2241
Pre-Operative In Silico Risk Assessment for Hepatectomy Patients, Using MRI and Pharmacokinetic Modeling
Christian Simonsson1,2,3, Wolf Claus Bartholomä1,2, Anna Lindhoff Larsson4, Markus Karlsson1, Jens Tellman1, Gunnar Cedersund2,3, Bengt Norén1, Nils Dahlström1,2, Per Sandström4, and Peter Lundberg1,2
1Department of Radiation Physics, Radiology, Department of Medical and Health Sciences, Linköping University, Linköping, Sweden, 2Center for Medical Image Science and Visualization (CMIV), Linköping University, Linköping, Sweden, Linköping University, Linköping, Sweden, 3Department of Biomedical Engineering, Linköping University, Linköping, Sweden, 4Department of Surgery, Department of biomedical and clinical sciences, Linköping University, Linköping, Sweden
1Department of Radiation Physics, Radiology, Department of Medical and Health Sciences, Linköping University, Linköping, Sweden, 2Center for Medical Image Science and Visualization (CMIV), Linköping University, Linköping, Sweden, Linköping University, Linköping, Sweden, 3Department of Biomedical Engineering, Linköping University, Linköping, Sweden, 4Department of Surgery, Department of biomedical and clinical sciences, Linköping University, Linköping, Sweden
Synopsis
Keywords: Liver, Liver, Hepatectomy, Gd-DPTA-EOB, Pharmacokinetic Modeling , Risk assessment
For a range of late-stage liver disease the only curative treatment option may be hepatectomy surgery, which can have fatal complications. Therefore, a pre-operative risk assessment is vital. However, usually the assessment only investigates global liver function. For a more precise assessment, we investigate the possibility of using DCE-MRI in combination with pharmacokinetic modeling to quantify both global- and regional liver function. Also, we show a novel eight-compartment hepatic model, capable of performing an in-silico resection. We show the tentative predictive capabilities of this approach. This approach could lead to a more precise pre-operative assessment.Introduction
For a range of late-stage liver disease the only curative treatment option may be hepatectomy surgery. A complication of such surgery is post-hepatectomy liver failure (PHLF), which has an incidence of 8-12%, and may in some cases be fatal. To minimize the risk of PHLF a pre-operative risk assessment is performed to assess sufficient function and volume of the remnant tissue. Usually, liver function assessment only accounts for global liver function and does not account for any regional variability. This might