2146
Exploring accelerated MRI based Bone Imaging in Pediatric Congenital Spinal Anomalies
Foram Bharat Gala1, Hirava Manek1, Indrajit Saha2, Narayana Krishna Rolla3, Pradeep Kumar4, and Rashmi Rao3
1Department of Radiology, Bai Jerbai Wadia hospital for children, Mumbai, India, 2Clinical Science, Philips India Limited, Delhi, India, 3Philips India Limited, Bangalore, India, 4Philips India Limited, Mumbai, India
1Department of Radiology, Bai Jerbai Wadia hospital for children, Mumbai, India, 2Clinical Science, Philips India Limited, Delhi, India, 3Philips India Limited, Bangalore, India, 4Philips India Limited, Mumbai, India
Synopsis
Keywords: MSK, Spinal Cord
Congenital spinal anomalies are common in children resulting in spinal deformities and these could be due to isolated vertebral segmentation abnormalities or with added cord abnormalities referred to as spinal dysraphism. Early surgical intervention is necessary in these children which requires both MRI and CT scan evaluation for cord and bone details respectively. We utilized novel technique - Compressed Sense accelerated MRI based - Fast field echo Resembling A CT Using Restricted Echo-spacing (CS-FRACTURE) technique in pediatric patients which provides CT like contrast. We describe our experience in evaluation of congenital spinal anomaliesINTRODUCTION
Congenital spinal anomalies can present in the neonatal period up to early childhood. Many of these anomalies are also associated with cord anomalies which makes MRI an indispensable part of imaging1. Treating these anomalies particularly those with spinal alignment deformities like scoliosis and kyphosis need comprehensive preoperative imaging for obtaining the exact bone and cord details1. While MRI can provide good soft tissue and cord details, a surgeon usually needs a bone model of the spine for preoperative planning, hence CT scan is also indispensable. Scanning pediatric patients is challenging as they need sedation for the period of scanning. Compressed Sense accelerated MRI based - Fast field echoResembling A CT Using Restricted Echo-spacing (CS-FRACTURE) is a novel technique which accentuates bony features and provide images which are visibly comparable to CT contrast2. The use of T1 spoiled gradient echo with ultra-short echo time MRI sequences to obtain CT like bone images has been studied in adult patients with degenerative spine changes3. This is helpful in pediatric patients as it requires a single sedation and prevents the use of ionizing radiation by avoiding CT scan. We describe our experience of this novel sequence in evaluation of congenital spinal abnormalities in children.Materials and Methods:
