2113
A Preliminary study on evaluation of collateral compensatory by high-resolution CS TOF MRA and 4D flow:Case Series
Yue Ma1, Yueluan Jiang2, Dan Tong1, Zechen Yu3, and Xinpeng Liu1
1Radiology, First Hospital of Jilin University, Changchun of Jilin province, China, 2MR Scientific Marketing, Diagnostic Imaging, Siemens Healthineers Ltd., Beijing, China, 3Siemens Healthineers Digital Technology (Shanghai) Co., Ltd., Changchun of Jilin province, China
1Radiology, First Hospital of Jilin University, Changchun of Jilin province, China, 2MR Scientific Marketing, Diagnostic Imaging, Siemens Healthineers Ltd., Beijing, China, 3Siemens Healthineers Digital Technology (Shanghai) Co., Ltd., Changchun of Jilin province, China
Synopsis
Keywords: Stroke, Blood vessels
Evaluation of hemodynamic and geometric changes of intracranial atherosclerosis and follow-up is of great clinical significance. A comprehensive quantification of the whole collateral recruitment in the circle of Willis (CW) is needed. In this work, we combined High-resolution CS TOF-MRA and 4D Flow MRI to investigate the situation of collateral recruitment. We were able to demonstrate a new way to visual and quantify the cerebrovascular impact of a significant intracranial stenosis and the compensatory mechanism of the collaterals.Synopsis:
Evaluation of hemodynamic and geometric changes of intracranial atherosclerosis and follow-up is of great clinical significance. A comprehensive quantification of the whole collateral recruitment in the circle of Willis (CW) is needed. In this work, we combined High-resolution CS TOF-MRA and 4D Flow MRI to investigate the situation of collateral recruitment. We were able to demonstrate a new way to visual and quantify the cerebrovascular impact of a significant intracranial stenosis and the compensatory mechanism of the collaterals.Introduction:
Collateral compensatory assessment remains challenging due to the small size of vessels and digital subtraction angiography (DSA) is the gold standard. However, as an invasive and ionizing radiation imaging technology, DSA is unsuited for repeated imaging or research-oriented studies. Time-of-Flight magnetic resonance angiography (TOF-MRA) has been widely used in intracranial artery visualization, which is a non-invasive and bright-blood visualization with superior vessel to tissue contrast [1]. However, it has limitations in the visualization of small and distal arterial branches because of limited spatial resolution within the clinical- acceptable scanning time. Compressed sensing (CS) allows rapid acquisition of images by using undersampling of the k-space to accelerate scan[2]. 4D Flow MRI, a new tool for investigating the collaterals through quantify blood flow rates (BFRs) in individual cerebral arteries has been presented in recent study[3]. Therefore, we aimed to study the feasibility and clinical utility of CS TOF-MRA and 4D Flow MRI for assessment of collateral circulation which may dramatically preserve cerebral perfusion in intracranial atherosclerosis.Materials and methods:
Three intracranial stenosis patients enrolled in this study, they underwent conventional TOF MRA, CS TOF-MRA,4D Flow examinations on a 3T MRI system (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany) with a 20-channel head coil. CS-TOF MRA parameters are shown as follows: slice orientation axial, FOV=220*220mm2, resolution=383*326, 175slices, voxel size=0.4*0.4*0.4mm3, CS acceleration factor=4.4. Conventional parallel acceleration TOF MRA set the same parameters of FOV, resolution slice thickness as CS-TOF MRA.4D Flow MRI parameters were as follows: voxel size=0.8*0.8*1.5mm3, FOV=180*100mm2, slice thickness=1.5mm, 104 slices, TR=50.4ms, TE=3.71ms,venc=120. The total acquisition time was 20 minutes and 34 seconds. Flow analysis was performed in Circle Cardiovascular Imaging CVI42 software for calculating BFRs in milliliters per minute. The average velocity (Vavg), maximum velocity (Vmax), average blood flow (Flowavg), and pulsatility index (PI) of the proximal and distal stenosis segments were calculated. MIP images and source images of CS TOF-MRA were used for imaging evaluation. Images were assessed independently in a randomized order by two neuroradiologists.Results:
Figure1 and Figure2 show representative MIP images acquired with conventional TOF-MRA and CS TOF-MRA. Scan coverage was increased in CS TOF-MRA with a prominent shorter scan time compared to conventional TOF-MRA (approximately 3 minutes vs. 6 minutes).SNR and CNR of the vessels in both conventional TOF MRA and CS TOF MRA were calculated in figure 2, The vessel CNR between vessel and background and SNR of vessel in CS TOF-MRA groups is higher than that in conventional TOF MRA(CNR: 26.79 vs 28.22 ; SNR 7.43 vs 22.187).Figure 3 show the image quality and diagnostic performance of high-resolution CS TOF-MRA in a patient with mild stenosis of the left middle cerebral artery follow-up original images. Figure 4 summarized the sum BFRs of ACA2, MCA, and PCA1 was lower on the ipsilateral(11.430mL/min) than on the contralateral(13.278mL/min). The severe stenosis showed significantly higher Vavg(9.098 vs 6.707 cm/s), Vmax(19.236 vs 9.804 cm/s), and PI(1.003 vs 0.816 mmHg) than the mild one,The results showed that the pressure gradient was different in patients with moderate to severe middle cerebral artery stenosis.The combined protocol provides a detailed depiction of the vascular architecture and dynamic blood flow pattern with high spatial and temporal resolutions, allowing the visualization of focus arteries.Discussion:
In this study, the scan time of CS TOF-MRA for achieving a high-resolution spatial resolution (0.4 × 0.4 × 0.4 mm3) was 3 minutes and 7 seconds. We observed that CS TOF-MRA with an acceleration factor of 4.4 provided better quality images in lesion sites and small and distal arterial branches without significantly sacrificing image quality while reducing nearly half the scan time compared with conventinal parallel acceleration TOF_MRA.The Iso-Voxel CS TOF-MRA allows detailed characterization of small perforating arteries which benefit from advances in parallel imaging technologies. Similar to some study research, we found not local intracranial stenosis only changes the flow of the distal stenosis artery, but also significantly affects the ipsilateral side collateral circulation[4]. Previous imaging studies on vascular morphology have provided important clinical information. In our study, the severe stenosis showed significantly higher BFRs in the stenosis side of the the circle of Willis than the mild one,demonstrate collateral circulation to fully establish (increase in number and diameter) and exert better compensatory capacity. The evaluation of arterial blood flow dynamics may provide information on vascular function and lay a foundation for the comprehensive assessment of collateral circulation.Conclusion:
This is preliminary study explored a set of possible qualitative and quantitative methods for collateral recruitment in the circle of Willis. The proposed CS TOF-MRA and 4D flow protocol provides a detailed depiction of the vascular architecture and dynamic blood flow pattern with high spatial and temporal resolutions, allowing the visualization of focus arteries.Acknowledgements
No acknowledgement found.References
[1]Jindal G, Miller T, Raghavan P, Gandhi D. Imaging evaluation and treatment of vascular lesions at the skull base. Radiol Clin North Am 2017; 55: 151– 166. [2]Cho SJ, Choi YJ, Chung SR, et al. High-resolution MRI using compressed sensing-sensitivity encoding (CS-SENSE) for patients with suspected neurovascular compression syndrome: comparison with the conventional SENSE parallel acquisition technique. Clin Radiol 2019;74:817.e9-817.e14[3]Zarrinkoob L, Wåhlin A, Ambarki K, Birgander R, Eklund A, Malm J. Blood Flow Lateralization and Collateral Compensatory Mechanisms in Patients With Carotid Artery Stenosis. Stroke. 2019 May;50(5):1081-1088. doi: 10.1161/STROKEAHA.119.024757. PMID: 30943887; PMCID: PMC6485302.[4] Wu C, Schnell S, Vakil P, et al. In vivo assessment of the impact of regional intracranial atherosclerotic lesions on brain arterial 3D hemodynamics[J]. AJNR Am J Neuroradiol, 2017, 38(3): 515‑522. DOI: 10.3174/ajnr.A5051.Figures
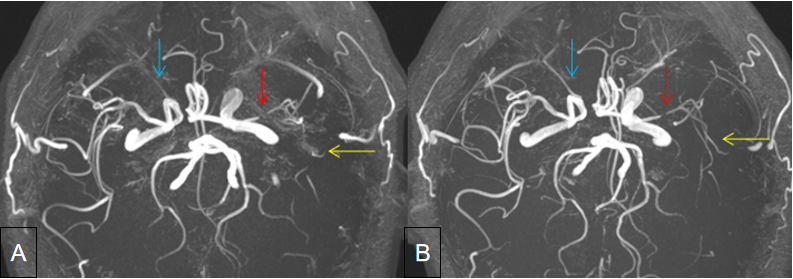
Figure 1. A conventional TOF-MRAand BCS TOF-MRA) . 54-year-old male patient with left middle cerebral artery (MCA 1) stenosis had acute stroke and TOF-MRA images show site of atherosclerosis nearly occlusion (red arrowhead). The CS TOF-MRA shows the distal arterial branches (yellow arrowhead) and ophthalmic arteries (blue arrowhead), which is considered closed or not clearly displayed on conventional TOF-MRA . Note the increased background noise on conventional TOF-MRA.