be problematic, as regions, or segments, of lower function might not be identified by global function measurements and be included in the remnant liver volume. Thus, evaluation of regional function has the potential to generate a higher degree of individual precision which could benefit the pre-operative assessment. The use of dynamic contrast enhanced (DCE) MRI to assess liver function has the possibility to measure regional functionality [1-3]. Herein. we look at DCE-MRI in combination with pharmacokinetic modelling of the hepatocyte specific contrast agent, Gd-DPTA-EOB (gadoxetate), to enhance the pre-operative risk assessment for patients undergoing cancer related hepatectomyMethods
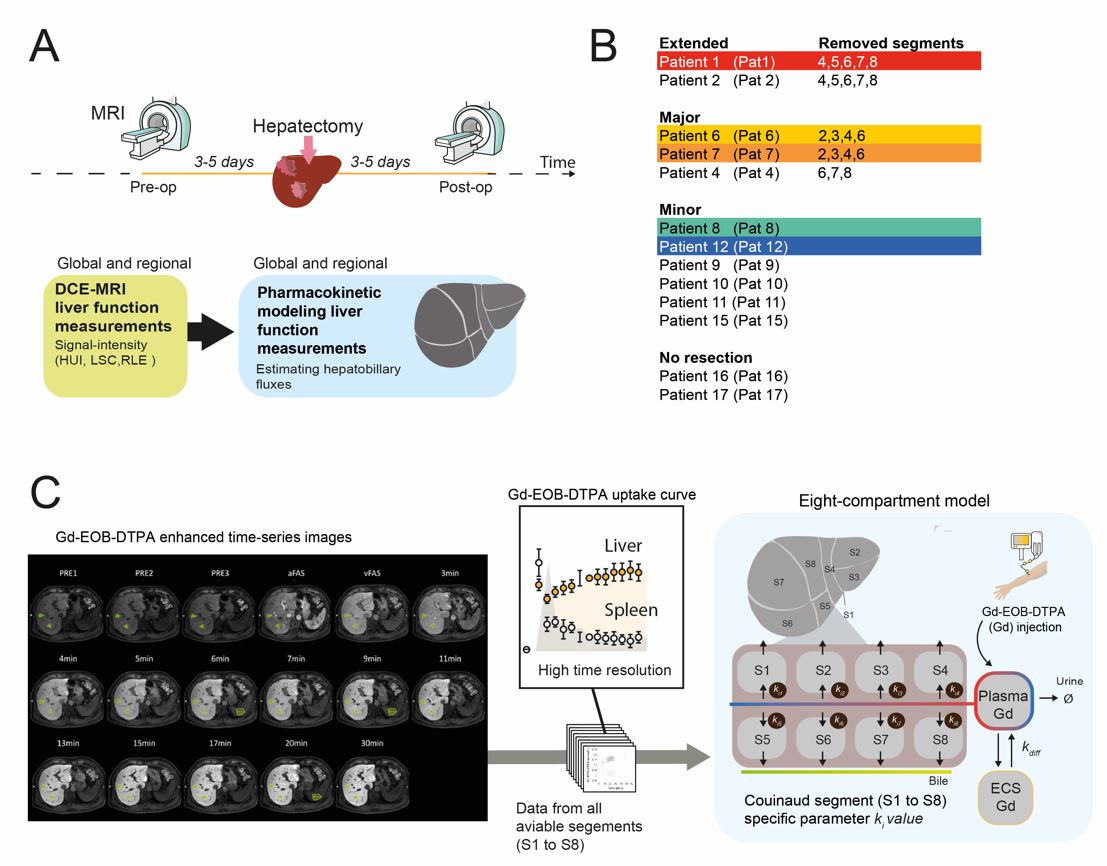
Patients (N=13 fasting) with liver metastases were examined by DCE-MRI (3 T Philips Ingenia) within 3-5 days before (n=13) and after (m =15) liver resection (Fig. 1A). Patients underwent various degrees of hepatic resection (Fig. 1B). Many of these very ill patients declined to undergo a post-surgical research examination due to a severe physical and mental load. The local ethics committee approved this study, and written informed consent was obtained from all patients.Following a bolus injection (0.025 mmol/kg body weight) of gadoxetate, images were acquired using an axial breath-hold, fat-saturated, T1-weighted, 3D gradient echo sequence. Typical image parameters included flip angle: 10°, repetition time: 4.2 ms, echo time: 2.0 ms, SENSE factor: 1.7, field of view: 300x200x350 mm3). The post‑injection images included arterial and portal venous phases, as well as time-series images acquired e.g., between 0, and 50 minutes (Fig. 1C, left).
In post-processing ROIs were placed in each of the eight Couinaud segments, plus three ROIs in the spleen, as well as ROIs in muscle, and portal vein by an experienced radiologist (BN and WB). Signal intensity measurements were obtained from each ROI, and used to estimate T1 relaxation rate (R1) and concentration of gadoxetate for each compartment (Fig. 1C, middle).
The dataset was then used to train our novel eight-compartment dynamic ODE model (Fig. 1C, right) describing the hepatobiliary fluxes of gadoxetate for each segment. This yielded segment, patient and examination-specific influx rates ki. By using the model ‘preform’ an in silico resection, using the datasets of patients having both pre-and post-examination data, we could assess any difference in uptake rate between examinations, this was quantified using the parameter kstress.