11 children with spinal anomalies were included prospectively and imaged using both MRI and CT scan. This study was approved by institutional ethical review board and after taking informed consent from the parents. The scans were performed under sedation in those children who were too young to cooperate.Imaging Protocol:
MR imaging was obtained on 1.5T Ingenia (Philips Healthcare, the Netherlands) using pediatric spine coil. CS-FRACTURE sequence was acquired as part of the routine clinical spine protocol. The routinely acquired sequences and their parameters are summarized in Table 1. A compressedSENSE factor of 8 was used to reduce the acquisition time to 3 minutes. CT imaging was performed at a 64 slice scanner with the following protocol parameters: 80 Kv, 130 mAs, 1mm slice thickness utilizing bone specific kernel.Image analysis
The CT scan and MRI images were interpreted independently by a neuroradiologist with ~ 12 years of experience. Images were considered diagnostic when the image quality was such that a confident diagnosis can be made and had either no or minimal artifacts which do not hamper in making a diagnosis.Results
We included 11 patients in this prospective study. This included children with Klippel Fiel anomaly, spinal dysraphisms, dorsolumbar vertebral anomalies and segmental spinal dysgenesis. 1) The first group included 5 children with Klippel Fiel anomaly. They showed complex fusion anomalies along the cervicodorsal vertebrae and their posterior elements.2 children had atlanto-occipital assimilation. 1 child had complete agenesis of atlasm1 had absent posterior archand 1 had asymmetry between two lateral arches of which the left one was oblique and displaced antero-inferiorly. The diagnosis of absent C1 or its elements was more confidently made on CS-FRACTURE MRI as compared to CT as sometimes cartilaginous (non-ossified) arches may be difficult to visualize on CT. 2 patients had basilar invagination and cord compression which was seen on both CS-FRACTURE MRI and CT scan. The extent and level of fusion anomalies along the cervicodorsal spine and associated findings like torticollis, Sprengel’s deformity of shoulder could be made confidently on CS-FRACTURE MRI and were confirmed by CT images. 2) The second group included 4 patients with spinal dysraphism, 2 with lipomyelocele, 1 with lipomyelomeningocele and 1 with combined Pang type 1 diastematomyelia and limited dorsal myeloschisis(LDM). The level and extent of vertebral segmentation anomalies and posterior element defects could be confidently identified on both CS-FRACTURE MRI and CT scan images. The 2 patients with lipomyelocele had subcutaneous lipoma with hamartomatous tissue which showed bone like signal with differentiation of cortex and medulla on MRI however showed soft tissue density on CT images. None of these have been operated yet to have a pathological correlation. The diastematomyelia case showed osseous bar on both CS- FRACTURE MRI and CT scan Images. 