2108
Artificial Intelligence-Driven Image Quality Assessment for Intracranial Vessel Wall Magnetic Resonance Imaging
Wenjia Peng1, Haiyan Zhao1, Xuefeng Zhang1, Luguang Chen1, Hao Li2, Shuo Wang2, and Jianping Lu1
1The First Affiliated Hospital of Naval Medical University, Shanghai, China, 2Fudan University, Shanghai, China
1The First Affiliated Hospital of Naval Medical University, Shanghai, China, 2Fudan University, Shanghai, China
Synopsis
Keywords: Stroke, Stroke, vessel wall imaging
Image quality control is a prerequisite for quantitative image analysis. We develop a convolutional neural network-based model for assessing the image quality of intracranial vessel wall MRI. Experimental results show that the model prediction is in good agreement with a senior radiologist, with a Cohen’s Kappa of 0.689. The model demonstrates real-time evaluation speed which is 500 times faster than the radiologist. It has the potential to be used in performing quality control on historical data for research purposes, and also can be used to examine the image quality immediately after the clinical MRI scan.Introduction
Intracranial atherosclerotic disease is a major cause of ischemic stroke, accounting for 70% of all stroke cases in China. Higher-resolution magnetic resonance imaging (hr-MRI) of the intracranial vessel wall (IVW) provides rich information about plaque morphology and composition. Previous studies have shown that image features (e.g., intraplaque haemorrhage, vessel wall remodelling, plaque enhancement) derived from hr-MRI provide complementary information to assess plaque vulnerability in addition to the degree of stenosis.Recently, the advancement of machine learning enables the investigation of more complex radiomics features (e.g., histogram, texture), improving diagnostic and prognostic accuracy [1]. However, the calculation of such high-order image features is sensitive to the grayscale intensity and therefore, susceptible to the artifacts. Image quality control is a prerequisite for quantitative analysis of hr-MRI images in clinical routine, while the standard of image quality assessment (IQA) on IVW hr-MRI has not been established. The assessment usually depends on the radiologist’s experience which is subjective and time-consuming. The global image metrics such as signal-to-noise ratio (SNR) may not reflect the imaging quality of the localized plaque. Therefore, an automated system which provides a rapid and accurate IQA of different regions of the intracranial arteries is highly demanded.
Method
We retrospectively included 500 patients who underwent intracranial vessel wall imaging between January 2013 and December 2018. The hr-MRI was performed using a 3T whole-body MRI system (Skyra, Siemens Healthcare, Germany) with a 20-channel head/neck coil. Three-dimensional IVW imaging was acquired in the sagittal plane using spatial and chemical-shift encoded excitation (SPACE) sequence. The protocol and parameters of image acquisition were reported in previous studies [2]. We extract the post-contrast T1-weighted images for the image quality assessment study. The 500 images were randomly split into training (60%, 300 images), validation (20%, 100 images), and test (20%, 100 images) sets.For each image volume, the image quality was assessed by a senior radiologist (WP; more than 10 years of experience) for the seven segments of intracranial arteries, including the left and right internal carotid arteries (L-ICA and R-ICA), the M1 segments of the left and right middle cerebral arteries (L-MCA and R-MCA), the V4 segments of left and right vertebral artery (L-VA and R-VA), and the basilar artery (BA). A 4-point Likert scale was used for the subjective IQA, as demonstrated in Figure 1. The seven segments of interest were also annotated by placing a bounding box in Horos (Horos Imaging Software v3.3.6).
As shown in Figure 2, a convolutional neural network for image quality assessment (IQA-CNN) using the ResNet [3] backbone was trained to regress the subjective image score. The network was pre-trained on the ImageNet. The two-dimensional image cropped by the bounding box was the input to the IQA-CNN, while the output was the subjective score that was scaled to a 1 - 5 range and transformed into a discrete 5-point scale. The detailed CNN architecture is demonstrated in Figure 3.
The system performance was evaluated using the test set. Agreement among the quality scores was analyzed by using Cohen’s Kappa test and Kappa values were interpreted as follows: 0.00-0.20, poor agreement; 0.21-0.40, fair agreement; 0.41-0.60, moderate agreement; 0.61-0.80, substantial agreement; and 0.80-1.00, almost perfect agreement.