Results
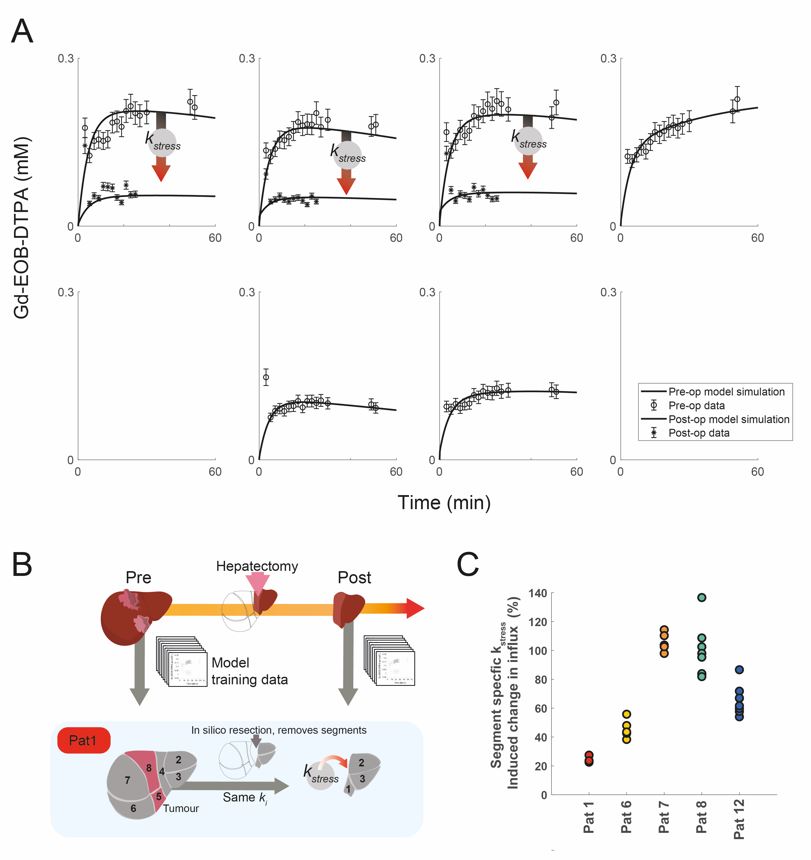
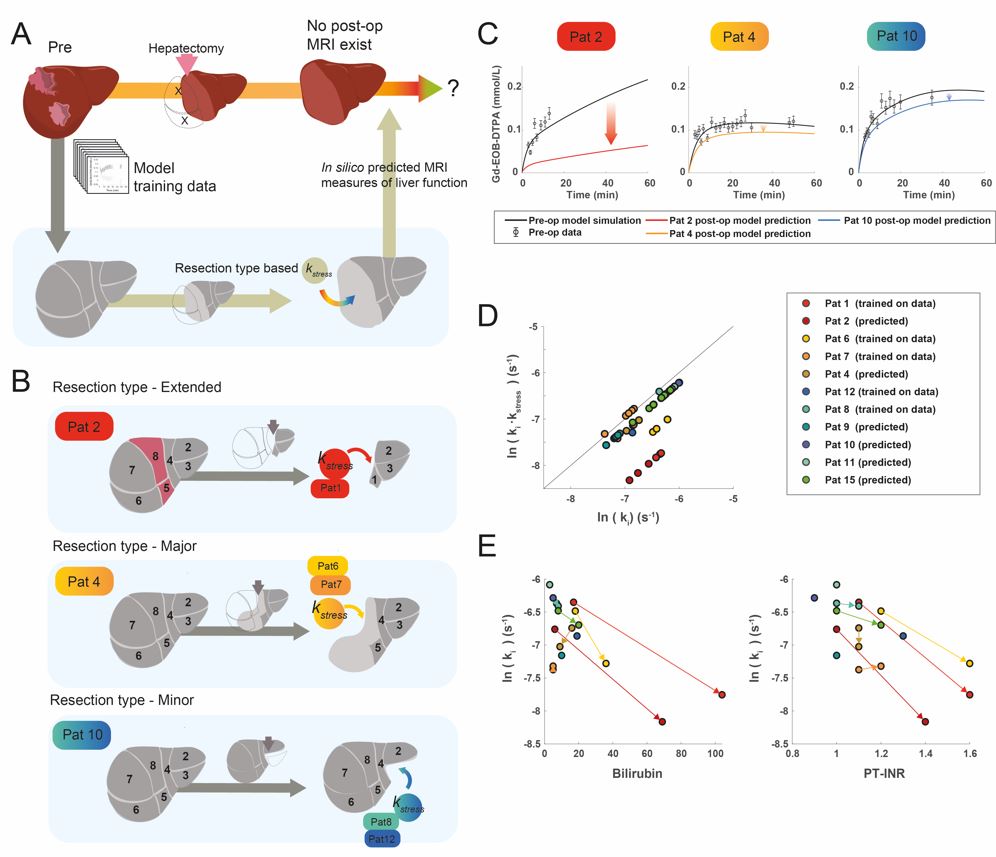
The model fit for the in silico resection for patient1 can be seen in Fig. 2A. Using this approach, we could quantify the difference in uptake function pre-and post-surgery (Fig. 2B). The difference in influx rate, kstress, pre-and post-surgery was quantified for all patients who underwent both examinations (Fig. 2C).Next, we wanted to make model prediction using only information from before the surgery (Fig. 3A). In silico resections were ‘performed’ by training the model on only pre-surgery data and using a kstress value that matched the extent of resection (Fig. 3B). The corresponding model predicted gadoxetate concentration post-surgery can be seen in Fig. 3C. The predicted change in influx can be seen in Fig. 3D. As a tentative validation we compared the new predicted influx with other measure of liver function, e.g., Bilirubin and PT-INR (Fig. 3E). The predicted drop in influx for patient2, corresponds to a higher bilirubin value, which correlates to the trend seen in patient 1 and 6. This tentatively shows the predictive capabilities of our approach.
