2333
High-resolution fetal brain anatomical imaging using a reduced field-of-view with outer volume suppression1Department of Radiology, Weill Cornell Medicine, New York, NY, United States, 2Department of Biomedical Engineering, Ulsan National Institute of Science and Techonology, Ulsan, Korea, Republic of
Synopsis
Keywords: Fetal, Fetus
Reliable fetal brain anatomical imaging is critical to identify structural brain abnormalities early in utero. Fetal brain imaging with increased spatial resolution may provide more details but is limited by a large acquisition matrix size with a long readout time. Here, we demonstrate high-resolution fetal brain imaging using a reduced field-of-view with outer volume suppression. The performance of outer volume suppression pulse was evaluated in simulations and phantom/in vivo experiments. High-resolution imaging with reduced field-of-view demonstrated improved image quality than conventional imaging without visible blurring or aliasing artifacts.Introduction
Acquisition of reliable anatomical images of the fetal brain is important for assessing brain development and identifying brain abnormalities in fetuses.1 The most widely used sequence for fetal brain anatomical imaging is single-shot fast spin-echo (SSFSE) because this provides a short scan time (~1 sec) to freeze fetal motion in each slice.2,3 In general, because the fetus is surrounded by maternal tissue, a wide field-of-view (FOV) covering the entire maternal abdomen