3) The third group had vertebral anomalies at dorso-lumbar spine, of which 1 patient had 2 lumbar hemivertebrae with multilevel fusion anomalies and another had dysplastic left sided pedicles from d10-12 along with focal cord hypoplasia suggesting segmental spinal dysgenesis. These findings were well seen on CS-FRACTURE MRI and confirmed on CT images.Discussion
The use of new CS-FRACTURE sequence in pediatric patients is useful in all types of spinal anomalies. In children with vertebral segmentation anomalies, it helps in characterizing the type of vertebral anomaly, localizing the exact level and extent of vertebral fusion/ defect and alignment abnormalities like kyphoscoliosis. Additionally, MRI helps in evaluation of cord abnormalities. Added advantage of fast and robustness of the CS technique and subtraction method involved in the post processing of FRACTURE reduced motion related artifacts hence improving pediatric patient comfort. Thus, with comparable information obtained in CS-FRACTURE sequence on MRI scanner, we can obliviate the need of CT scan and avoid the ionizing radiation.Acknowledgements
No acknowledgement found.References
1. Trenga, A.P., Singla, A., Feger, M.A. et al. Patterns of congenital bony spinal deformity and associated neural anomalies on X-ray and magnetic resonance imaging . J Child Orthop 10, 343–352 (2016). https://doi.org/10.1007/s11832-016-0752-6 2. Johnson B, Alizai H, Dempsey M. Fast field echo resembling a CT using restricted echo-spacing (FRACTURE): a novel MRI technique with superior bone contrast. SkeletalRadiology. 2021 Aug;50(8):1705-1713. DOI: 10.1007/s00256-020-03659-7. PMID: 33175183. 3. Schwaiger, B.J., Schneider, C., Kronthaler, S. et al. CT-like images based on T1 spoiled gradient-echo and ultra-short echo time MRI sequences for the assessment of vertebral fractures and degenerative bone changes of the spine. EurRadiol 31, 4680–4689 (2021). https://doi.org/10.1007/s00330-020-07597-9Figures
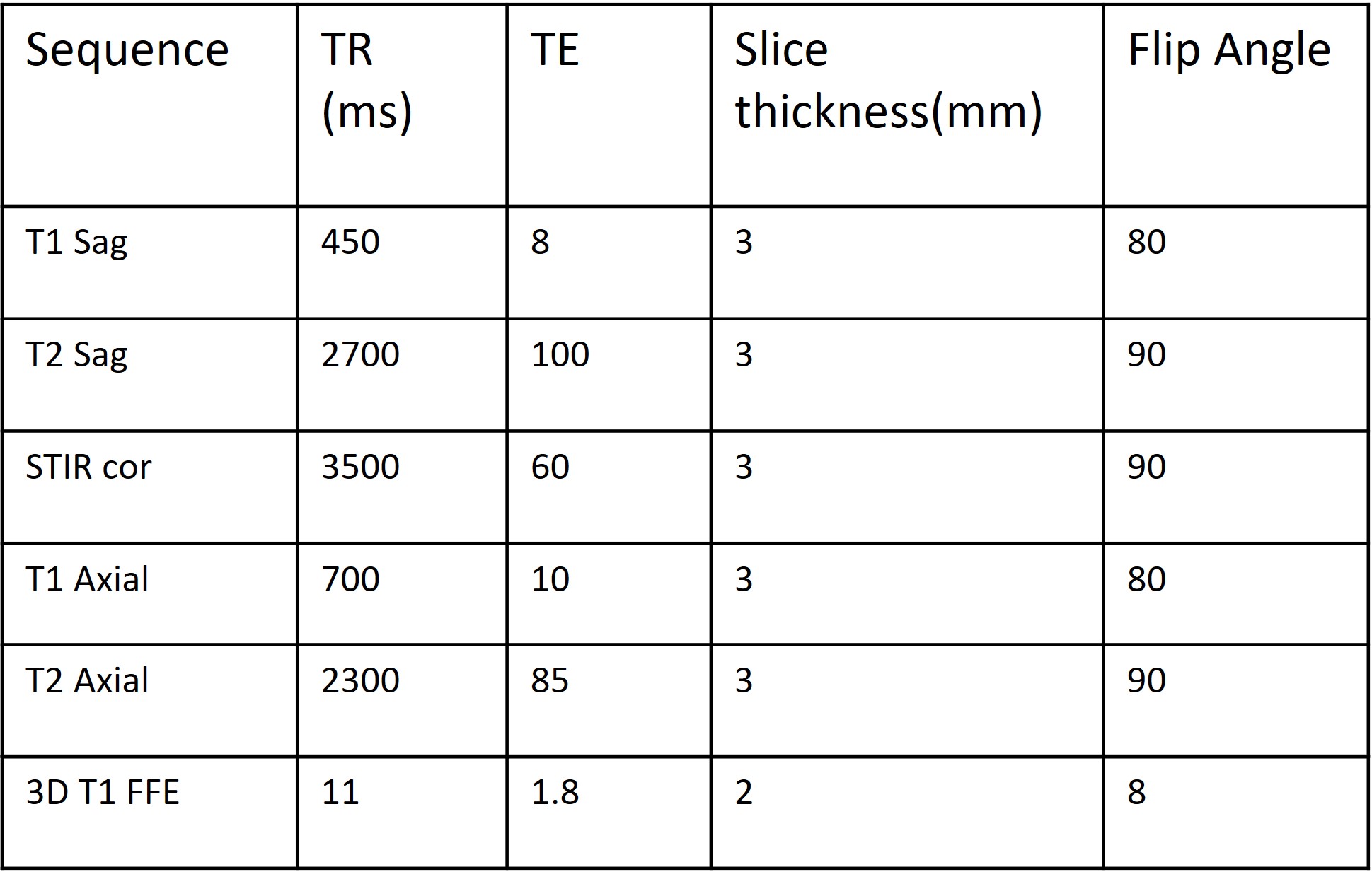
Table 1: Scan parameters of routine pediatric spine protocol along with CS-FRACTURE

Figure 1: CT (bone window images -a) and
corresponding sagittal MRI CS-FRACTURE IMAGES (b) in a 6
year old girl
with Klippel Fiel syndrome showing atlanto-occipital assimilation (black
arrow), basilar invagination, absent posterior spinous processes of C1 and C2
(white arrow), fusion of multiple cervical and dorsal vertebrae with posterior
elements (dotted arrow). Hypoplastic retroflexed dens (bent arrow) effacing
anterior subarachnoid space and indenting the cervico-medullary cord.
