2199
Comparison of UTE-T1ρ vs. MAPSS-T1ρ Sequences in In-Vivo Knees
Sara E Sacher1, Michael Carl2, Hollis G Potter1, and Matthew F Koff1
1Hospital for Special Surgery, New York, NY, United States, 2GE Healthcare, San Diego, CA, United States
1Hospital for Special Surgery, New York, NY, United States, 2GE Healthcare, San Diego, CA, United States
Synopsis
Keywords: Pulse Sequence Design, Quantitative Imaging, Ultrashort echo time
The relative accuracy of an ultrashort echo time (UTE) based T1ρ sequence was compared to a MAPSS based T1ρ sequence in the evaluation of articular cartilage. Scanning with similar parameters between the acquisitions was performed, producing similar T1ρ values in all cartilage sub-compartments except for the femoral trochlea (TrF). TrF MAPSS-T1ρ values were shorter than TrF UTE-T1ρ values (10.91% difference, p = 0.0028). Overall, there was reasonable agreement between the two sequences indicating that UTE-T1ρ may be a promising method to use in place of conventional MAPSS sequences to quantify T1ρ values of articular cartilage.Introduction
T1ρ is a quantitative MRI biomarker correlated to proteoglycan content within articular cartilage and is sensitive to the severity of knee osteoarthritis (OA)1,2. Conventional T1ρ sequences employ relatively long echo times (TEs) which limit the ability to capture the signal of tissues with “short” relaxation times including certain regions of meniscus and bone. OA is a multifactorial disease involving many regions of the knee. The ability to quantitatively evaluate short-TE tissues such as the deep radial and calcified layers of cartilage, meniscus, tendon, ligament, and subchondral bone help to further elucidate changes associated with OA. Ultrashort echo time (UTE) sequences are designed to image tissues with very short relation times (< 1 ms) by capturing the signal prior to decay3,4. However, whether a UTE based T1ρ acquisition may be used in place of a conventional magnetization-prepared angle-modulated partitioned-k-space SPGR snapshots (3D MAPSS) sequences is unknown. In this study we implemented a UTE-T1ρ sequence and compared its performance against MAPSS-T1ρ.Methods
This study had IRB approval and informed written consent was obtained. 