2260
Evaluating blood supply changes in the osteonecrosis of the femoral head using gadobutrol-based steady-state MRA1Deyang People's Hospital, Sichuan, China, 2Philips Healthcare, Chengdu, China
Synopsis
Keywords: Joints, Vessels, osteonecrosis of the femoral head
Dynamic evaluation of retinacular arteries is essential for understanding blood supply changes occurring in osteonecrosis of the femoral head (ONFH). The steady-state (SS) magnetic resonance angiography (MRA) may be an effective method as our previous study suggested, however its feasibility is yet to be determined. Therefore, this study intends to use gadobutrol-based SS MRA to evaluate the blood supply of ONFH.Introduction
Dynamic evaluation of retinacular arteries is essential for understanding blood supply changes occurring in osteonecrosis of the femoral head (ONFH) [2]. Due to their mini diameter (mean of 0.47-0.66 mm) [3], only rare imaging techniques could reveal these small vessels reliably. The invasive superselect DSA is recommended as the primary method to provide pre-clinic imaging data due to its high resolution [4], While computed tomography angiography is a noninvasive technique of vascular imaging of the femoral head but with limited reliability and inability to show intraosseous vessels [5]. The SS MRA was successfully applied to demonstrate the distributions of the three groups of normal retinacular arteries however its feasibility of evaluation of blood supply changes in ONFH is yet to be determined [1]. Therefore, this study intends to use gadobutrol-based SS MRA to evaluate the blood supply of ONFH.Materials and Methods
From December 2021 to May 2022, a total of 47 patients (including 12 cases that were unilaterally affected, 13 cases that were bilaterally affected but with surgical intervention in only one hip, and 22 cases that were bilaterally involved and had no surgical intervention) with 69 diseased hips without surgical intervention and 10 healthy volunteers with 20 healthy hips were consecutively involved in this prospective study. The ethics committee of the hospital approved the study. All subjects signed informed consent before the SS MRA examination. A 3T MR scanner (Philips Healthcare, Ingenia, Netherlands) with a 32-channel torso coil spanning the bilateral hip joints was used in this study to accomplish SS MRA, using T1 fast field echoes sequence with coronal scan. The spectral presaturation with inversion recovery technique was applied to suppress the fat background. After completion of the localization scan, a 0.1 mmol/kg gadobutrol (Bayer Healthcare) was injected at 1.5 ml/s, followed by a 20-ml saline flush injected at 2.0 ml/s, using a high-pressure syringe (Vasovist, Bayer Schering, Berlin, Germany). The detailed parameters of SS MRA were adopted as follows: field of view = 250 × 370 × 116 mm3, acquisition voxel size = 0.8 × 0.8 × 0.8 mm3, reconstruction voxel size = 0.4 × 0.4 × 0.4 mm3, slice number = 290, oversample factor (slice direction)= 1.2, flip angle= 30o, TR / TE = 18 ms / 2.5 ms, SENSE acceleration factor (phase direction) = 2, Halfscan factor = 0.65, number of signal-averaged = 1, water-fat shift = 1, and the acquisition time was five minutes and nine seconds. Based on the SS MRA, the retinacular arteries were quantified using “slicer” software as follows: The number of the retinacular arteries, including the overall retinacular arteries (ORA), superior retinacular arteries (SRA), inferior retinacular arteries (IRA) and anterior retinacular arteries (ARA), which were compared between healthy and ONFH hips and between hips across Association Research Circulation Osseous (ARCO) staging I-IV [2]. The affected rates of the SRA and IRA were also compared between healthy and ONFH hips and between hips with stages I-IV.Results
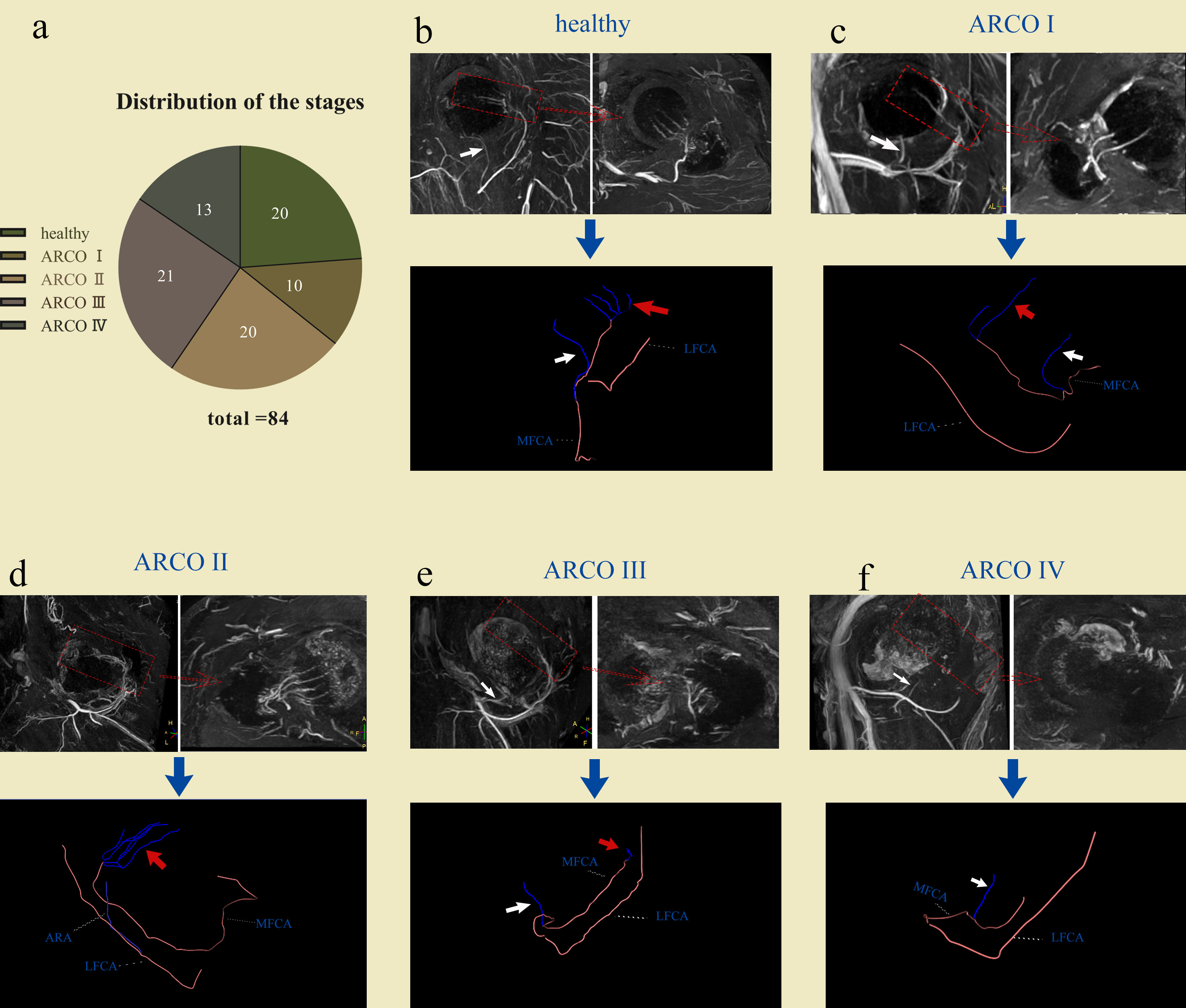
Twenty healthy hips and 64 ONFH hips with ARCO I-IV were successfully evaluated in 54 participants (10 healthy volunteers, 7 males, aged 50 [42, 55]; 44 patients, 37 males, aged 49.75 ± 11.76). There were significant differences between ARCO I-IV for the number of ORAs (mean of 3.5 ± 1.5, 2.3 ± 1.3, 1.7 ± 1.4, and 0.8 ± 0.8 for ARCO I-IV, respectively; p < .001), SRAs (median of 2.5, 1, 0.5 and 0 for ARCO I-IV, respectively; p < .001) and the affected rate of SRAs (20.00%, 65.22%, 77.78%, 92.31% for ARCO I-IV, respectively, p = 0.002). There were significant differences between ONFH and healthy hips for the number of ORAs (median of 5 vs. 2; p < .001), SRAs (median of 3 vs. 1; p < .001), IRAs (median of 1 vs. 1; p < .001), ARAs (median of 0 vs. 0; p = 0.04), and also the affected rate of SRAs (5.00% vs. 67.20%, p < .001) and IRAs (30 % vs. 84.4%, p < .001). Example cases were provided in Figure 1.Conclusion
In conclusion, the main nutrient arteries, including superior and inferior retinacular arteries, were successfully evaluated using gadobutrol-enhanced steady-state magnetic resonance angiography for healthy and ischemic necrotic femoral heads. These results indicated that gadobutrol-enhanced magnetic resonance angiography is a feasible method to aid in the diagnosis and dynamic evaluation of blood supply for osteonecrosis of the femoral head.Acknowledgements
NONEReferences
1 Liao Z, Bai Q, Ming B, Ma C, Wang Z, Gong T (2020) Detection of vascularity of femoral head using sub-millimeter resolution steady-state magnetic resonance angiography-initial experience. Int Orthop 44:1115-1121
2 Yoon BH, Mont MA, Koo KH et al (2020) The 2019 Revised Version of Association Research Circulation Osseous Staging System of Osteonecrosis of the Femoral Head. J Arthroplasty 35:933-940
3 Zhao D, Qiu X, Wang B et al (2017) Epiphyseal Arterial Network and Inferior Retinacular Artery Seem Critical to Femoral Head Perfusion in Adults With Femoral Neck Fractures. Clin Orthop Relat Res 475:2011-2023
4 Chi Z, Wang S, Zhao D, Wang B (2019) Evaluating the Blood Supply of the Femoral Head During Different Stages of Necrosis Using Digital Subtraction Angiography. Orthopedics 42:e210-e215
5 Zlotorowicz M, Czubak J, Kozinski P, Boguslawska-Walecka R (2012) Imaging the vascularisation of the femoral head by CT angiography. J Bone Joint Surg Br 94:1176-1179
Figures