2287
Histogram analysis of diffusion kurtosis imaging of deep brain nuclei in Parkinson's disease with different motor subtypes1Medical school, Kunming University of Science and Technology, Kunming, China, 2Department of MRI, the First People’s Hospital of Yunnan Province, Kunming, China, 3Department of Neurology, the First People’s Hospital of Yunnan Province, Kunming, China, 4MR Scientific Marketing, Siemens Healthineers Ltd., Kunming, China
Synopsis
Keywords: Parkinson's Disease, Gray Matter
Parkinson's disease (PD) has significant clinical heterogeneity. According to its motor symptoms, PD could be divided into two principal clinical subtypes: tremor-dominant (TD) and postural instability and gait disorder (PIGD). Identifying clinical subtypes of PD could serve to better understand the underlying disease mechanisms, predict progression, and guide treatment. In this study, diffusion kurtosis imaging (DKI) combined with histogram analysis were used to evaluate the microstructural changes of the deep brain gray matter nuclei in PD patients. And it demonstrated that DKI histogram analysis was useful to diagnose and discriminate different motor subtypes of PD.
Purpose
To evaluate the diagnostic and differential efficacy of diffusion kurtosis imaging (DKI) histogram analysis for different motor subtypes of Parkinson's disease (PD) and explore the relationship between histogram features and clinical indicators.Methods
A total of 70 PD patients (39 males and 31 females) and 36 age- and sex-matched healthy controls (HC) were prospectively enrolled. There were 40 patients with postural instability and gait disorder (PIGD) (22 males and 18 females) and 30 patients with TD (17 males and 13 females). All subjects underwent MR imaging on a 3.0T superconducting scanner (GE Signa HDXt, America) with a 8-channel head coil. The parameters of DKI were as follows: repetition time (TR)=13200ms, echo time(TE)=95.3ms, slice thickness=2.5mm, slice distance=2.5mm, incentive times=1, field of view=240mm2, bandwidth=62.5Hz, matrix=256×256, 50 diffusion gradient directions, b-values=0, 1250 and 2500 s/mm², and acquisition time=13min43sec. The DKI raw images were post-processed by the Functool software of GE Advantage Workstation 4.7 workstation to obtain pseudo-color maps of DKI quantitative parameters, including mean kurtosis (MK), axial kurtosis (Ka), radial kurtosis (Kr) and the reference map T2-weighted-trace. Import these above DICOM format images into FireVoxel software (https://www.firevoxel.org/) to obtain histogram features. The region of interest (ROI) was manually drawn on the MK, Ka and Kr maps showing the maximum cross section of each nucleus with reference to the T2-weighted-trace maps. ROI includes bilateral red nucleus (RN), substantia nigra pars reticulate (SNpr), substantia nigra pars compacta (SNpc), head of caudate nucleus (CN), globus pallidus (GP), putamen (PUT), thalamus (TH) and dentate nucleus (DN). As showing in Figure 1. The corresponding DKI histogram features, including minimum intensity (min), maximum intensity (max), mean intensity (mean), standard deviation (stddev), coefficient of variation (CV), skewness, kurtosis, entropy, and 10th, 25th, 50th, 75th, and 90th percentiles (P10, P25, P50, P75, P90) were extracted. Statistical analyses were performed with SPSS statistical software (version 26.0, IBM Corporation, Armonk, NY) and MedCalc statistical software (version 20.114, Ostend, Belgium). The chi-square test was applied to compare the gender distribution between the PD patients and HC. The Kolmogorov-Smirnov test was used to assess whether continuous variables conformed to a normal distribution, and all measures were expressed as mean±standard deviation. Independent samples t-test (normal distribution) or Mann-Whitney U-test (non-normal distribution) was applied to compare the ages, MMSE score, tremor score, PIGD score and all of the histogram features. Receiver operating characteristic (ROC) curves were applied to evaluate the diagnostic performance of all statistically significant histogram features according to the area under curve (AUC) of ROC curve. MedCalc software was used to calculate the sensitivity, specificity, 95% confidence interval (CI) and Youden index for the significant histogram features. A multifactorial logistic regression analysis was also performed to identify the best combined model for diagnosis. Interobserver agreement of histogram features was evaluated by intraclass correlation coefficient (ICC), which interpreted as follows: 0.8-1.0, excellent; 0.6-0.8, good; 0.4-0.6, medium; < 0.4, poor. Correlation analysis of each histogram feature with clinical features was performed by pearson or spearman correlation analysis. P < 0.05 was considered considered statistically significant.Results
