2247
Hepatocellular carcinoma with central scar: imaging findings of gadoxetic acid-enhanced MRI and pathological features1the Third Affiliated Nantong Hospital of Nantong University, Nantong, China, 2Philips Healthcare, Beijing, China, 3Philips Healthcare, Shanghai, China
Synopsis
Keywords: Liver, Cancer, HCC
central scar is not a rare feature of conventional non-fifibrolamellar HCC. The dynamic enhancement mode of Gd-EOB-DTPA was helpful to distinguish inflammatory, collagenous, and vascular scars. The EOB “target sign” had a certain characteristic but non-specific, which still needed to be combined with MRI features of the mass.Introduction
Central scars frequently occur in fibrolamellar HCC, which is a specific histological variant of HCC with a reported incidence of 20–71%1. Other hepatic masses that can have central scars include focal nodular hyperplasia (FNH)2, intrahepatic cholangiocarcinoma (ICC)3, cavernous hemangioma, and hepatic adenoma4.Central scars are rarely seen in conventional HCC, although an area of intratumoral hemorrhage or necrosis in large HCCs may mimic central scar5. To our knowledge, few reports are available on imaging features of conventional HCCs with central scars in a large case series1. Gd-EOB-DTPA enhanced MRI is now widely used to assess hepatic tumors6. Thus, we conducted this study to analyze the imaging findings of Gd-EOB-DTPA enhanced MRI and pathological features of HCC with central scar.Methods