Result and Discussion
The agreement between the scores predicted by the IQA-CNN and the senior radiologist is shown in Figure 4 and Figure 5. The results showed a substantial agreement of scores between the IQA-CNN and the radiologist, with a kappa of 0.689. The agreement on rating the ICA was the highest, with a kappa of 0.772. The assessment speed of the radiologist and the IQA-CNN were also evaluated. In comparison, the evaluation time by IQA-CNN (0.08s per segment) is over 500 times faster than the manual assessment (4s per segment).One limitation of this study is that the intracranial artery segments were manually annotated, which makes the method semi-automatic. We are developing a CNN-based objective detection model to perform the automatic localization of the seven segments, so that the system will work end-to-end. The inter-radiologist agreement should be assessed as a reference to evaluate the performance of the IQA-CNN in the next studies. Also, the assessment criteria should be extended for the assessment of flow artifacts which occur frequently in clinical scans and have an influence on the downstream quantitative analysis.
The potential use of the automated IQA system is two-fold. On one hand, the IQA system can be used to score the images stored in the database and to perform quality control for selecting good-quality images for quantitative image analysis. On the other hand, the real-time speed of the automated system allows IQA immediately after the clinical MRI scan. This enables to feedback the technician and arrange the second scan in time if the quality control fails, reducing the patient waiting time and the re-injection of contrast.
Conclusion
We developed an artificial intelligence-driven system for the image quality assessment of intracranial vessel wall magnetic resonance imaging. The CNN models demonstrated good agreement with the radiologist with a much faster speed.Acknowledgements
This work is supported by the Medical Innovation Research Special Project of Shanghai Science and Technology Commission (22Y11911200) and Natural Science Foundation of Shanghai (22ZR1478100). Shuo Wang is supported by Shanghai Sailing Programs of Shanghai Municipal Science and Technology Committee (22YF1409300).References
[1] Shi Z, Li J, Zhao M, Peng W, Meddings Z, Jiang T, Liu Q, Teng Z, Lu J. Quantitative histogram analysis on intracranial atherosclerotic plaques: a high-resolution magnetic resonance imaging study. Stroke. 2020;51(7):2161-9.
[2] Tian X, Tian B, Shi Z, Wu X, Peng W, Zhang X, Malhotra A, Mossa‐Basha M, Sekhar L, Liu Q, Lu J. Assessment of intracranial atherosclerotic plaques using 3D black‐blood MRI: Comparison with 3D time‐of‐flight MRA and DSA. Journal of Magnetic Resonance Imaging. 2021;53(2):469-78.
[3] He K, Zhang X, Ren S, Sun J. Deep residual learning for image recognition. In Proceedings of the IEEE conference on computer vision and pattern recognition 2016 (pp. 770-778).
Figures
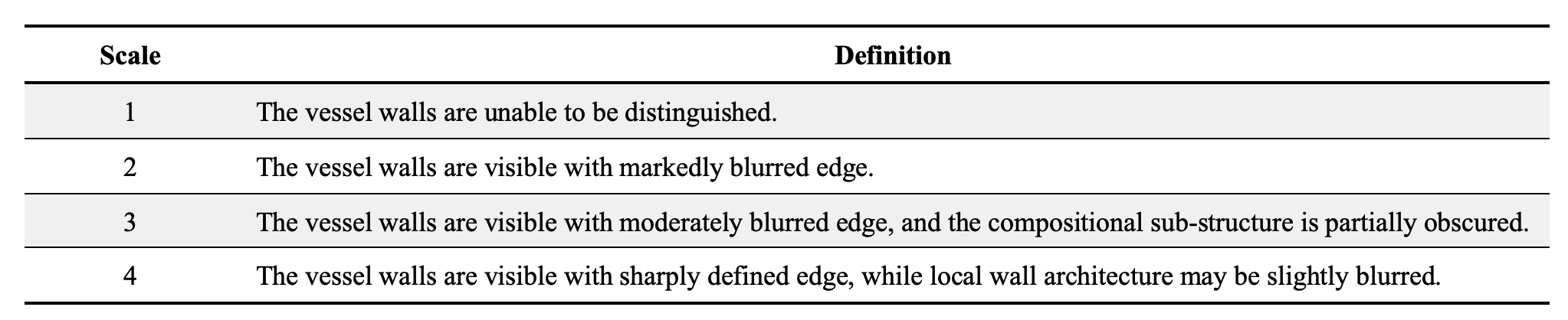
Figure 1 Definition of the 4-point Likert scale for vessel wall image quality assessment.