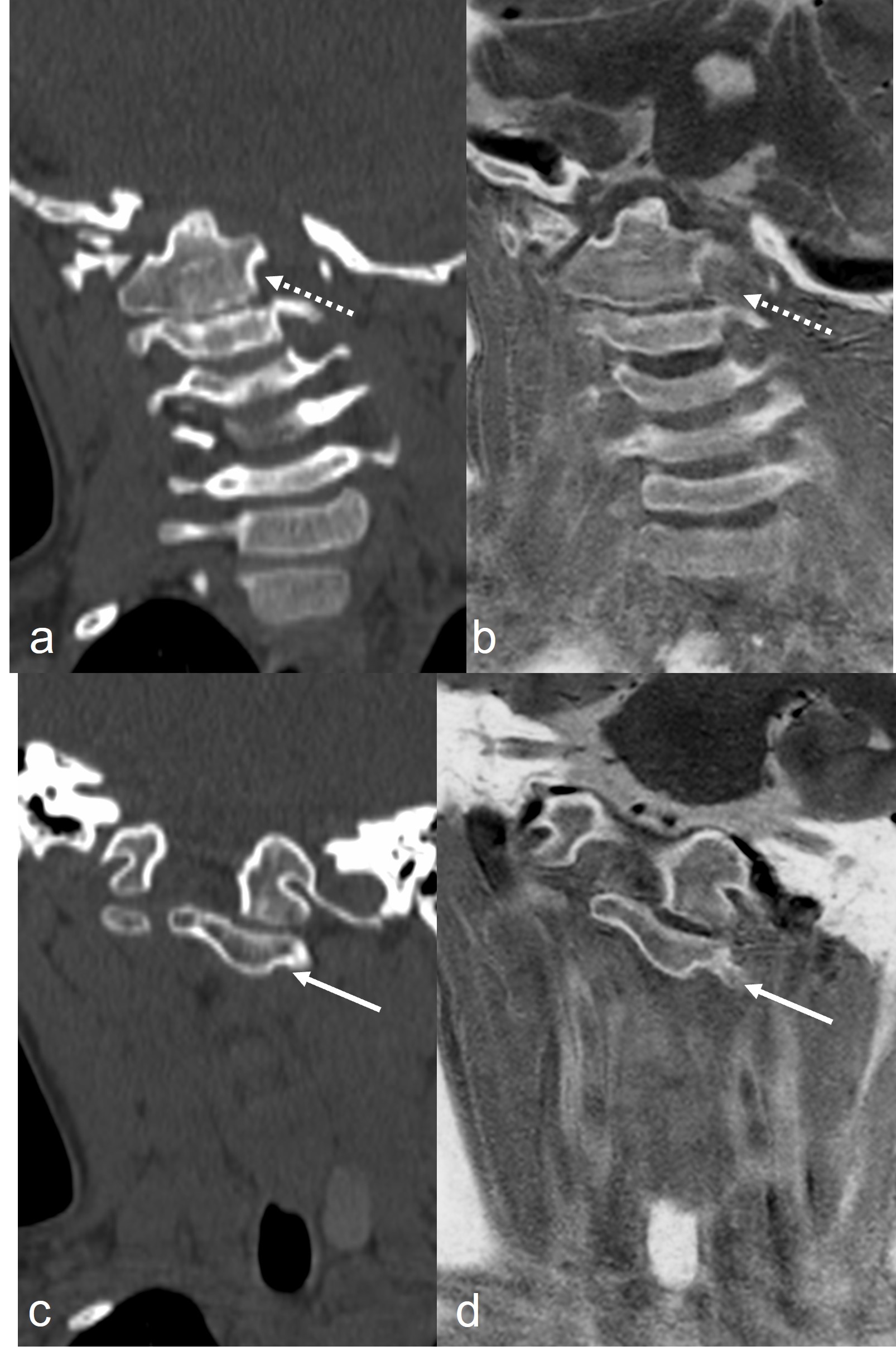
Figure 2: CT (bone window images –a,c) and
corresponding coronal MRI CS-FRACTURE IMAGES (b,d) in a 5 year old girl with Klippel Fiel syndrome shows
antero-inferiorly displaced left lateral arch of C1 (white arrow). Fusion of
C2-3 vertebral bodies (dotted arrow) is also seen. Tilt of head is seen to left
side.