6 individuals undergoing clinical knee MRIs were sequentially recruited. All imaging was performed on a single 3T clinical scanner. Knees were scanned with UTE-T1ρ and MAPSS sequences. The acquisition parameters were as follows: UTE TSLs = 0.028, 4.6, 9.1, 13.6, 18.2, 25 ms; MAPSS TSLs = 0.032, 4.6, 9.1, 13.6, 18.2, 25 ms; field of view (FOV) = 160 mm; slice thickness = 3; mm receiver bandwidth = 488 kHz/pix. The pulse sequences were scanned at four spin lock times (TSLs) for decay curve fitting (Figure 1). Knee articular cartilage was manually segmented (ITK-SNAP 3.8.0) and subdivided into compartments consisting of the medial femoral condyle (MF), medial tibia (MT), lateral femoral condyle (LF), lateral tibia (LT), femoral trochlea (TrF), and patella (P)5 (Figure 2). T1ρ values in these regions were calculated on a pixel-by-pixel basis with a mono-exponential fit. Paired t-tests were performed to compare mean T1ρ values and the standard deviation of T1ρ values within each compartment calculated from UTE-T1ρ vs. MAPSS sequences within all subjects. A significance level of p < 0.05 was used for all analyses.Results
T1ρ values did not differ significantly between the MAPSS and UTE imaging acquisitions for any sub-compartment except TrF (Figure 3). T1ρ values in the TrF region from MAPSS imaging were shorter than those from UTE imaging (-11.54% difference, p = 0.0028) (Figure 3). Mean standard deviations (SD) of T1ρ values did not differ in any sub-compartment or in the full cartilage between MAPSS vs. UTE.Discussion
The absence of significant differences in mean T1ρ values between MAPSS vs. UTE sequences in all sub compartments, except TrF, indicates reasonable agreement between the two sequences. In addition, the absence of significant differences in standard deviations between the MAPSS and UTE acquisitions indicates the variation in T1ρ values and level of noise is in agreement between acquisitions. Further evaluation of data using histograms of the T1ρ values within individual compartments confirmed that noise variation within the TrF region was not considerably different between the sequences (Figure 4). The shorter MAPSS T1ρ values observed in the TrF sub-compartment may require further investigation into why this difference exists only in this region.Conclusion
This preliminary study indicates that T1ρ mapping using a UTE based acquisition may be considered to be a viable alternative to a MAPSS based acquisition. A UTE based acquisition may permit quantitative evaluation of tissues with short T1ρ components.Acknowledgements
HSS has an institutional research agreement with GE HealthcareReferences
1Li et al, Magn Reson Med 2008; 2Du et al, Magn Reson Imag 2011; 3Regatte et al, J acra 2004; 4Rahmer et al, Magn Reson Med 2006; 5Pedoia et al, JMRI 2016.Figures
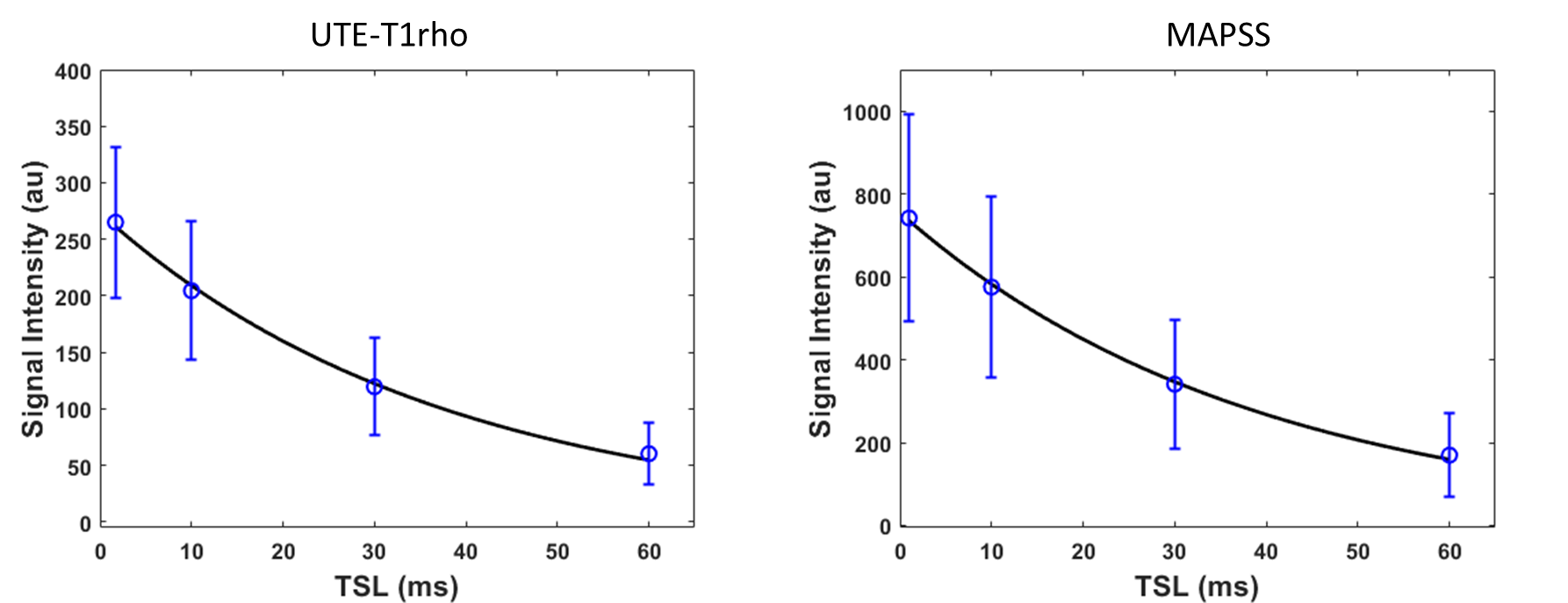
Figure 1. Representative T1ρ decay curves and best-fit curves for full cartilage of knee shown in Figure 2.
