2083
Application of slice-accelerated one-minute TGSE-BLADE DWI in clinical practices1Department of Diagnostic Imaging and Nuclear Medicine, Graduate School of Medicine, Kyoto University, Kyoto, Japan, 2Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China
Synopsis
Keywords: Stroke, Artifacts
TGSE-BLADE DWI has been reported to reduce geometric distortion and susceptibility artifacts, however the long acquisition time prevent its clinical application. We reduced acquisition time to 1 minute for TGSE-BLADE DWI using slice acceleration (1-min TGSE-BLADE DWI). We compared distortion and artifacts between SS-EPI DWI and 1-min TGSE-BLADE DWI, and evaluated diagnostic performance for acute infarctions of 1-min TGSE-BLADE DWI. The result shows that the 1-min TGSE-BLADE-DWI has better quality image in terms of distortion and artifacts, and higher diagnostic performance for acute infarctions. TGSE-BLADE DWI with slices acceleration is a promising method for evaluating lesions in acute stroke patients.INTRODUCTION:
Single-shot echo planar imaging based diffusion-weighted imaging (SS-EPI DWI) is prone to susceptibility artifacts in an inhomogeneous magnetic field. The 2D turbo gradient- and spin-echo diffusion-weighted imaging with non-Cartesian BLADE trajectory (TGSE-BLADE DWI) is insensitive to B0 inhomogeneity related effects, leading to reduction of geometric distortion and susceptibility artifacts.1 Several reports showed clinical usefulness of TGSE-BLADE DWI,2-5 however, the long acquisition time prevents its clinical application. To overcome this shortcoming, we applied simultaneous multi-slice (SMS) acceleration technique in TGSE-BLADE DWI. Slice acceleration can be used to reduce scan time and achieve higher resolution6, and has been widely used in many applications. In this study, we achieved to reduce the acquisition time of TGSE-BLADE-DWI to 1 minute, by employing slice acceleration technique. The purpose of this study was to compare the distortion and the artifacts between the SS-EPI DWI and the 1-min TGSE-BLADE DWI, and to evaluate diagnostic performance for acute infarctions in 1-min TGSE-BLADE DWI.METHODS:
SubjectsPatients with acute brain infarction or suspected brain infarction, or patients with post-operative state for a brain tumor within a few days (mean age 66.9, range 18-93 years) were enrolled in this institutional review board-approved study. Written informed consent was provided by these patients.
Image Acquisition
The two DWI sequences (SS-EPI and a prototype 1-min TGSE-BLADE) and T2-weighted imaging (T2WI) sequence for brain were performed using 3T-MR systems (MAGNETOM Skyra or MAGNETOM Prisma; Siemens Healthineers, Erlangen, Germany) with a 32-channel head coil or a 64-channel head/neck coil. The detailed imaging parameters are shown in Figure 1.
Image Analysis
The distortion was quantitatively examined by measuring the displacement between T2WI sequence and each DWI sequence in three parts of brain: frontal lobe near frontal sinus, temporal tip, and pons. Geometric distortion, susceptibility artifacts, and overall image quality were assessed qualitatively using a 4-point Likert scale (1, poor; 2, fair; 3, good; 4, excellent). In patients who had high signal intensities on a trace-weighted image, lesion conspicuity and diagnostic confidence were assessed using a 4-point Likert scale2.
Regions-of-interest (ROIs) were placed on high signal intensity lesions, centrum semiovale (CS) and the pons in the ADC maps. Signal-to-noise ratio (SNR) was calculated as SNRcs = SIcs / SDcs and SNRpons = SIpons / SDpons in all patients, and the contrast-to-noise ratio (CNR) was calculated as CNR = (SIlesion - SIcs) / SDcs in patients with high signal intensity lesions.
Statistical Analysis
The lengths and scores were compared between SS-EPI DWI and 1-min TGSE-BLADE DWI using Wilcoxon signed-rank test. SNR and CNR were compared among them using paired t-test because a dataset of them follows a normal distribution. P value less than 0.05 was considered statistically significant. Statistical analysis was performed using MedCalc version 20.111.