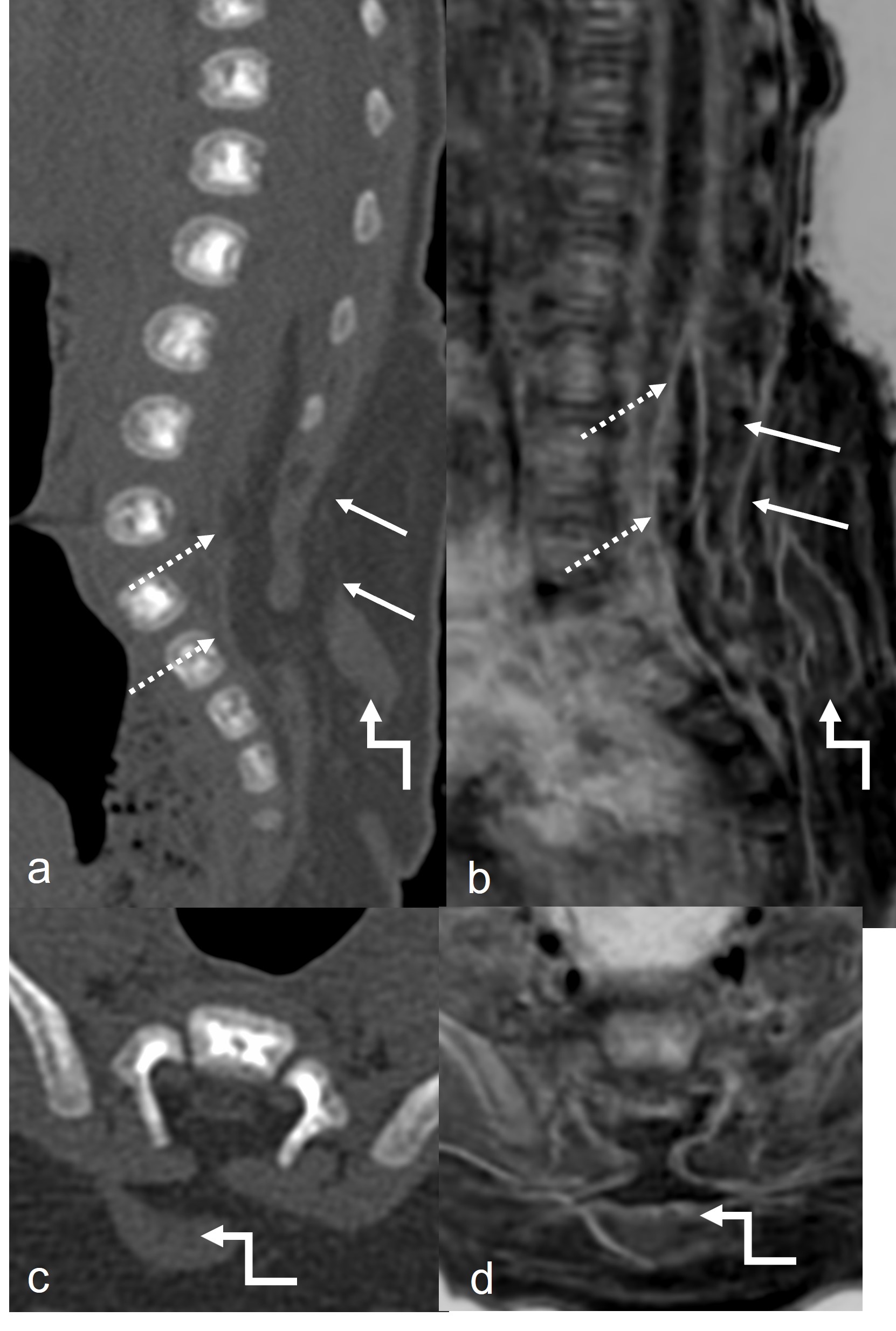
Figure 3: CT (bone window images –a,c) and
corresponding sagittal and axial MRI CS-FRACTURE IMAGES (b,d) in
a 1
month old girl
with subcutaneous swelling over back shows posterior element defects from L4
below ( white arrow), herniation of subcutaneous fat into spinal canal with
neural placode junction in the spinal canal suggesting lipomyelocele (dotted
arrow). Low lying cord is well seen on MRI images . Also note soft tissue
density tissue in subcutaneous lipoma on CT (bent arrow) which appears osseous
on CS-FRACTURE likely to represent osseous dysraphic hamartoma.