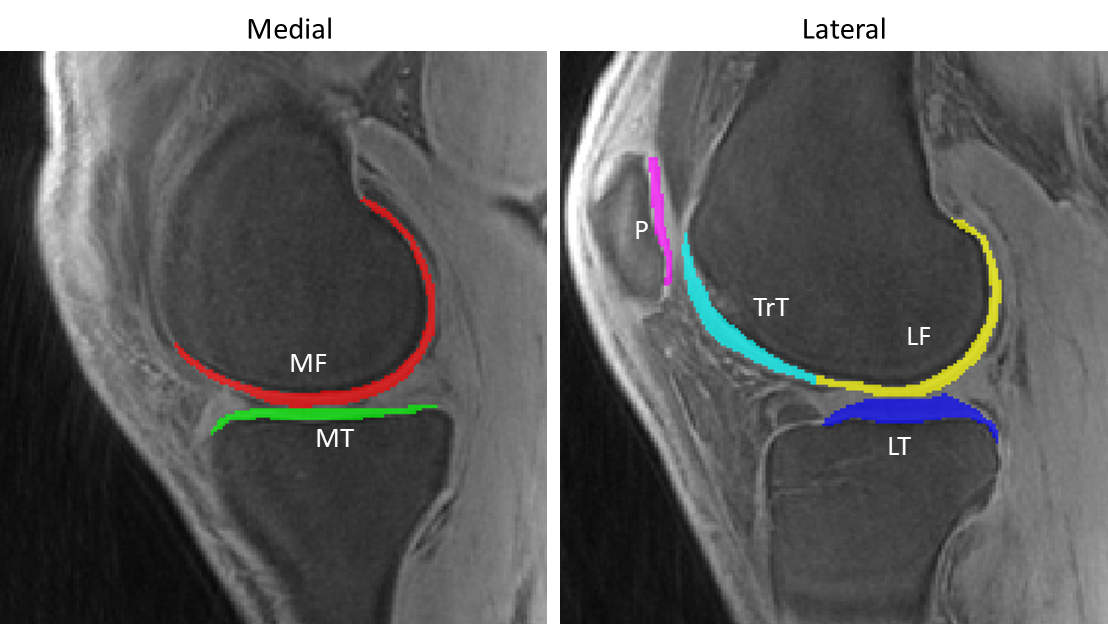
Figure 2. Knee cartilage sub-compartments.
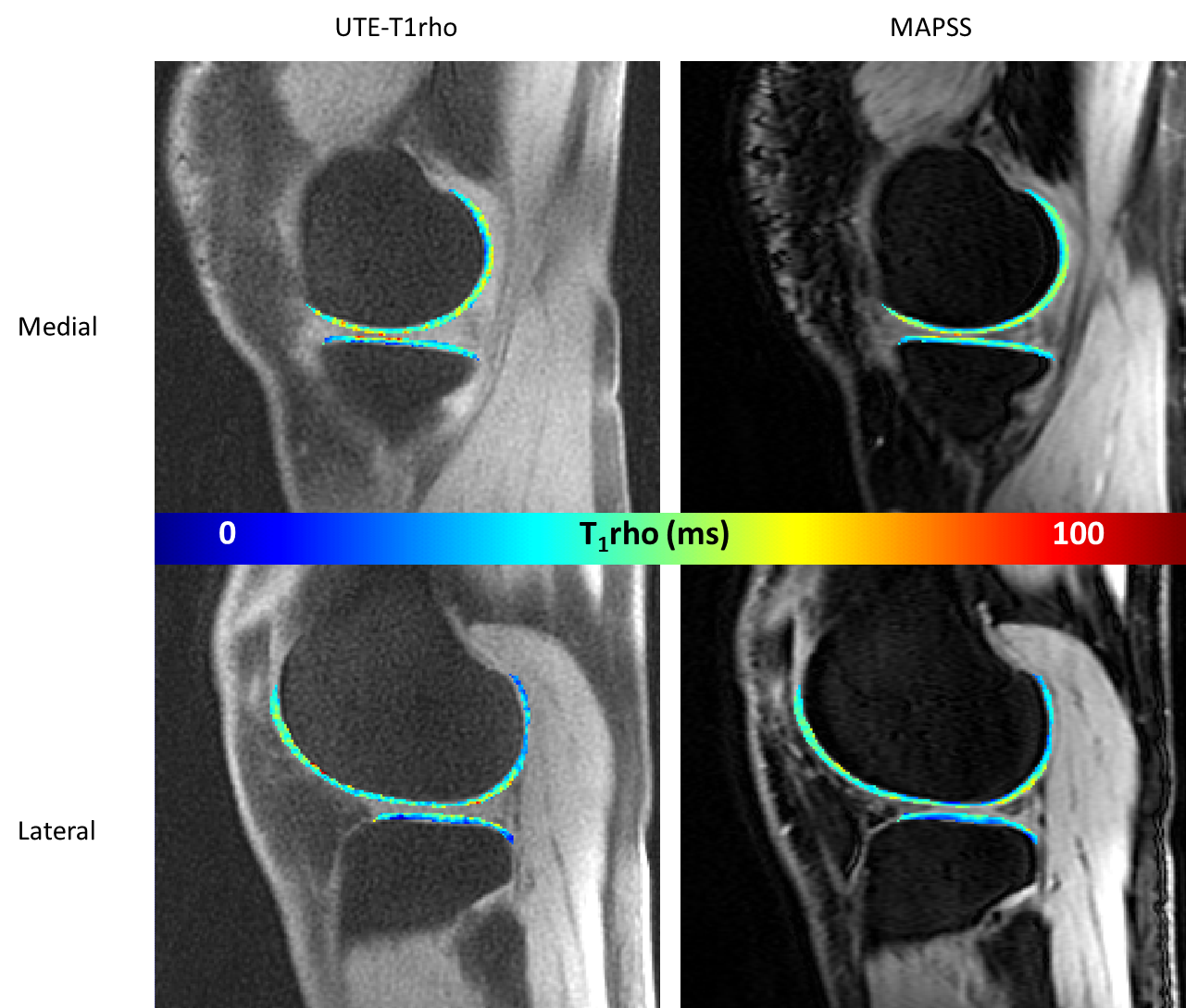
Figure 3. Representative quantitative T1ρ maps from 43 yr. old male. Mean TrF UTE-T1rho = 51.6 ms, mean TrF MAPSS-T1rho = 44.4 ms.
