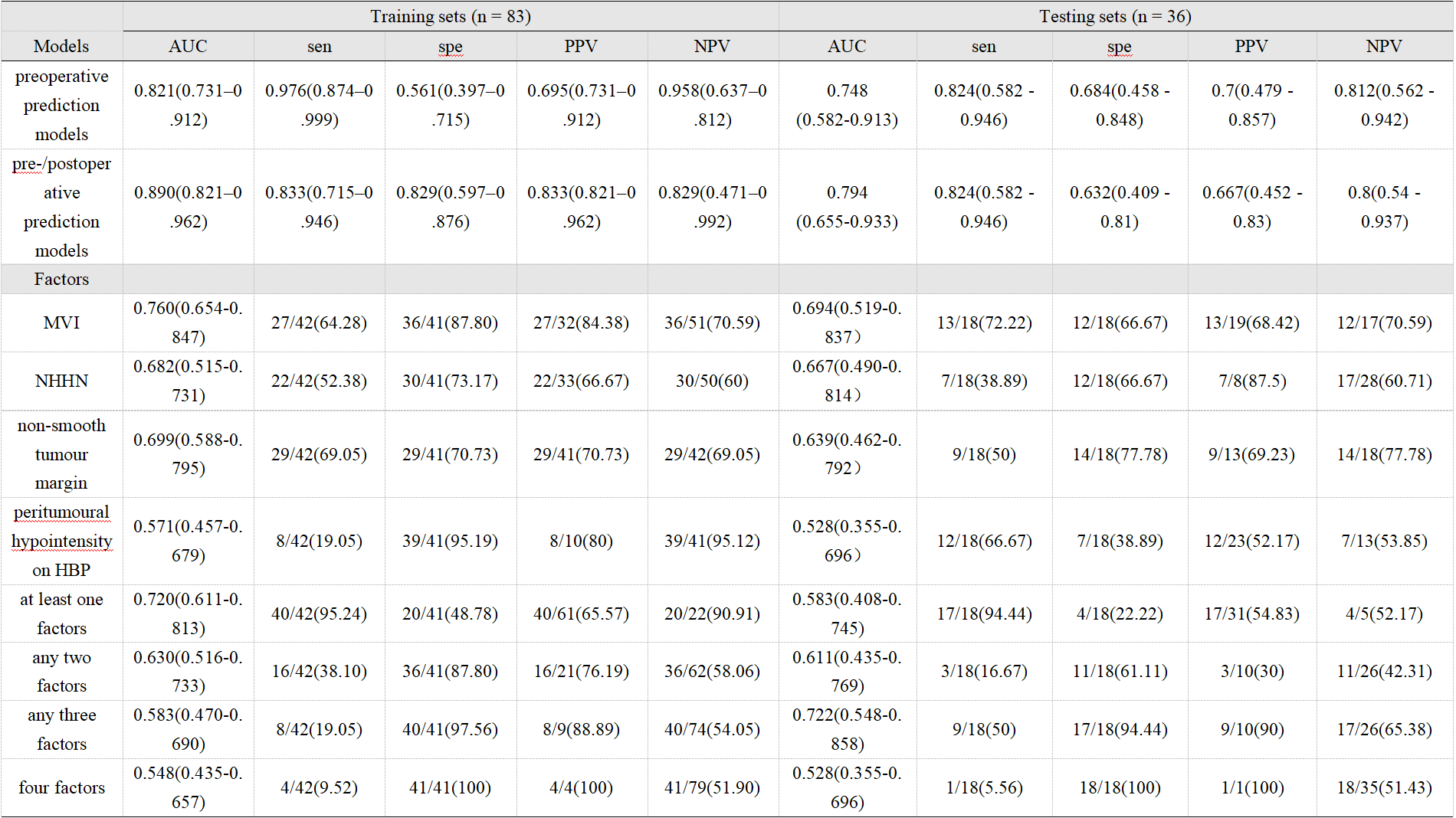
Table 1: The performance of the preoperative, pre-/postoperative prediction model, each risk factors and combine factors for predicting early recurrence
AUC=area under the curve; CI=confidence interval; HBP=hepatobiliary phase; MVI=microvascular invasion; NHHN=nonhypervascular hepatobiliary phase hypointense nodule; NPV=Negative Predictive Value; PPV=PositivePredictive Value; Sen=sensitivity; Spe=specificity;