2164
Finding Precise, Direct, and Personalized Landmarks of Deep Brain Stimulus Tremor Targeting on Advanced MR imaging1Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 2Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 3Nash Family Center for Advanced Circuit Therapeutics, Ichan School of Medicine at Mount Sinai, New York, NY, United States
Synopsis
Keywords: Quantitative Imaging, Quantitative Susceptibility mapping, Tremor
Deep brain stimulation (DBS) is an efficacious treatment for tremors. The clinical outcome is critically dependent on precisely personalized targeting, yet localization of DBS target remains challenging owing to difficulties in resolving individual thalamic nuclei or dentato-rubro-thalamic (DRT) pathways. Here we investigated retrospectively to identify neurosurgical landmarks of DBS targeting by examining the volume overlap and centroid distance between DBS contacts and DRT delineated from quantitative susceptibility imaging. Our findings show a significantly higher volume overlap of DBS contacts with DRT in the good-response tremor group, showing potential of our approach as a direct and personalized neurosurgical guidance tool.
Introduction
Roughly 10 million Americans and millions worldwide suffer from a tremor disorder such as essential tremor or tremor-dominant Parkinson’s disease.1 The associated disabling aspect of tremors can severely impact a patient’s quality of life,2 and neurosurgical treatment such as Deep Brain Stimulation (DBS) may be an option.3 The outcome is critically dependent on precisely personalized targeting; however, direct visualization of the tremor-reducing target, such as the ventral intermediate nucleus (VIM) or dentato-rubro-thalamic (DRT) tract is a major challenge due to low inter-thalamic nuclei contrast in conventional structural imaging (Fig.1, top row). Recent studies show the potential to delineate the DRT using quantitative susceptibility imaging (QSM) since the DRT regions appear hypointense (dark) due to the diamagnetism of myelin.4,5 Here, we employed QSM to identify the DRT and investigated associations of the amount of overlap as well as the centroid distance between the volume of tissue activated (VTA) with given stimulation settings and DRT regions with DBS clinical outcome.Methods
We studied 8 patients with severe tremor who underwent VIM DBS surgery (age range, 62 – 77 years). Patients were divided into two groups based on their clinical outcome within 1-year post-surgery: moderate-response (4 subjects) and good-response (4 subjects) groups. Preoperative MRI was performed on a 3T MRI scanner (GE Signa Architect, GE Healthcare) using a 3D multiple gradient echo sequence (FOV=256×256×176mm3, TE1/ΔTE/nTE = 4.2/4.9ms/10, TR=53.9ms, FA=15°, 0.5mm-isotropic resolution). QSM was generated by using the MEDI6 and DRT was delineated manually as the hypointense area on QSM (Fig.1, bottom row). Individuals’ VTA regions were estimated using Lead DBS software toolbox with given stimulation settings (i.e. amplitude and contact configuration). Percent volume overlap of the VTA with the respective DRT was calculated as (VTA$$$\bigcap$$$DRT)/VTA×100 (%) and the centroid distance between the VTA and DRT regions was also measured. Student’s t-test was performed to test for significant differences between groups.Results
A significant difference was found between the moderate-response and good-response groups in terms of the percent volume overlap of the VTA with the DRT regions (p<0.001; 15.9±10.1% and 76.6±13.2%, respectively) (Fig.2A). There was also a trend toward significant difference in centroid distance between groups (p=0.06; 1.3±0.4 mm and 0.8±0.2 mm, respectively) (Fig.2B).Discussion
Our study shows that the volume overlap of DBS contacts with the DRT tract in the good-response group is significantly higher than that in the moderate-response group, suggesting that the DRT may serve as imaging markers for DBS targeting and QSM has potential to provide direct visualization of the VIM DBS target. Although our findings are based on small numbers of patients, further studies are warranted to confirm and extend our approach to determine the extent of a clinically safe margin and its reproducibility as a direct and personalized neurosurgical guidance tool.Conclusion
This work presents potential of QSM to identify the DRT pathways known as a tremor-reducing structure, highlighting a better DBS outcome with more VTA volume overlap with the DRT in DBS patients with tremor. Our findings may shed new and needed light on the direct and personalized targeting for neurosurgical guidance.Acknowledgements
No acknowledgement found.References
- Louis ED, Ferreira JJ. How common is the most common adult movement disorder? Update on the worldwide prevalence of essential tremor. Mov Disord 25:534-541, 2010.