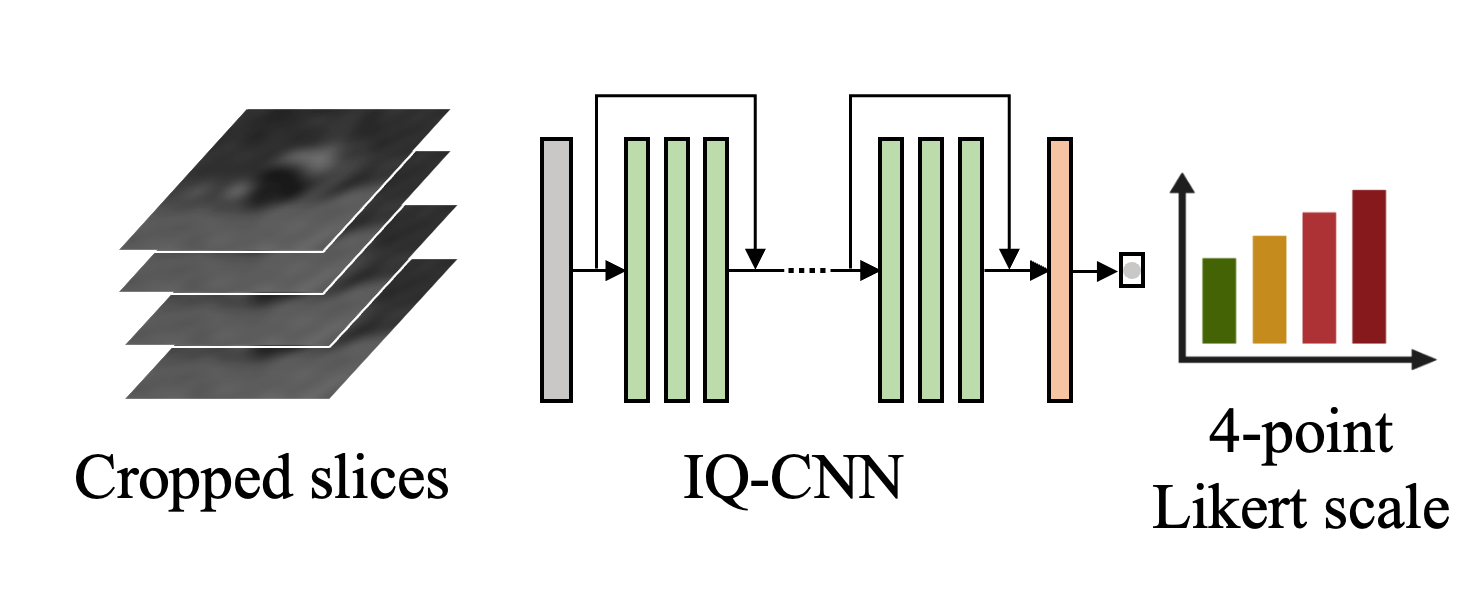
Figure 2 Pipeline of the image quality assessment model. The convolutional neural network takes the cropped image slice as the input and predicts the subjective image quality score.
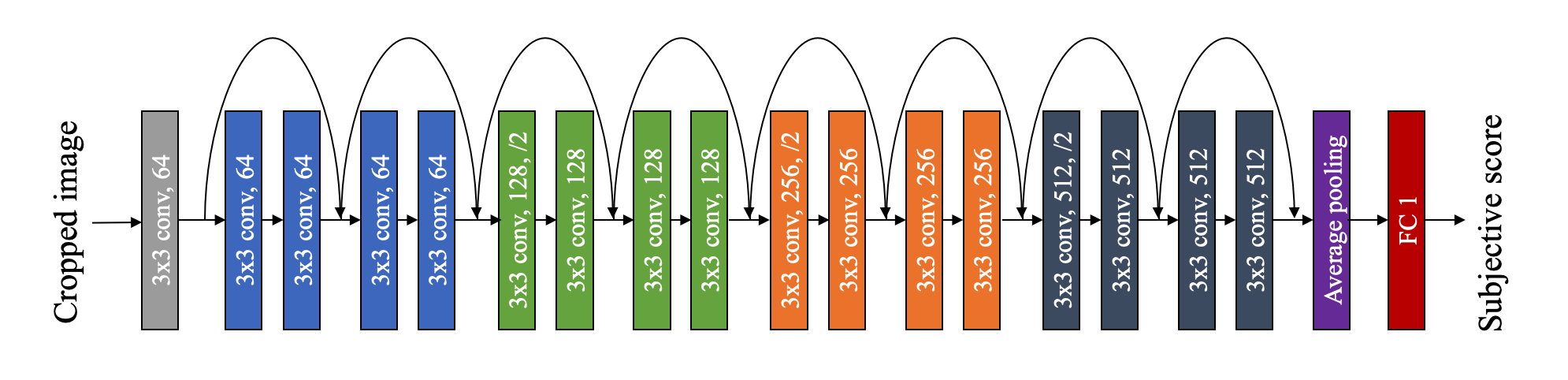
Figure 3 Architecture of the convolutional neural network for image quality assessment.