is required in fetal MRI to avoid aliasing artifacts. As a result, high-resolution imaging of the fetal brain is limited by a large acquisition matrix size, which increases sensitivity to fetal motion and T2 decay in SSFSE imaging. In this study, we demonstrate the feasibility of high-resolution anatomical imaging of the fetal brain using SSFSE combined with outer volume suppression (OVS) preparation to reduce the FOV and hence reduce the matrix size.Methods
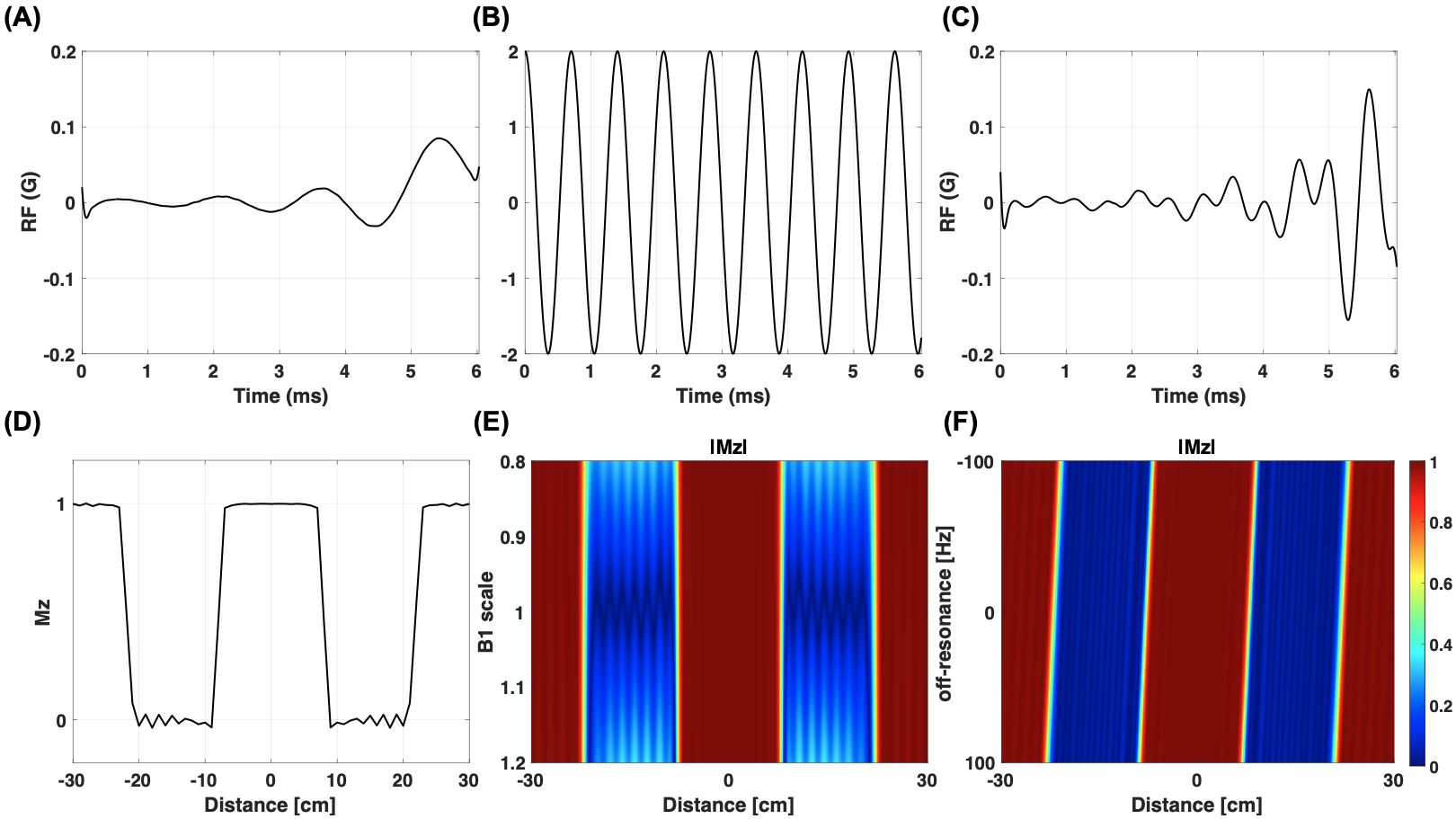
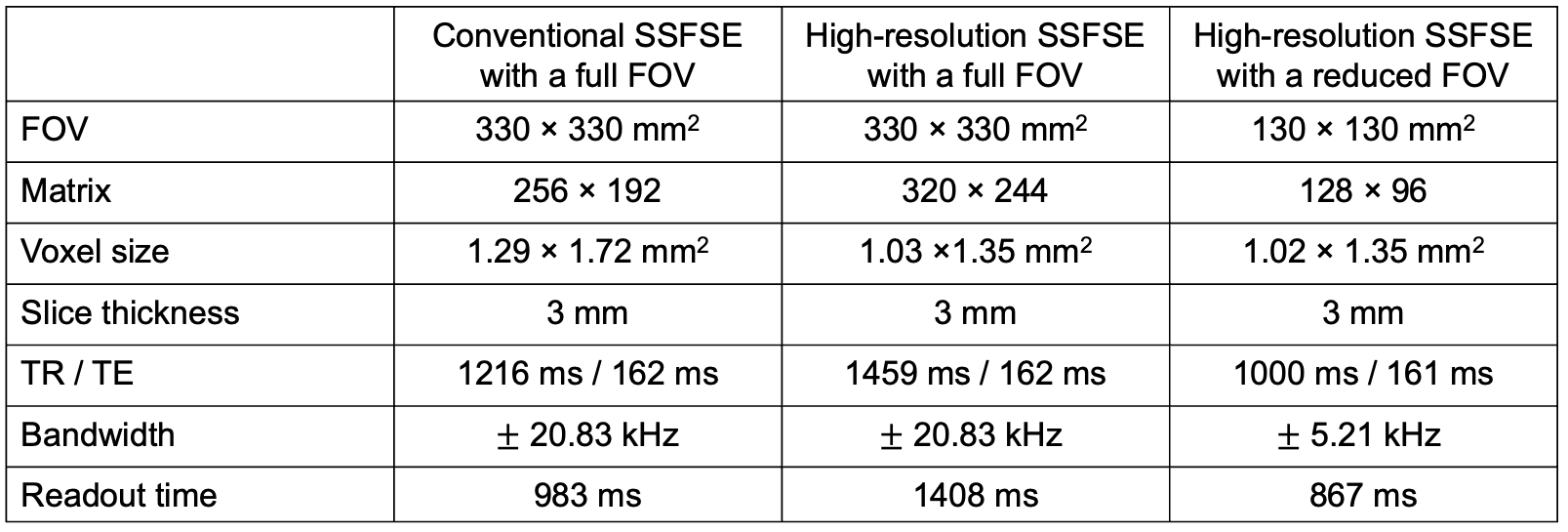
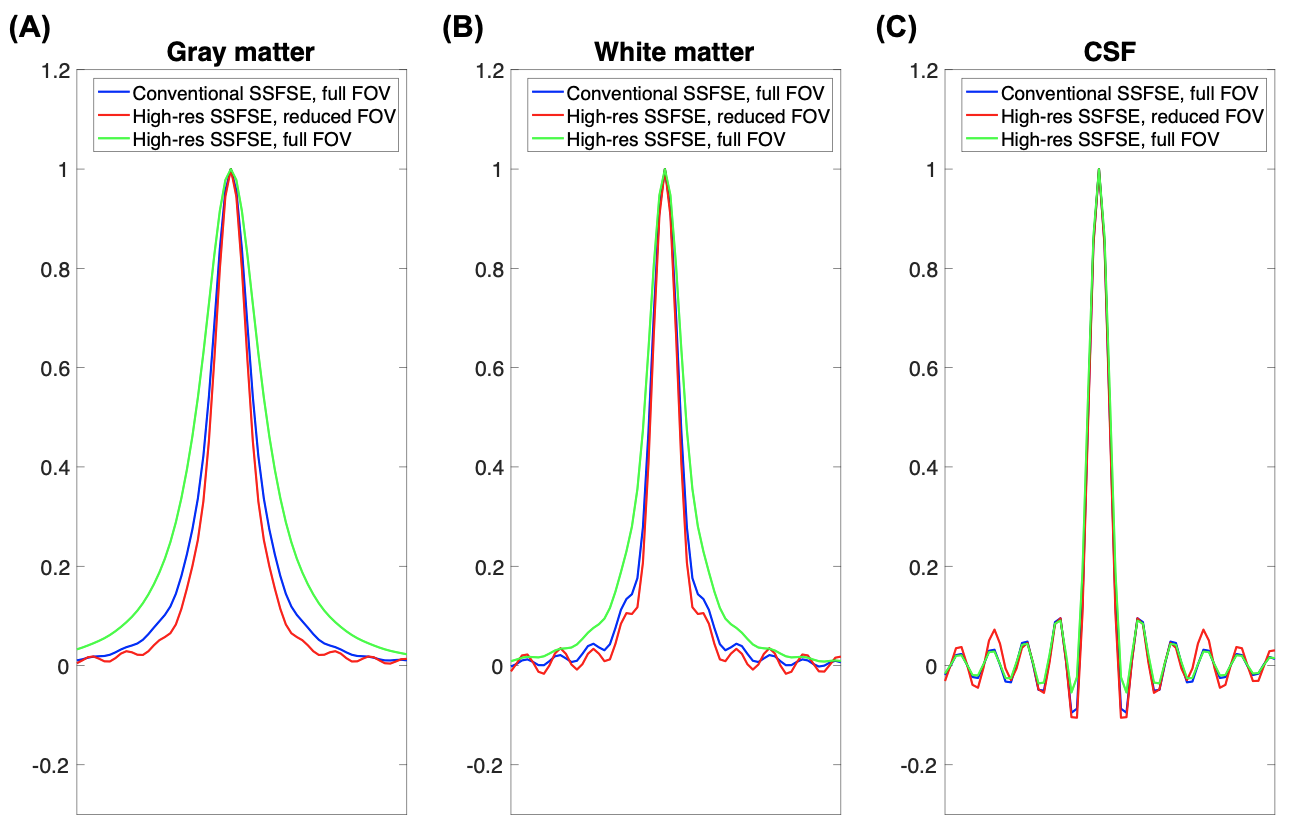
An RF pulse for single-slab saturation was designed using the Shinnar-Le Roux minimum-phase RF approach4 with a time-bandwidth product of 8. OVS preparation pulse was generated by modulating this RF with a cosine waveform to suppress both sides of the outer volume simultaneously (Fig. 1A-C).5 Excitation profile of OVS pulse and its sensitivity to B1 and B0 variations were simulated. B1 scale ranging from 0.8 to 1.2 and off-resonance ranging from -100 to 100 Hz were used. In our imaging sequence, the designed OVS RF pulse followed by a gradient crusher (total duration of 8 ms) was repeated three times immediately prior to SSFSE readout in order to reduce residual Mz in the saturation bands due to B1 and B0 inhomogeneity. Signal suppression using repeated OVS pulses was evaluated in a phantom scan. In the in vivo experiments, we compared three different approaches to fetal brain