RESULTS:
Out of 62 patients with acute cerebral infarction or suspected cerebral infarction, abnormal high signal intensities suggesting acute or subacute cerebral infarctions were detected in 29 patients (Figure 2), and in the remaining 33 patients, no abnormal high signal intensity was detected. Nineteen patients who had undergone surgery within a few days before brain MRI were also enrolled, and high signal intensity lesions suspected of postoperative changes or acute infarctions were evaluated on DWI (Figure 3). Six patients had acute or subacute infarctions that were detectable only in 1-min TGSE-BLADE DWI, but not in SS-EPI DWI. No lesion was detectable only in SS-EPI DWI.The distortion in frontal lobe, temporal tip, pons was statistically less in 1-min TGSE-BLADE DWI than in SS-EPI DWI (P<0.0001) (Figure 4). The scores for geometric distortion, susceptibility artifacts, overall image quality were better in 1-min TGSE-BLADE DWI than SS-EPI (P<0.0001). The scores for lesion conspicuity and diagnostic confidence were better in 1-min TGSE-BLADE DWI than in SS-EPI DWI (P<0.0001) (Figure 5).
SNR was lower in 1-min TGSE-BLADE DWI (15.5 ± 3.2) than in SS-EPI DWI (16.9 ± 4.8) in CS (P=0.001). However, no statistical differences were observed in SNR of the pons (SS-EPI DWI, 6.0 ± 1.9; TGSE-BLADE DWI, 5.6 ± 1.2) and CNR (SS-EPI DWI, 11.8 ± 5.0; TGSE-BLADE DWI, 12.2 ± 4.7).
DISCUSSION:
The distortion was significantly less in TGSE-BLADE-DWI near the air-bone interfaces (e.g., frontal lobe, temporal tip, and pons), which is consistent with previous reports of TGSE-BLADE DWI without slice acceleration.5 A few acute infarctions were detected only in 1-min TGSE-BLADE DWI; however, no lesions were detectable only in SS-EPI DWI. The scores for lesion conspicuity and diagnostic confidence were better in TGSE-BLADE DWI. These results suggest that TGSE-BLADE DWI using slice acceleration is a promising method that has a good image quality and less artifacts, and more useful for diagnosis of acute infarctions in clinical practices.SNR for TGSE-BLADE DWI was slightly lower than SS-EPI DWI in CS, however, had no statistical differences in pons. Despite this disadvantage of 1-min TGSE-BLADE DWI in SNR, its ability to detect lesions near susceptibility artifacts is a strong advantage.
CONCLUSION:
TGSE-BLADE DWI using slice acceleration has better image quality regarding distortion and artifacts than SS-EPI DWI, and higher diagnostic performance for acute infarctions. The acquisition time of 1 minute is clinically acceptable in evaluation of acute stroke and postoperative complications.Acknowledgements
We are grateful to Mr. Yuta Urushibata, Siemens Healthineers Japan, for their useful comments on this study.References
1. Hu HH, McAllister AS, Jin N, et al. Comparison of 2D BLADE Turbo Gradient- and Spin-Echo and 2D Spin-Echo Echo-Planar Diffusion-Weighted Brain MRI at 3 T: Preliminary Experience in Children. Acad Radiol 2019; 26(12): 1597-604.
2. Fu Q, Kong XC, Liu DX, et al. Clinical comparison of single-shot EPI, readout-segmented EPI and TGSE-BLADE for diffusion-weighted imaging of cerebellopontine angle tumors on 3 tesla. Magn Reson Imaging 2021; 84: 76-83.
3. Geng Y, Shi Y, Chen W, et al. BLADE turbo gradient- and spin-echo in the assessment of sinonasal lesions: a comprehensive comparison of image quality in readout-segmented echo-planar imaging. Acta Radiol 2021: 2841851211041820.
4. Sheng Y, Hong R, Sha Y, Zhang Z, Zhou K, Fu C. Performance of TGSE BLADE DWI compared with RESOLVE DWI in the diagnosis of cholesteatoma. BMC Med Imaging 2020; 20(1): 40.
5. Okuchi S, Fushimi Y, Yoshida K, et al. Comparison of TGSE-BLADE DWI, RESOLVE DWI, and SS-EPI DWI in healthy volunteers and patients after cerebral aneurysm clipping. Sci Rep 2022; 12(1): 17689.
6. Li X, Zhu H, Sun K, Chai W, Fu C, Yan F. Is simultaneous multi-slice readout-segmented echo-planar imaging valuable for predicting molecular subtypes of breast cancer? Eur J Radiol 2022; 150: 110232.
