2253
Differentiation between HCC and ICC using 3D amide proton transfer weighted imaging and diffusion kurtosis imaging1Department of Radiology, The First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Engineering Research Center for Artificial Intelligence in Medical Imaging, Dalian, China, 3Clinical & Technical Support, Philips Healthcare, Beijing, China
Synopsis
Keywords: Liver, CEST & MT
Hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC) are the two most common primary intrahepatic malignant tumors, and the prognosis and treatment methods are significantly different between them. The purpose of this study was to explore the diagnostic ability of APTw and DKI in distinguishing ICC from HCC. When the APTw values were combined with DKI parameters, the AUC was improved from 0.760 to 0.784 and the sensitivity reached 100%. Our preliminary study showed that APTw combined with the mean diffusivity and kurtosis anisotropy values drived from DKI demonstrated a better performance in the differential diagnosis of HCC and ICC.Purpose
Hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC) are the two most common primary intrahepatic malignant tumors, and the prognosis and treatment options are significantly different between them [1]. Therefore, it is important to make an accurate diagnosis for ICC and HCC. However, some atypical ICC have many demographic, clinical, and MRI similarities with HCC. It is difficult to distinguish them using the conventional methods including contrast enhancement [2]. Amide proton transfer-weighted imaging (APTw) is a noninvasive molecular imaging technique that can measure the concentration of free proteins and polypeptides in tissues without the use of exogenous contrast agents, and it may reflect the microscopic information of diseased tissues [3]. Diffusion kurtosis imaging (DKI) which reflect the properties of non-Gaussian water molecules diffusion in tissues was recently be used in the histologic grading of HCC[4]. However, few studies have explored the ability of both in primary liver cancer diagnosis. Therefore, the purpose of this study was to explore the diagnostic ability of APTw and DKI in distinguishing ICC from HCC.Materials and Methods