- Louis ED, Machado DG. Tremor-related quality of life: A comparison of essential tremor vs. Parkinson’s disease patients. Parkinsonism Relat Disord 21:729-735, 2015.
- Benabid AL, et al. Long-term suppression of tremor by chronic stimulation of the ventral intermediate thalamic nucleus. Lancet 337:403-406, 1991.
- Chung S, et al. MR susceptibility imaging with a short TE (MR-SISET): A clinically feasible technique to resolve thalamic nuclei. AJNR 41:1629-1631, 2020.
- Chung S, et al. Targeting the VIM/DRT for essential tremor using MR susceptibility imaging with short echo time (MR-SISET): a pilot study. ASNR 59th Annual Meeting, 2021.
- http://pre.weill.cornell.edu/mri/pages/qsm.html
Figures
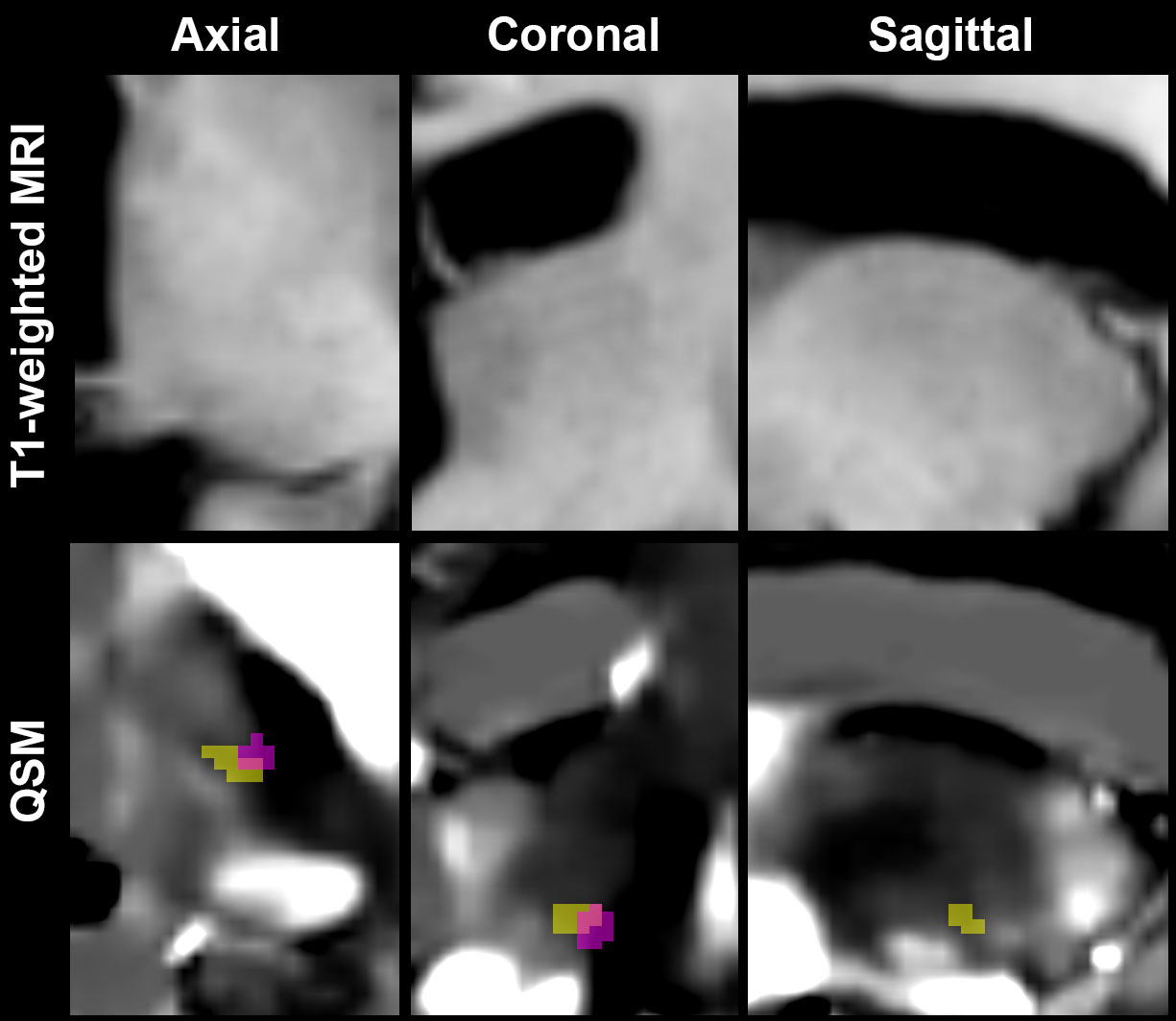
Figure 1. (Top row) Conventional T1-weighted images are shown in axial, coronal, and sagittal planes from left to right. (Bottom row) Images of quantitative susceptibility mapping (QSM) are shown with the estimated dentato-rubro-thalamic (DRT) regions (yellow) and DBS volume of tissue activated (VTA) (red) after VIM-DBS surgery. DRT pathways appear hypointense (dark) on QSM.