Figures
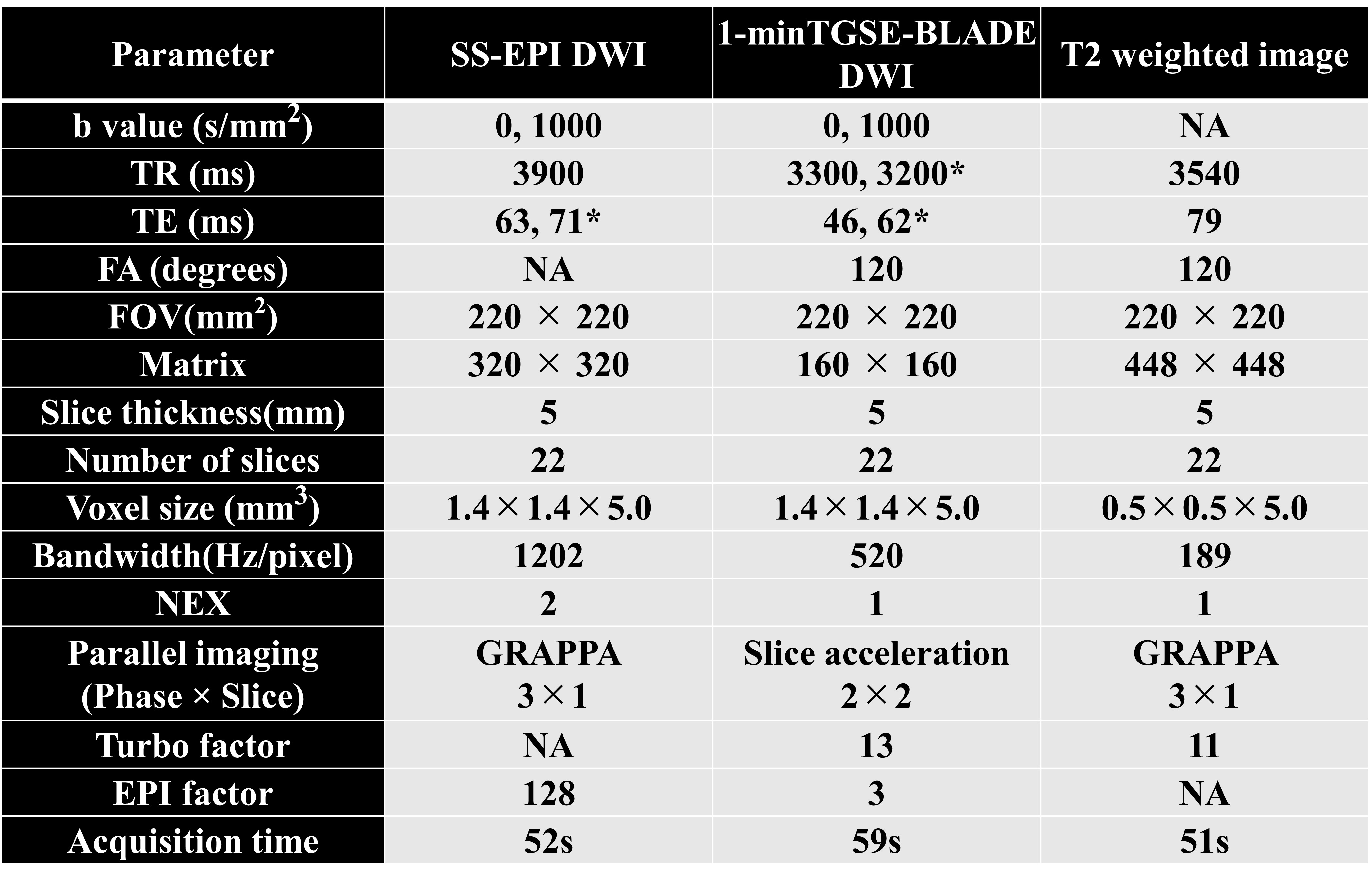
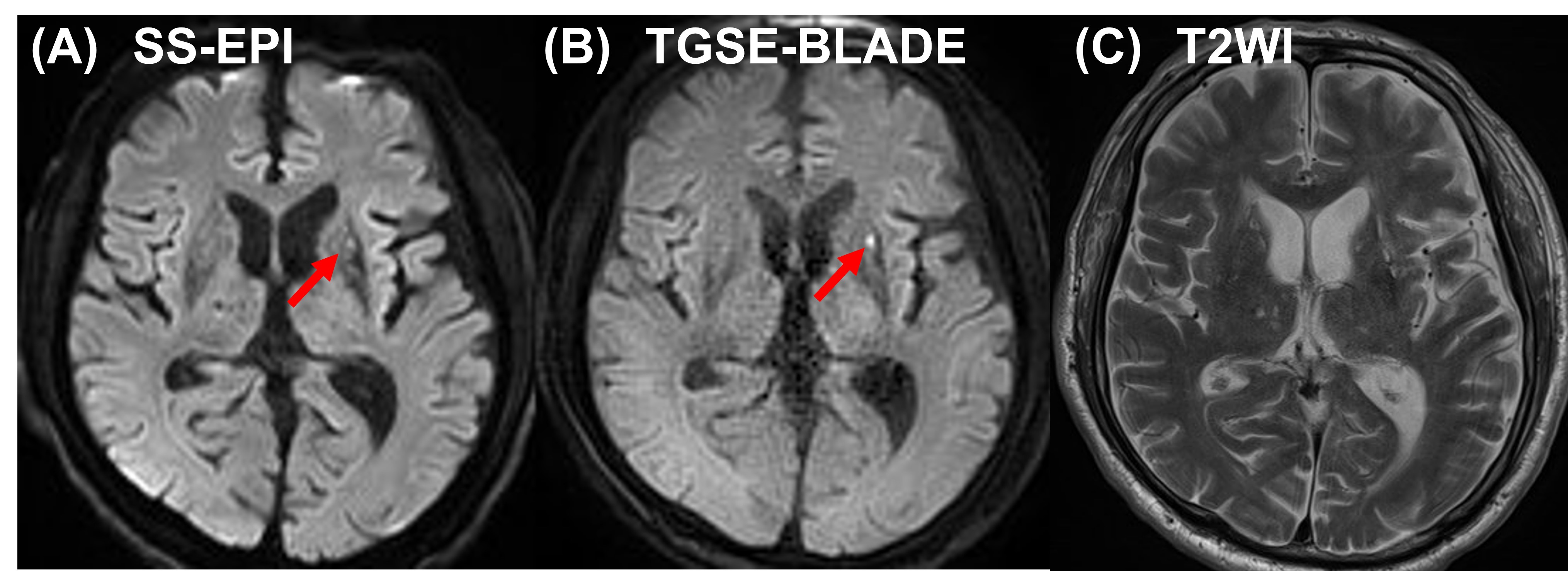