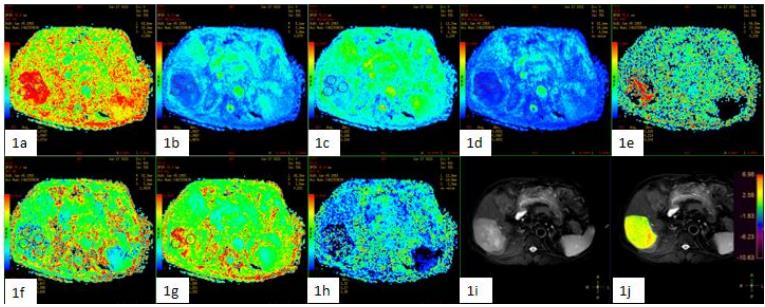
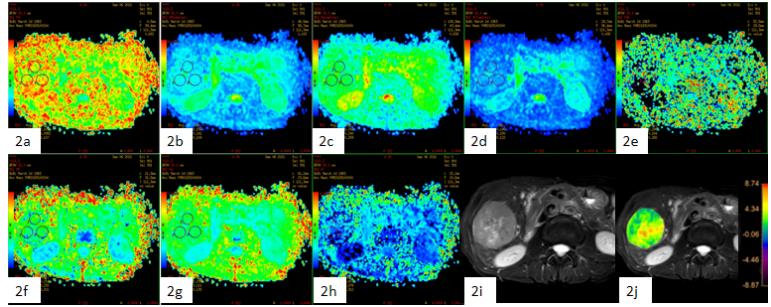
28 patients (with clinical symptoms and MRI image characteristics of primary liver cancer) were recruited in this study, which consisted of 19 HCC patients (13 men, 5 women; mean age, 55 years; range, 24–72 years) and 9 ICC patients (5 men, 4 women; mean age, 52 years; range, 28–68 years). All patients were scanned using a 3.0 T MR scanner (Ingenia CX, Philips Healthcare, the Netherlands). 3D-APTW imaging was performed using a 3D fat-suppressed echo (FSE) sequence at seven different frequency offsets (± 3.0, ± 3.5, ± 4.0, and − 1560 ppm). This specific MTRasym was presented as APTW%. DKI data was acquired before the administration of contrast agent using a single-shot echo-planar (SS-EPI) diffusion sequence under free breathing. xxx b-values (0, 200, 700, 1,400, and 2,100 s/mm2) in three orthogonal directions were used. The DKI parameter maps were generated using Functool software on a GE AW 4.6 workstation. An experienced radiologist manually placed the ROIs (100 - 200 mm2) on the axial slice of fusion of T22WI and APTw images, and DKI parameter images with the largest lesions according to the high-resolution T2W images (Figure 1, 2). APTw values (in percent, representing the magnetization transfer ratio asymmetry in the z-spectrum) and DKI parameters were compared between the HCC and ICC groups using the Mann-Whitney U test, respectively. ROC curves were used to analyze the diagnostic efficiency of APTw, DKI and joint use strategy in HCC and ICC. The diagnostic values of the combination of APTw and DKI were calculated by logistic regression. A p -value < 0.05 was considered statistically significant.Results
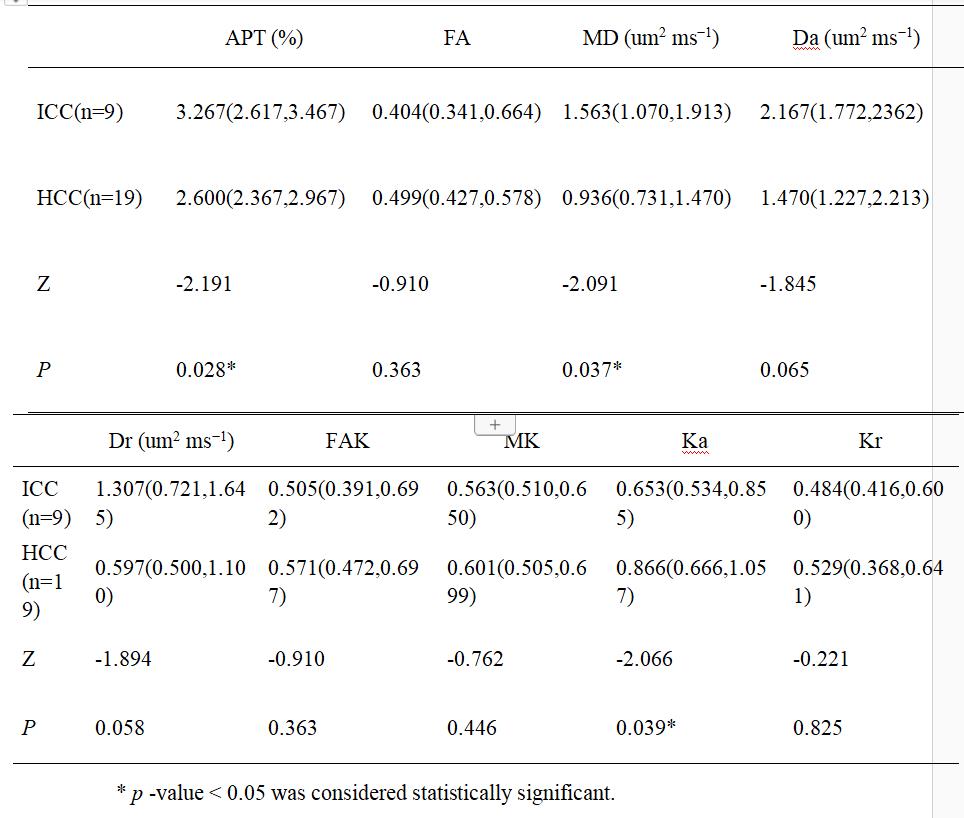
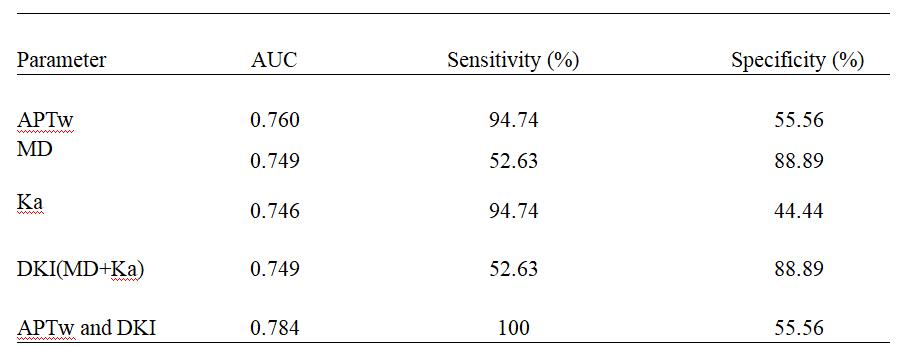
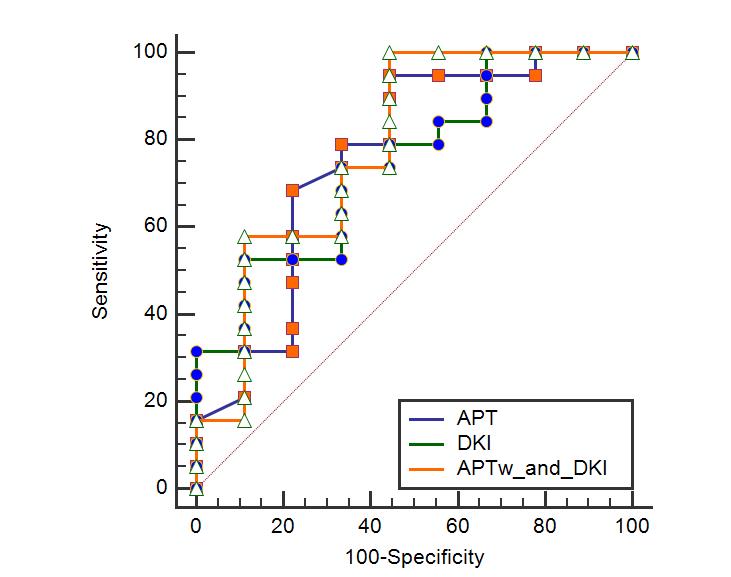