17 cases of HCC confirmed by surgery and pathology in the third affiliated Nantong hospital of Nantong university from May 2016 to January 2022 were retrospectively analyzed, all of whom underwent preoperative Gd-EOB-DTPA-enhanced MRI and showed a central scar sign. According to different pathological properties of central scars, there were categorized into three types: inflammatory, vascular, and collagenous. The maximum diameter, basic MRI signs, enhancement characteristics of dynamic multiphase and dynamic enhancement mode of mass and central scar were analyzed. Independent sample t-test or Fisher's exact test were used to compare the imaging findings of central scars with different pathological types.Results
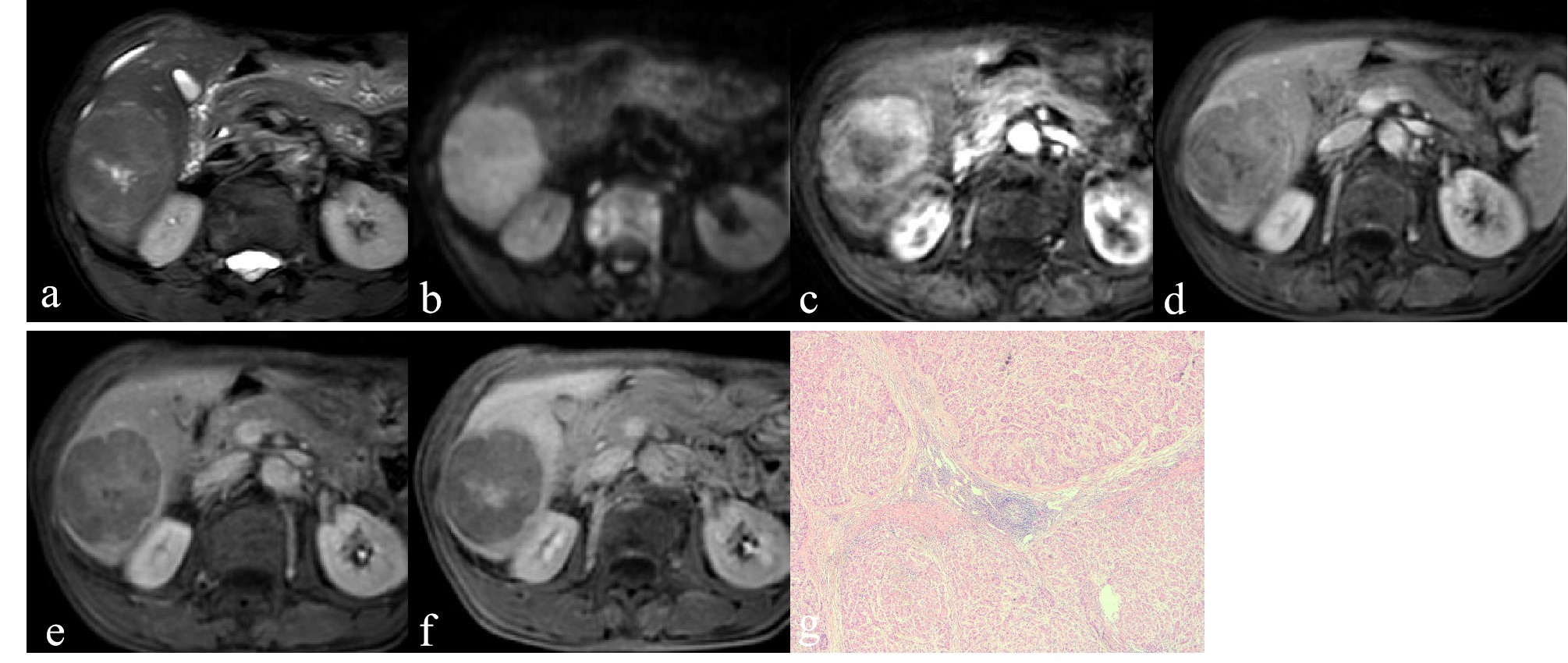
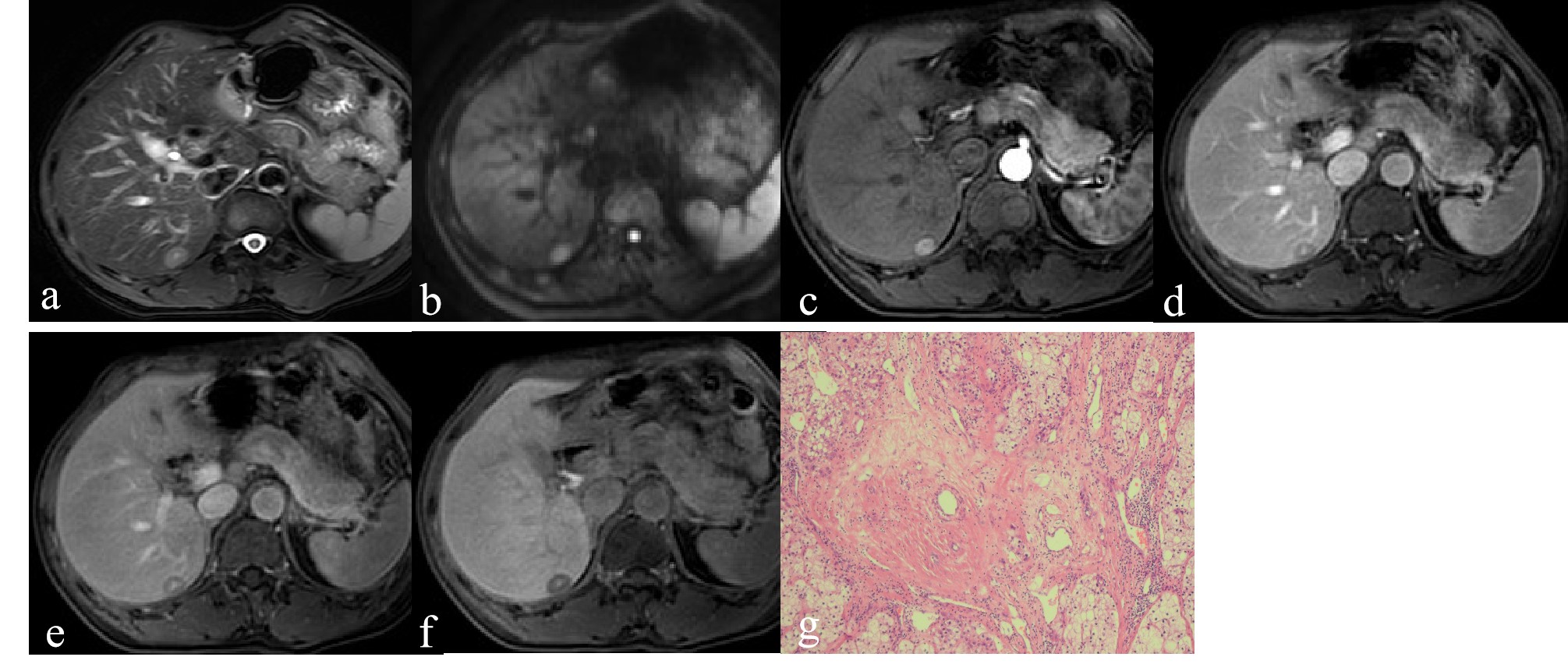
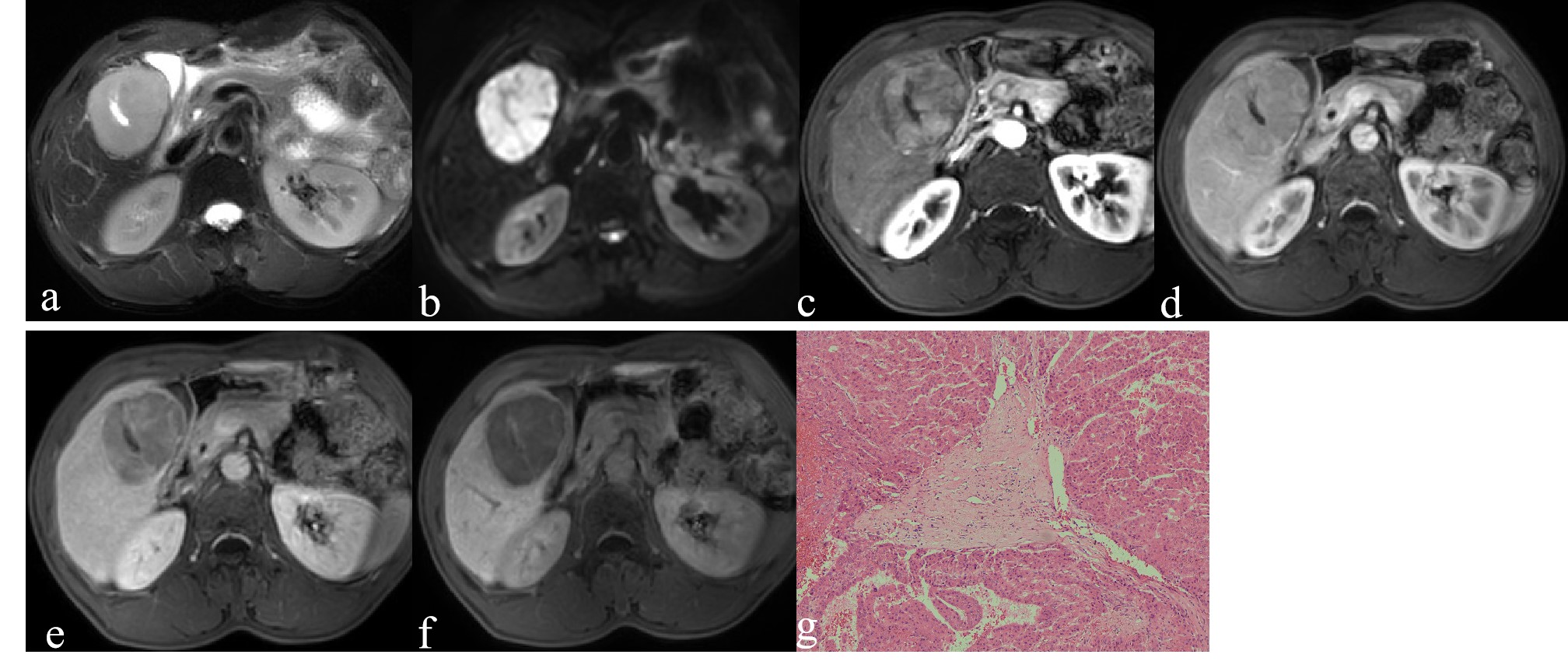
All the 17 cases were single lesions, including inflammatory scar (n = 8), vascular scar (n = 5) and collagen scar (n = 4). Pathology revealed that the main components of three types of central scars were fibrous tissue. The mass mean maximum diameters were (53.6±20.7) mm, all masses were hyperintense on T2WI and DWI. Most masses (15/17, 88.2%) showed “wash-in with wash-out” dynamic enhancement mode, and “wash-in without