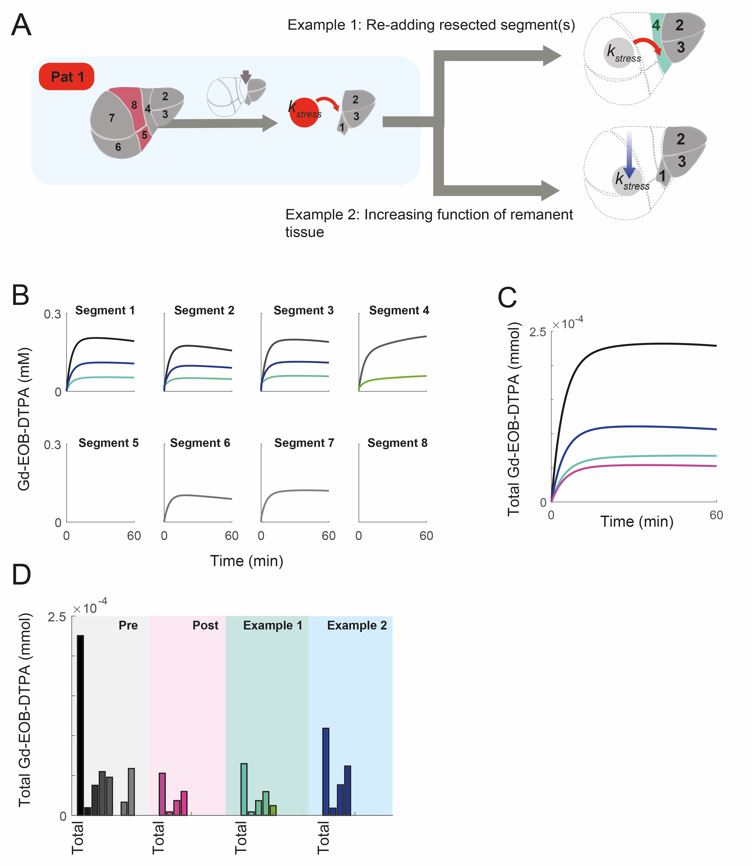
To show model usability, we show the resection scenario of patient1 (Fig. 4A). Here we highlight two examples which would lead to higher uptake after surgery. Example 1; re-adding segment four, and example 2 increased function. Simulations for each segment during these scenarios are shown in Fig. 4B, and the total hepatic gadoxetate in Fig. 4C-D. To show further capabilities of using a model-based approach, we highlight the possibility of simulating any type of resection (Fig. 5A). Corresponding simulations are shown in Fig. 5B, where yellow lines are simulations where segment are removed in order 1 to 8, and blue lines order 8 to 1. In Fig. 5C we highlight the possibility of freely changing the function of individual segments, simulations of concentration of individual segments in Fig. 5D and total liver in Fig. 5E. Changing function in larger segments yields larger effect on the total concentration.
Discussion
Herein, we present a novel approach of combining DCE-MRI assessment of liver function with an eight-compartment ODE model. We show that the approach has tentative predictive capabilities worth exploring further. There are a lot of limitations, and more validation will be needed to determine if the approach could be used for any clinical application.In conclusion, the work shown herein is a step toward better pre-operative assessments which would help limit surgical complications for already very late-stage patients.
Acknowledgements
References
1. Nilsson, H., et al., Assessment of liver function in primary biliary cirrhosis using Gd-EOB-DTPA-enhanced liver MRI. HPB, 2010. 12(8): p. 567-576.