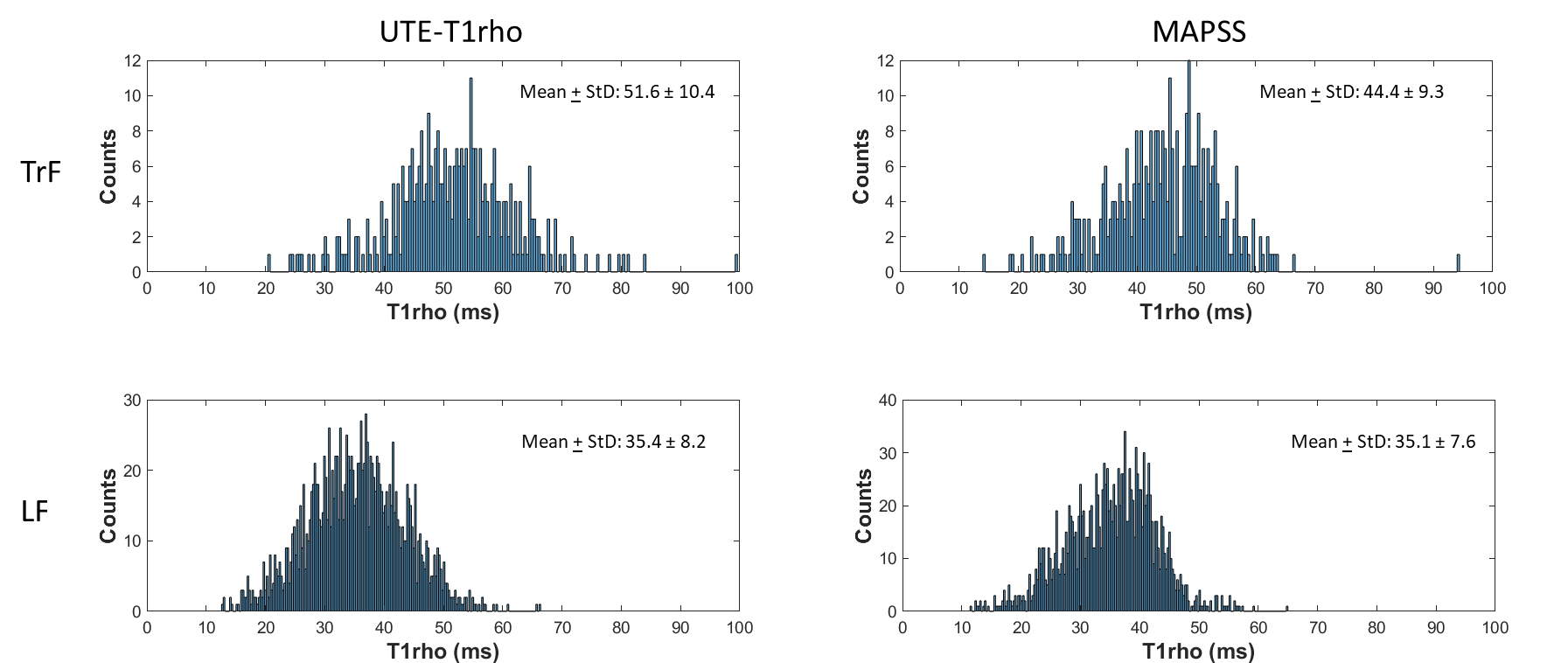
Figure 4.
Histograms of T1ρ data for the lateral femur (LF) and trochlear (TrF) regions. The
mean T1rho values in the TrF region derived from the MAPSS acquisition were
significantly shorter than the corresponding values derived from the UTE acquisition,
even as the distributions were similar.
DOI: https://doi.org/10.58530/2023/2199