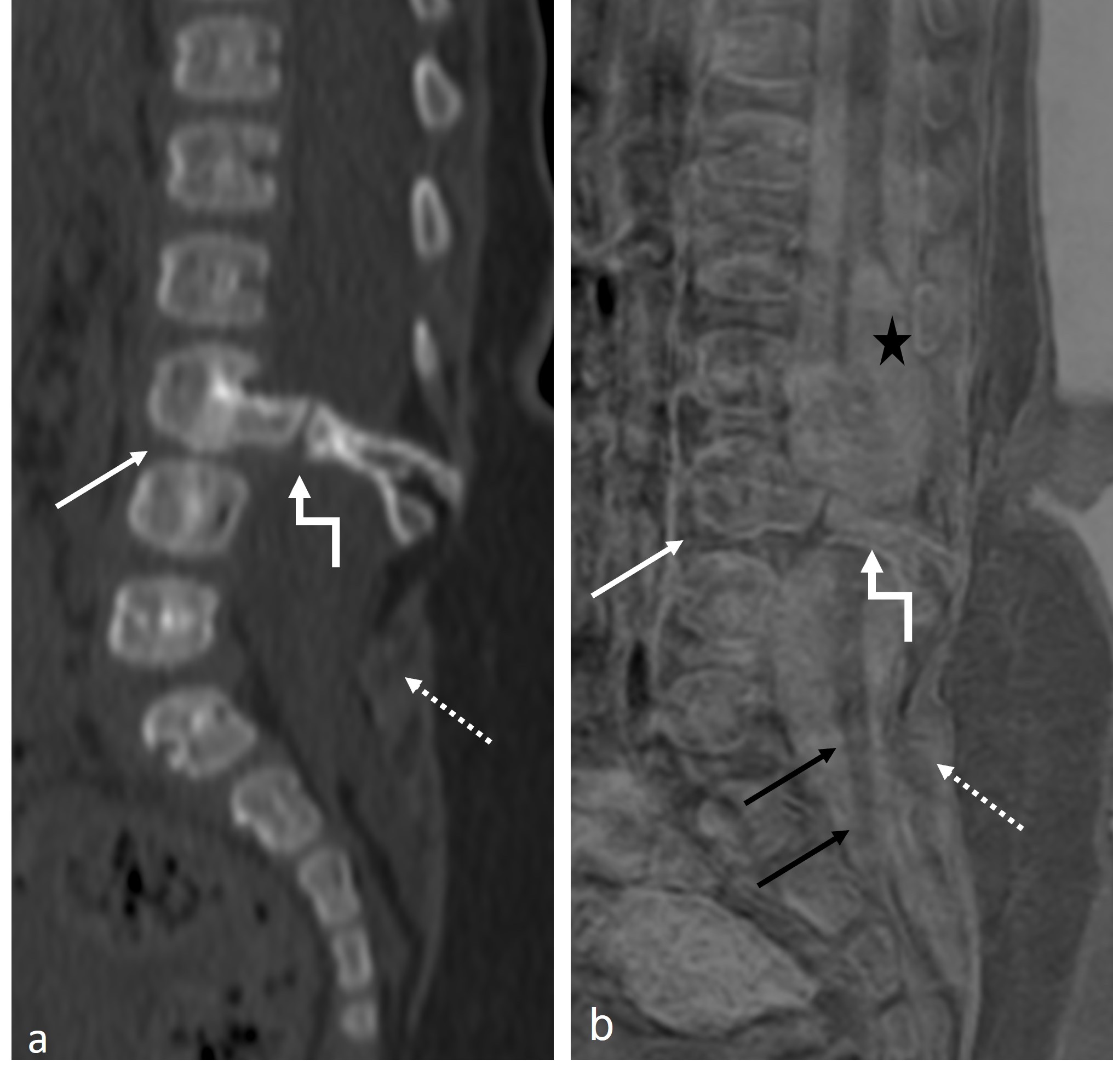
Figure 4: CT (bone window images –a) and
corresponding sagittal MRI CS-FRACTURE IMAGES (b) in a 6
month old girl
with subcutaneous swelling over back, shows partial fusion of L3 and L4
vertebral bodies (white arrow), posterior element defects from L4 below (dotted
arrow). A well
defined
osseous bar (bent arrow)is seen at L3-4 level resulting in hemicords
suggestive of Pang type 1 diastematomyelia. Syrinx (star) and low
lying cord
are well seen on MRI images (black arrow).
DOI: https://doi.org/10.58530/2023/2146