2. Zhou, Z.-P., et al., Evaluating segmental liver function using T1 mapping on Gd-EOB-DTPA-enhanced MRI with a 3.0 Tesla. BMC Medical Imaging, 2017. 17(1): p. 20.
3. Truhn, D., et al., A New Model for MR Evaluation of Liver Function with Gadoxetic Acid, Including Both Uptake and Excretion. European Radiology, 2019. 29(1): p. 383-391.
Figures
Figure
1: A)
Study setup. Patients underwent pre- and post-operative MRI examinations B) Study cohort. C) Study data processing method
Figure
2. A) Model
fit to in silico resection for patient 1. B) Model simulation approach for
assessing the change in influx pre-and post-surgery. C) Patient and segment
specific kstress values, determining the change in influx per
segment.
Figure
3: A) Model
prediction approach. Assessing hepatic function after surgery, by only using
information available before surgery. B) In silico resection
could be made on extent of resection group basis. Patient 1 and 2 both
underwent an extensive resection. The estimated kstress value
for patient 1 was used to perform an in silico resection on patient 2. C)
Model prediction of post-surgery gadoxetate. D) Predicted changed in
influx. E) Predicted influx compared to other measure of liver function
Figure
4: A) Resection
scenario for patient 1, and example of scenarios. Example 1; re-adding segment
4, example 2; better tissue function. These simulations are based on
information from both pre-and post-surgery and are thus not clinically
relevant. However, we highlight future usability if the approach is validated.
B) Model simulation for each segment during scenarios. C) Total gadoxetate
during scenarios D) Total and segment specific values of gadoxetate.
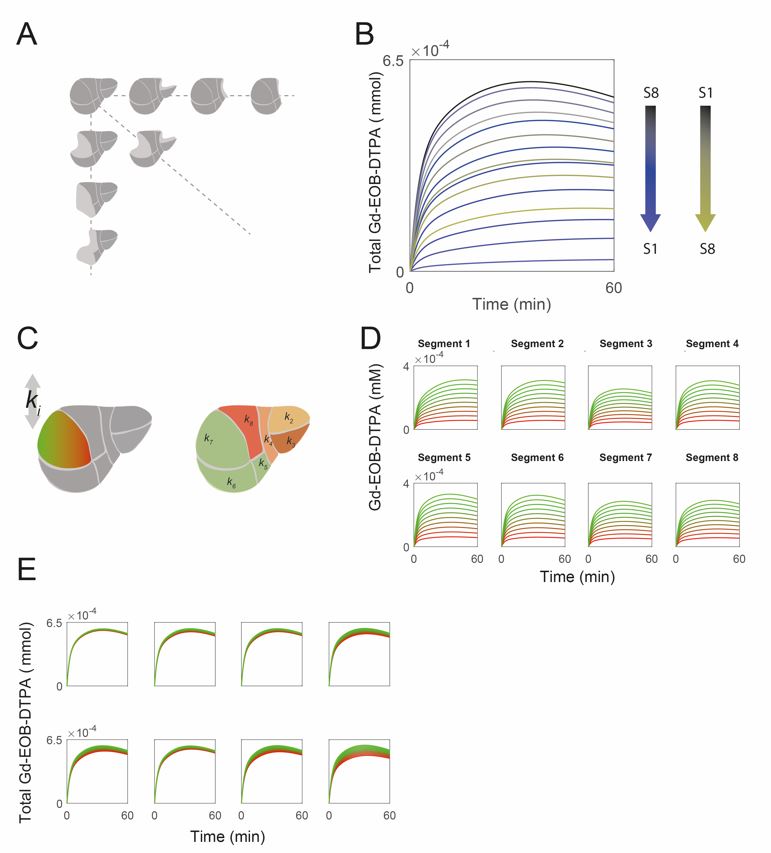
Figure
5: A) Schematic
showing the possibility of any resection/combination of segments. B) Corresponding
model simulations showing total hepatic Gadoxetate. Starting with either
removing segment 8 (blue lines) or segment 1 (yellow lines). C) Schematic
showing possibilities of changing the uptake function of each segment, and each
segment having regional function. D) Corresponding simulation showing
changes in each segment. E) Showing corresponding effect on the total
hepatic Gadoxetate
DOI: https://doi.org/10.58530/2023/2241