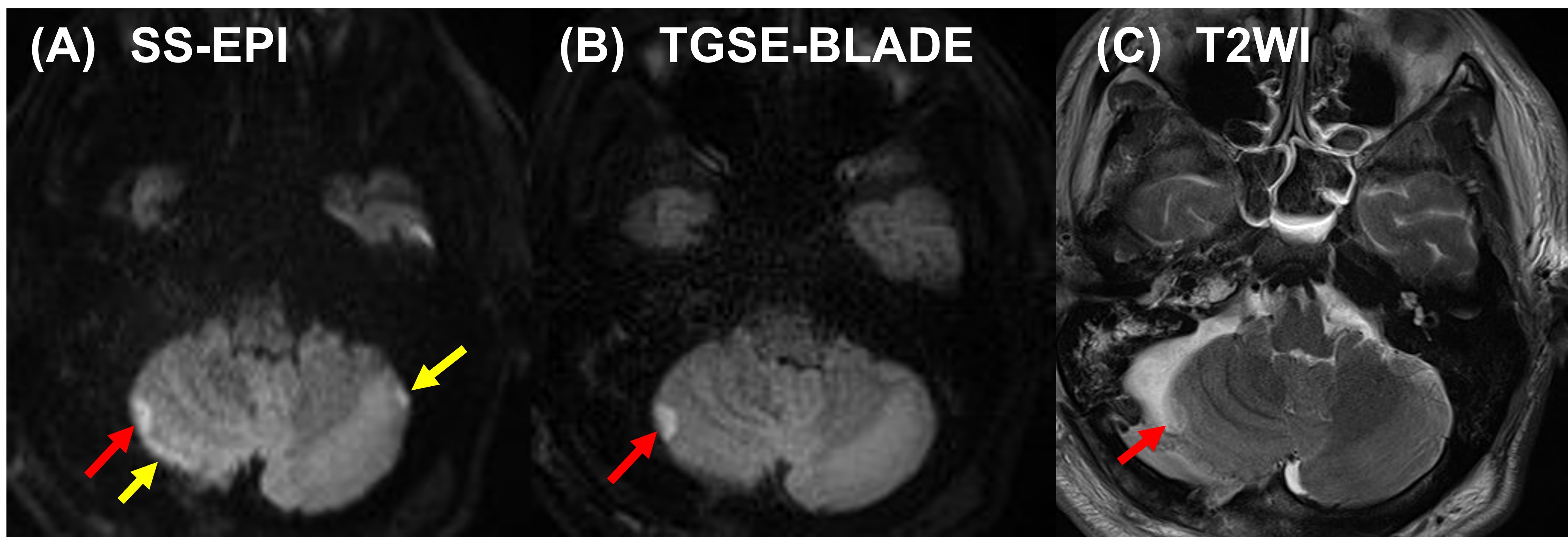
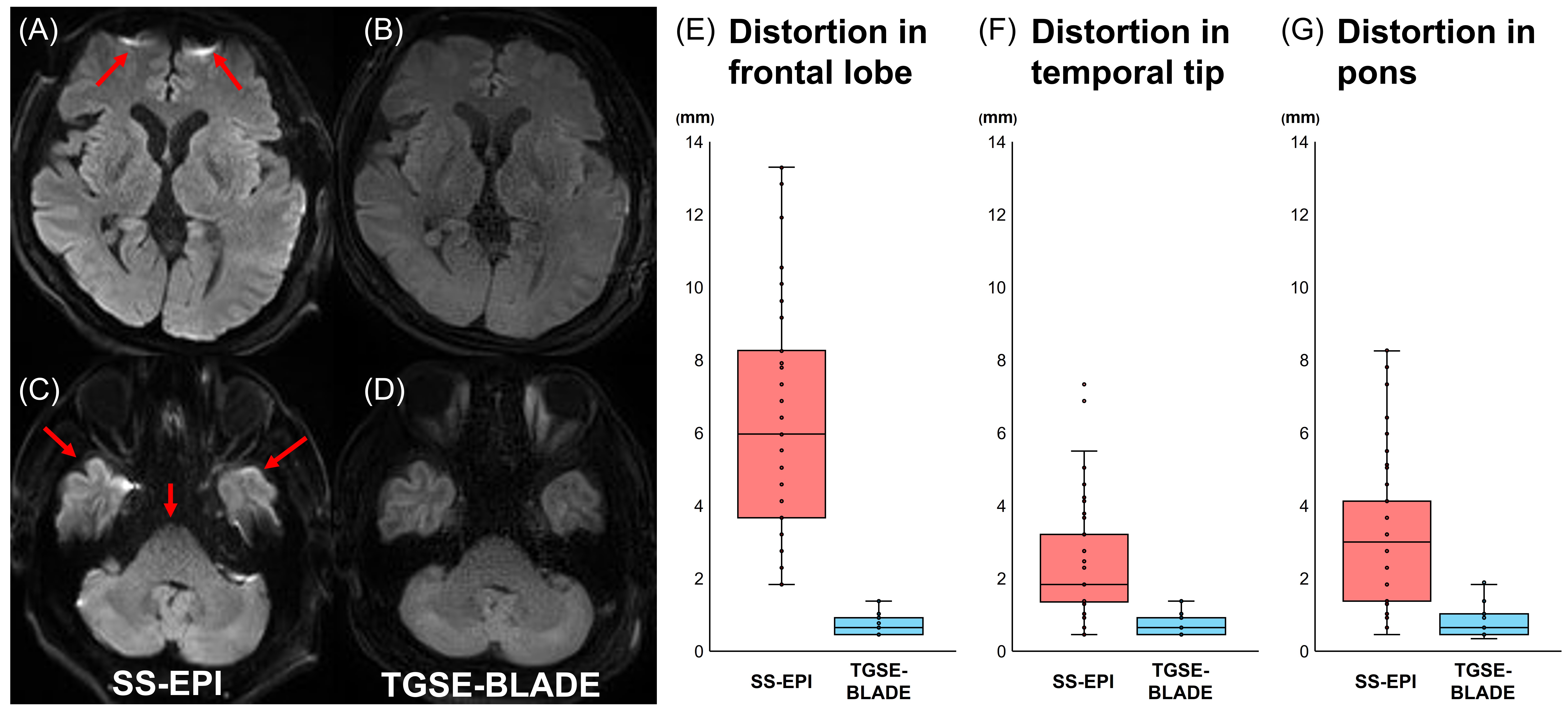
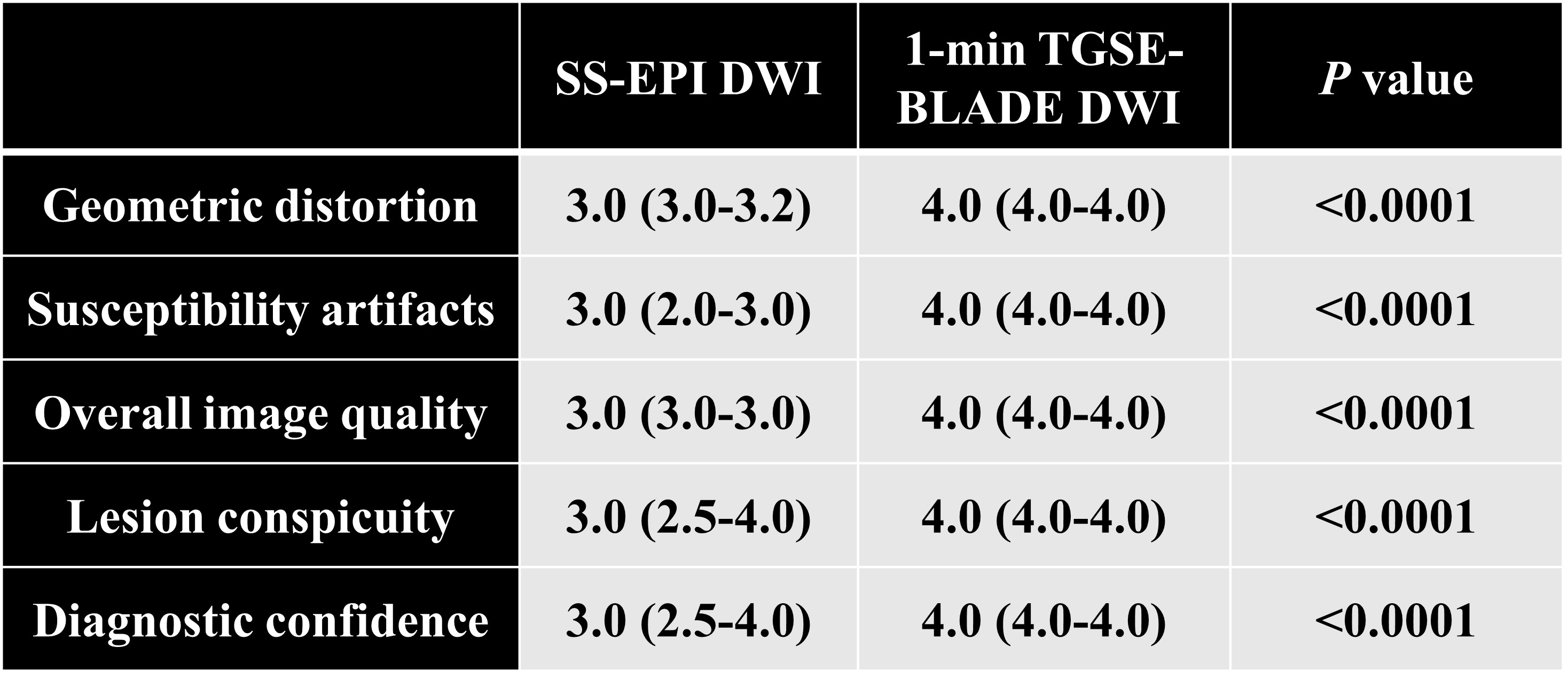
Figure 5. Results of the scores for geometric distortion, susceptibility artifacts, overall image quality, lesion conspicuity and diagnostic confidence.
Note – Data are presented as the median (interquartile range) score.