anatomical imaging in a pregnant woman (gestational age, 32 weeks): (1) conventional SSFSE with a full FOV, (2) high-resolution SSFSE with a full FOV, and (3) high-resolution SSFSE with a reduced FOV (proposed). Imaging parameters are summarized in Table 1. The passband and saturation slabs of the proposed method were 10 cm and 20 cm, respectively. Fat pre-saturation was used in all three methods and was performed immediately before OVS preparation in the proposed method. The point spread functions of these three imaging sequences were calculated for white matter, gray matter, and cerebrospinal fluid (CSF) by mapping simulated transverse signal of SSFSE to k-space, zero-padding for three times higher resolution, and applying Fourier transform. All experiments were performed on a clinical 1.5T scanner (GE Signa HDx) using an 8-channel cardiac array coil.Results
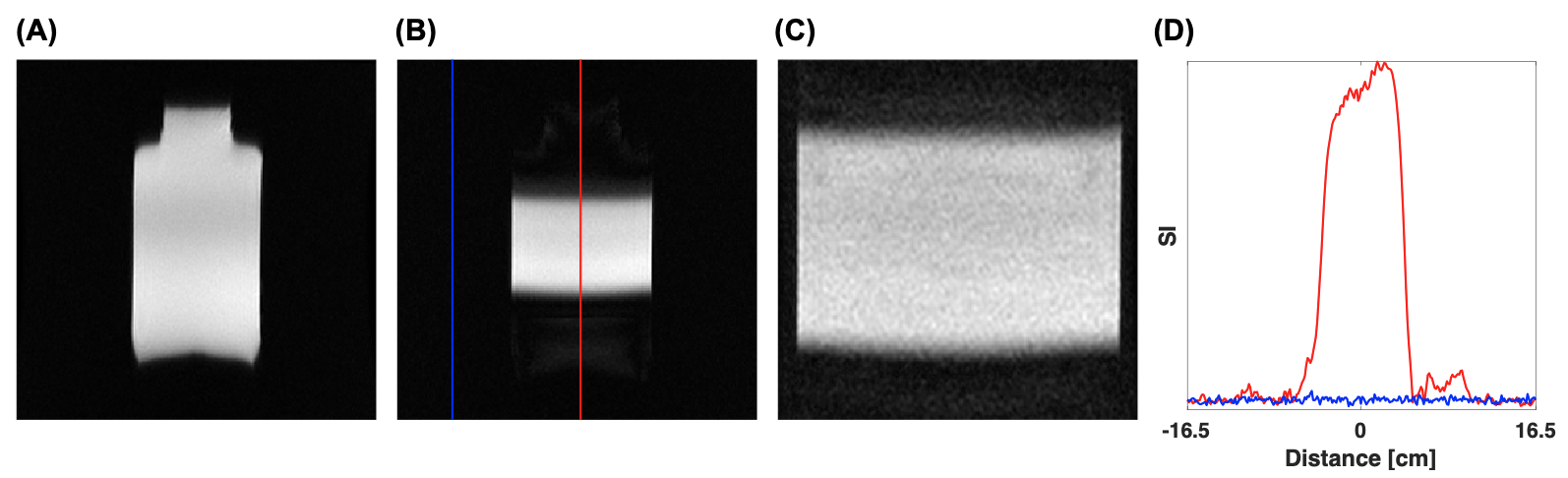
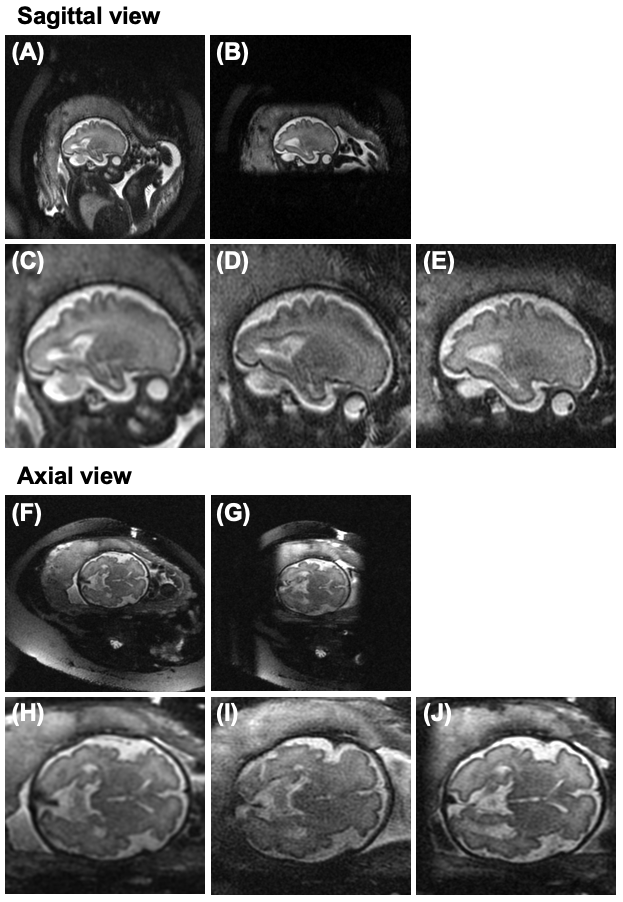
Figure 1D shows the simulated excitation profile of longitudinal magnetization after OVS preparation pulse with 15-cm passband and 15-cm saturation slabs. In Fig. 1E and F, the Mz in the passband slab (|r|<7.5 cm) were 0.99 ± 0.02 and 0.98 ± 0.09 within the range of B1 scale and off-resonance, respectively. The Mz in the saturation slab (7.5 cm<|r|<22.5 cm) were 0.20 ± 0.17 and 0.11 ± 0.22 within the range of B1 and off-resonance, respectively. In the phantom images acquired with OVS, the cross-sectional plot along the