wash-out” enhancement mode was rare (3/17, 17.6%). All masses were hypointense on HBP. Central scar mean maximum diameters were (20.0±10.9) mm. All central scars were mostly hyperintense on T2WI (16/17, 94.1%) and hypointense on DWI (9/17, 52.9%). Most central scars showed delayed enhancement (10/17, 58.8%), followed by no delayed enhancement (7/17, 41.2%). On HBP images, central scars mainly showed EOB "target sign" hyperintense (14/17, 82.4%), and the rest were hypointense (3/17, 17.6%). Both inflammatory and vascular scars showed hyperintense on T2WI, and collagenous scars showed hypointense (n = 1) or hyperintense (n = 3) on T2WI. Inflammatory and collagenous scars showed delayed enhancement (n = 3, n = 2,respectively) or no delayed enhancement (n = 5, n = 2,respectively), and all vascular scars showed delayed enhancement (n = 5). The maximum diameter, basic MRI signs(T2WI and DWI), and HBP findings between inflammatory, collagenous, and vascular scars were no significant differences (all P>0.05). There was a significant difference in the delayed enhancement (P=0.044).Conclusion
The main component of central scar of HCC was fibrous tissue. The dynamic enhancement mode of Gd-EOB-DTPA was helpful to distinguish inflammatory, collagenous, and vascular scars. The EOB “target sign” had a certain characteristic but non-specific, which still needed to be combined with MRI features of the mass.Acknowledgements