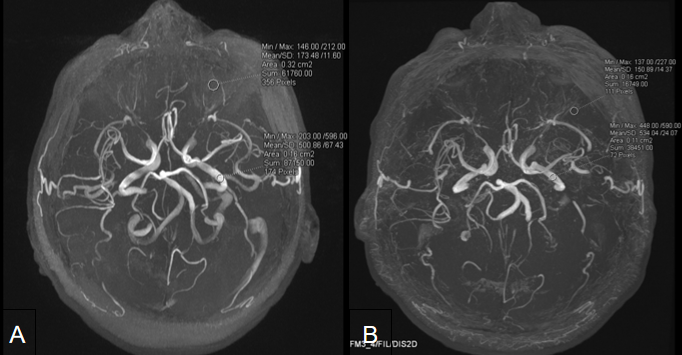
Figure 2.Comparison of conventional TOF-MRA(A) and CS TOF-MRA(B) images are shown. For each subject, two ROI with equal area were manually delineated on the MIP images. ROI 1 was placed within the arterial vessel area, and ROI 2 was placed at the background where no vessels passed by.
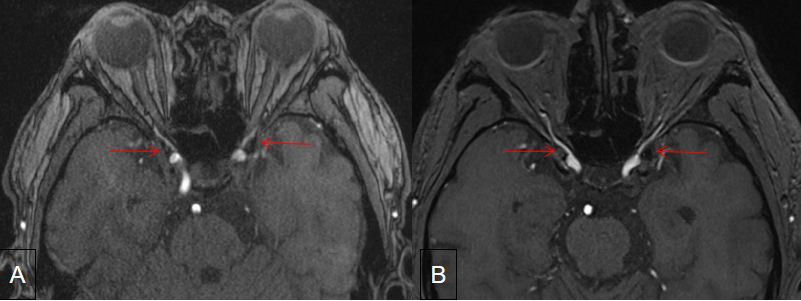
Figure 3. On the axial image, 65-year-old male patient with mild stenosis in the left middle cerebral artery (MCA 1).CS TOF-MRA(B) showed better noise reduction compared to conventional images clinical use. Red arrows indicate that the edge of vessel wall characteristics artifact, which was diminished in the CS TOF-MRA.
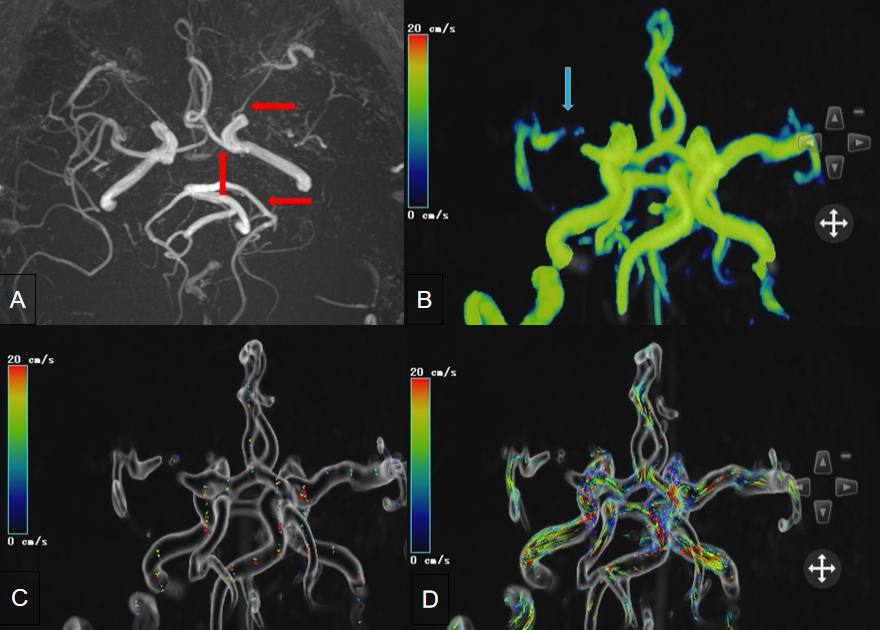
Figure 4.A 65-year-old female patient with nearly completely occlusion of the left middle cerebral artery(blue arrowhead).CS TOF-MRA(A) showed mild larger diameter of anterior cerebral artery(ACA), ophthalmic artery and posterior cerebral artery(PCA) than the contralateral ones(red arrowhead).Velocity(B) demonstrated Vavg, Vmax, Flowavg within the circle of Willis ;Vectory (C) and Pathline(Mask)(D)had a reversed BFR in the contralateral ACA,PCA,MCA.
DOI: https://doi.org/10.58530/2023/2113