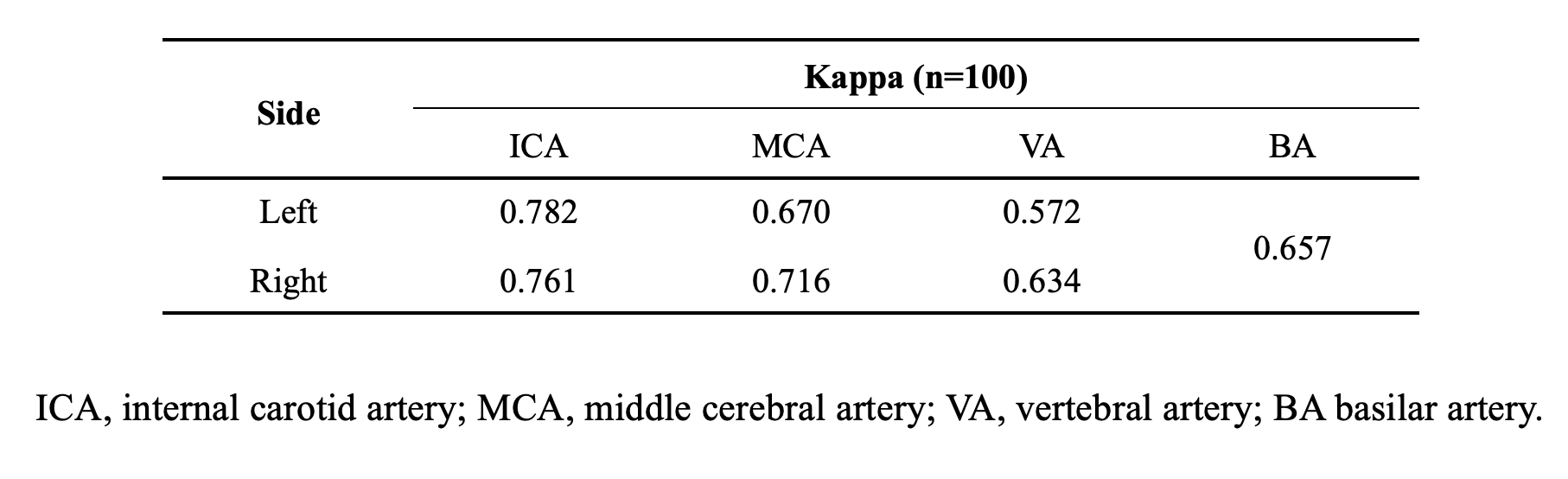
Figure 4 Image quality assessment agreement between the radiologist and IQA-CNN.
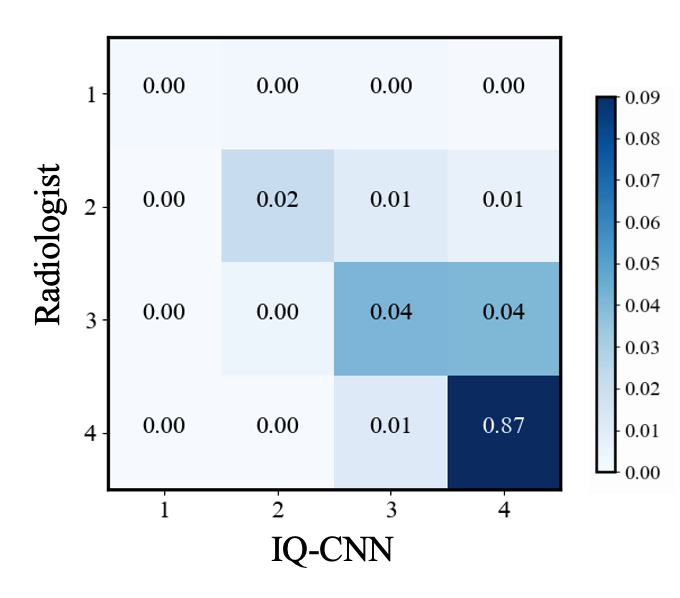
Figure 5 Confusion matrix analysis of the agreement between the radiologist and IQA-CNN.
DOI: https://doi.org/10.58530/2023/2108