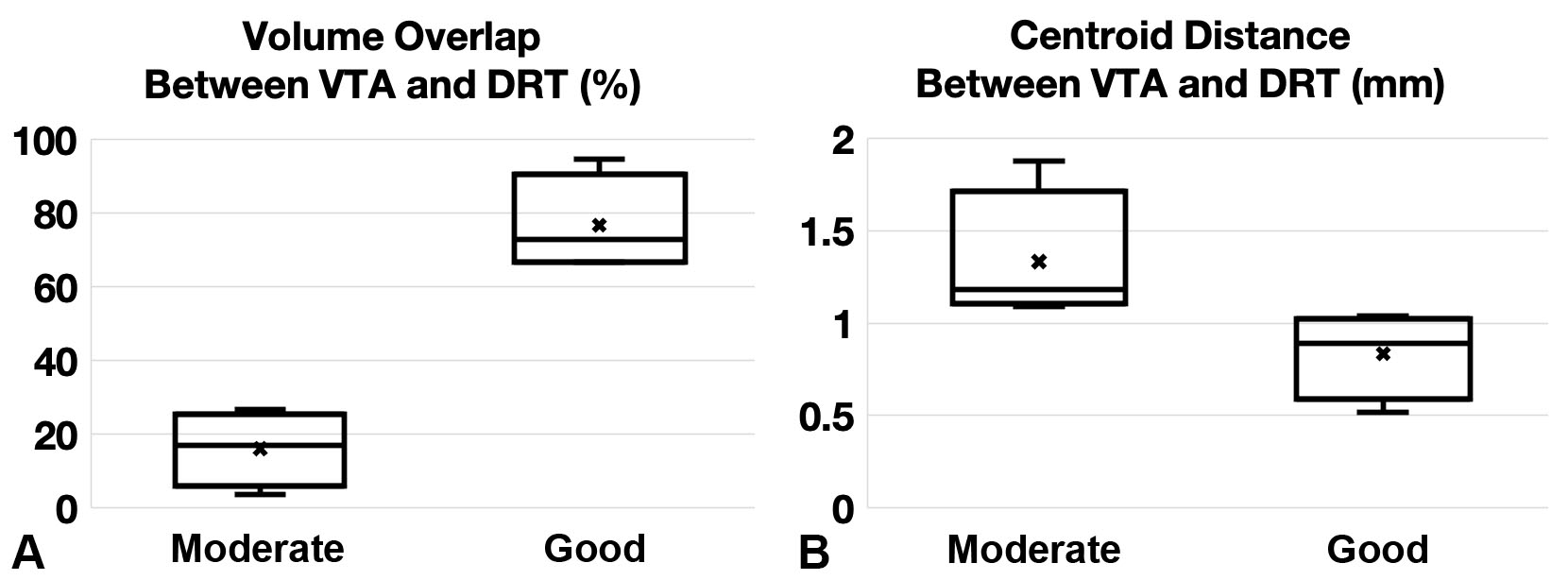
Figure 2. Boxplots show (A) a significant difference in the percent volume overlap of the VTA with the DRT regions between the moderate-response and good-response groups (p<0.001; 15.9±10.1% and 76.6±13.2%, respectively), and (B) a trend toward significance in the centroid distance between VTA and DRT regions (p=0.06; 1.3±0.4mm and 0.8±0.2mm, respectively)