No acknowledgement foundReferences
1. Rummeny E, Weissleder R, Sironi S, et al. Central scars in primary liver tumors: MR features, specificity, and pathologic correlation[J]. Radiology, 1989, 171:323–326.
2. Park HJ, Byun JH, Kang JH, et al. Value of discrepancy of the central scar-like structure between dynamic CT and gadoxetate disodium-enhanced MRI in differentiation of focal nodular hyperplasia and hepatocellular adenoma[J]. Eur J Radiol, 2021, 139:109730.
3. Yamamoto M, Ariizumi S, Yoshitoshi K, et al. Hepatocellular carcinoma with a central scar and a scalloped tumor margin resembling focal nodular hyperplasia in macroscopic appearance[J]. J Surg Oncol, 2006, 94(7): 587-591.
4.Yamauchi M, Asayama Y, Yoshimitsu K, et al. Hepatocellular carcinoma with a prominent vascular scar in the center: MR imaging findings[J]. Radiat Med, 2006, 24(6): 467-470.
5. Han SB, Kim YK, Min JH, et al. Hepatocellular carcinoma with central scar on gadoxetic acid-enhanced and diffusion-weighted magnetic resonance imaging[J]. Acta Radiol, 2018, 59(4):393-401.
6. Rudolphi-Solero T, Triviño-Ibáñez EM, Medina-Benítez A, et al. Differential Diagnosis of Hepatic Mass with Central Scar: Focal Nodular Hyperplasia Mimicking Fibrolamellar Hepatocellular Carcinoma[J]. Diagnostics (Basel), 2021, 12(1):44.
Figures