phase-encoding direction showed well-suppressed signal in the saturation bands (Fig. 2). The point spread functions of high-resolution SSFSE with a reduced FOV were similar to or sharper than conventional SSFSE for all three tissues whereas high-resolution SSFSE with a full FOV showed wider point spread functions for gray matter and white matter, suggesting blurring effects (Fig. 3). Figure 4 shows in vivo sagittal and axial fetal brain images. Full FOV SSFSE images with and without OVS preparation demonstrate signal suppression outside the region of interest (Fig. 4A-B, F-G). While both high-resolution SSFSE with a full and reduced FOV showed finer spatial resolution than conventional SSFSE, brain structures were relatively sharper in the high-resolution SSFSE images with a reduced FOV leading to overall improved image quality (Fig. 4C-E, H-J). No aliasing artifacts were observed in high-resolution SSFSE images with a reduced FOV.Discussion
Cosine-modulated Shinnar-Le Roux minimum-phase RF achieved time-efficient suppression of both sides of the outer volume in the phase encoding direction. Using this preparation pulse, 2D FOV of fetal brain imaging was reduced by approximately 85% without visible aliasing artifacts. This allowed for a greatly reduced acquisition matrix size required for a given voxel size, which could be translated to a dramatic reduction in readout time. To avoid substantial signal-to-noise ratio (SNR) loss from reduced readout time, we lowered