The values of APTw and DKI parameters from HCC and ICC patients were shown in Table 1. APTw, MD, and Ka showed a significant difference between HCC and ICC groups, whereas the others did not. The ROC analyses revealed the diagnostic performance of APTw, MD and Ka in differentiating HCC from ICC, with AUCs of 0.760, 0.749,and 0.746, respectively (Table 2). The AUCs of APTw, DKI(MD+Ka), and APTw combined with DKI(MD+Ka) were 0.760, 0.749 and 0.784. When joint use of APTw and DKI, the sensitivity was 100%, and the specificity was 55.56% (Figure 3).Discussion and conclusion
ICC is histologically characterized by adenoid secretion or mucous secretion, and thus elevation of mobile proteins and peptides. This might be the reason why APTw values are higher for ICC than HCC. Histologically, tumor cells in HCC show higher cell density and more heterogeneous cell morphology, which alter the diffusion properties of water significantly. Therefore, DKI is sensitive for HCC. When the APTw values were combined with DKI parameters, the AUC was improved from 0.760 to 0.784 and the sensitivity reached 100%. In conclusion, the combination of APTw and DKI could enhance the diagnosis of HCC and ICC in primary liver cancer.Acknowledgements
No acknowledgement found.References
[1] Sia D., Villanueva A., Friedman S. L., Llovet J. M. Liver cancer cell of origin, molecular class, and effects on patient prognosis. Gastroenterology . 2017;152(4):745–761. doi: 10.1053/j.gastro.2016.11.048
[2] Wengert G. J., Baltzer P. A., Bickel H., Thurner P., Breitenseher J. Differentiation of intrahepatic cholangiocellular carcinoma from hepatocellular carcinoma in the cirrhotic Liver using Contrast-enhanced MR Imaging. Academic Radiology . 2017;24(12):1491–1500. doi: 10.1016/j.acra.2017.06.005.
[3] Zhou J,Heo HY,Knutsson L,et al. APT-weighted MRI: Techniques, current neuro applications, and challenging issues [J]. Journal of magnetic resonance imaging : JMRI, 2019,50(2):347-364.
[4] Cao L, Chen J, Duan T, et al. Diffusion kurtosis imaging (DKI) of hepatocellular carcinoma: correlation with microvascular invasion and histologic grade. Quant Imaging Med Surg. 2019 Apr;9(4):590-602. doi: 10.21037/qims.2019.02.14. PMID: 31143650; PMCID: PMC6511714.
Figures