Some DKI histogram features were significantly different between PD patients and HC, and also different between patients with PIGD and TD (all P < 0.05) (Figure 2). MK-SNprkurtosis, Ka-SNpcP50 and Kr-SNpcP90 showed the highest AUC for distinguishing patients with PIGD from HC, respectively. MK-SNpcP10, Ka-SNpcP25 and Kr-CNP90 had the highest AUC for distinguishing patients with TD from HC, respectively. MK-PUTP10 combined with Ka-RNkurtosis yielded the highest diagnostic performance with an AUC of 0.762 for distinguishing patients with PIGD from TD (Table 1, Figure 3). Certain DKI histogram features were correlated with H&Y stage, MMSE score, tremor score, and PIGD score (all P < 0.05) (Figure 4 showed the correlation between the most strongly correlated histogram features and each clinical feature).Discussion
At present, there was no consensus on the altered microstructure of deep brain nuclei in PD patients. In this study, the combination of DKI parameters with histogram analysis confirmed the value of DKI histogram features for showing the distribution of PD microstructural changes. Compared with the previous studies, the histogram analysis could not only reflect the average level of parameter values, but also quantify the distribution of nuclei microstructure beyond the mean values, and the results are more comprehensive and accurate. DKI combined with histogram analysis is helpful to show the distribution of brain microstructural changes and to distinguish different motor subtypes in PD patients, and has the potential to be used as an imaging index to evaluate the clinical indicators of the disease.Conclusion
DKI combined with histogram analysis could comprehensively reflect the microstructure changes and inhomogeneity of deep brain nuclei in PD patients beyond the mean values. Some DKI histogram features were correlated with clinical stage and score, which could provide a useful method for the diagnosis of PD patients and the differentiation of different motor subtypes.Acknowledgements
We sincerely thank Technician Qing Li and Fan Ding for his guidance on the post-processing operation.
References
No reference found.Figures
Figure 1. The region of interests (ROIs) were manually drawn on the MK, Ka and Kr maps showing the maximum cross section of each nucleus with reference to the T2-weighted-trace maps. ROIs includes bilateral head of caudate nucleus (CN), globus pallidus (GP), putamina (PUT), thalamus (TH), red nucleus (RN), substantia nigra pars compacta (SNpc), substantia nigra pars reticulate (SNpr) and dentate nucleus (DN).
Figure 2. The results of histogram features of MK (a), Ka (b), and Kr (c) values between PD patients and healthy controls and between PIGD and TD subtypes. * indicates P < 0.05.
Figure 3. ROC curves of MK-SNprkurtosis, Ka-SNpcP50, Kr-SNpcP90 and their combinations for differentiating PIGD-PD patients from healthy controls (a). ROC curves of MK-SNpcP10, Ka-SNpcP25, Kr-CNP90 and their combinations for differentiating TD-PD patients from healthy controls (b). ROC curves of MK-PUTP10, Ka-RNkurtosis and their combinations for differentiating PIGD-PD patients from TD-PD patients (c).
Figure 4. The correlation between most strongly correlated histogram features and each clinical indicator. MK-CNmin of PD patients is positively correlated with the H&Y stage (a). MK-PUTCV of PD patients is negatively correlated with MMSE score (b). The Kr-GPP10 of PD patients is positively correlated with the tremor score (c). The Ka-CNskewness of PD patients is positively correlated with the PIGD score (d).
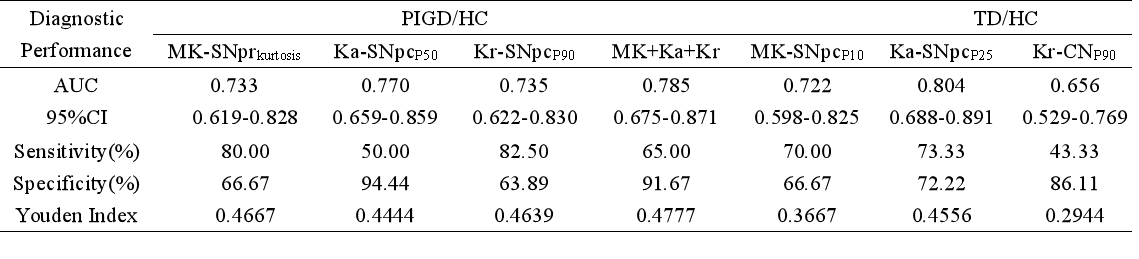
Table 1. Diagnostic Performance of Best DKI Histogram Features and Combined Model.