the readout bandwidth four times with a reduced FOV. As a result, no visible SNR loss was observed in the in vivo fetal brain images while the readout time was shortened by about 40% compared to high-resolution SSFSE with a full FOV. Reduced readout time of SSFSE is expected to be more robust to fetal and maternal motion and T2 decay, leading to improved image quality. This was corroborated by our in vivo fetal brain images.Conclusion
We have demonstrated the feasibility of high-resolution fetal brain anatomical imaging using SSFSE with a reduced FOV. The increased spatial resolution may improve diagnostic accuracy for fetal brain abnormalities in utero.Acknowledgements
R01HD100012, HI19C1095References
1. Saleem SN. Fetal MRI: An approach to practice: A review. Journal of advanced research. 2014;5(5): 507-523.
2. Gholipour A, Estroff JA, Barnewolt CE, et al. Fetal MRI: a technical update with educational aspirations. Concepts in Magnetic Resonance Part A. 2014;43(6):237-266.
3. Tee LM, Kan EY, Cheung JC, Leung WC. Magnetic resonance imaging of the fetal brain. Hong Kong Med J. 2016;22(3):270-278.
4. Pauly J, Le Roux P, Nishimura D, Macovski A. Parameter relations for the Shinnar-Le Roux selective excitation pulse design algorithm (NMR imaging). IEEE transactions on medical imaging. 1991;10(1):53-65.
5. Holbrook AB, Santos JM, Kaye E, Rieke V, Pauly KB. Real-time MR thermometry for monitoring HIFU ablations of the liver. Magn Reson Med. 2010;63:365-373.
Figures