2079
Correlation of Endolymphatic Hydrops and Perilymphatic Enhancement with Clinical Features of Ménière’s Disease1shangdong provincial ENT hospital, Jinan, China, 2Siemens healthineers, Shanghai, China, 3Shandong Provincial ENT Hospital, Jinan, China, 4Shandong Mental Health Center, Jinan, China
Synopsis
Keywords: Head & Neck/ENT, Head & Neck/ENT
To investigate the correlation of the EH grade and PE with clinical features in MD, we evaluated their correlations by using the cubic spline models and multivariate analysis. We found that a nonlinear or linear correlation of EH grade and SIR with duration of disease-related symptoms and hearing thresholds. Additionally, the higher duration of vertigo and LFHT were associated with a higher EH grade, as well as duration of tinnitus and vestibular EH for SIR. Consequently, the grades of EH and the extent of PE in patients with MD can be evaluated by use of some clinical features and PTA.BACKGROUND AND PURPOSE
Ménière’s disease (MD) is a common disorder of the inner ear which characterized by recurrent, spontaneous episodes of vertigo, hearing loss, aural fullness and tinnitus.1 What’s more, endolymphatic hydrops (EH) and perilymphatic enhancement (PE) were discriminating parameters for MD. Magnetic resonance imaging after intravenous injection of contrast agent enables to bilaterally grade and ascertain PE, and then can investigate their correlation with MD symptoms or audiovestibular function tests. However, the findings available on this correlation in literature were inconsistent and controversial thus far. So, we analyzed the correlation of EH and PE via MRI with MD symptoms and pure-tone average (PTA) in a large population of definite unilateral MD by the use of multivariate analysis.MATERIALS AND METHODS
From September 2020 to October 2021, 274 consecutive patients (123 males and 150 females, median age: 53 years) with definite unilateral Ménière’s disease were recruited. All patients were scanned on a 3T MR system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with 64 channel head coil. 3D-ZOOMit real IR and 3D-T2WI were performed after 6 h gadolinium injection with a double dose (0.4 ml/kg body weight; ProHance). The parameters of ZOOMit 3D real IR are as below: TR 8000ms, TE 491ms, TI 2250, FOV 160mm×80mm, voxel size 0.6mm×0.6mm and scan time 15min12s. The grades of cochlear and vestibular EH were evaluated separately by 2 radiologists independently. The grades of cochlear EH were classified into three levels: none, grade I, and grade II, according to the criteria described previously, 2, 3 and of vestibular EH using a modified four-stage grading system based on Bernaerts 3 described: none, grade I, grade II or grade III, separately. The signal intensity ratio was calculated using the following equations:SIR = SIperi/SIlmcp [Eq. 1]
Where, SIperi and SIlmcp present the signal intensity of the cochlear basal turn and the left middle cerebellar peduncle of the images. Multivariate analysis was performed by backward stepwise regression using R software (v 4.1.3). The nonlinear correlations between continuous variables and outcomes were analyzed using the restricted cubic spline using rms packages of R software (v 4.1.3). If a nonlinear correlation happened, using quartiles for classification as quartile 1 (Q1), quartile 2 (Q2), quartile 3 (Q3), and quartile 4 (Q4), and the lowest quartile served as the referent. Statistical significance was set at P values < 0.05.
RESULTS
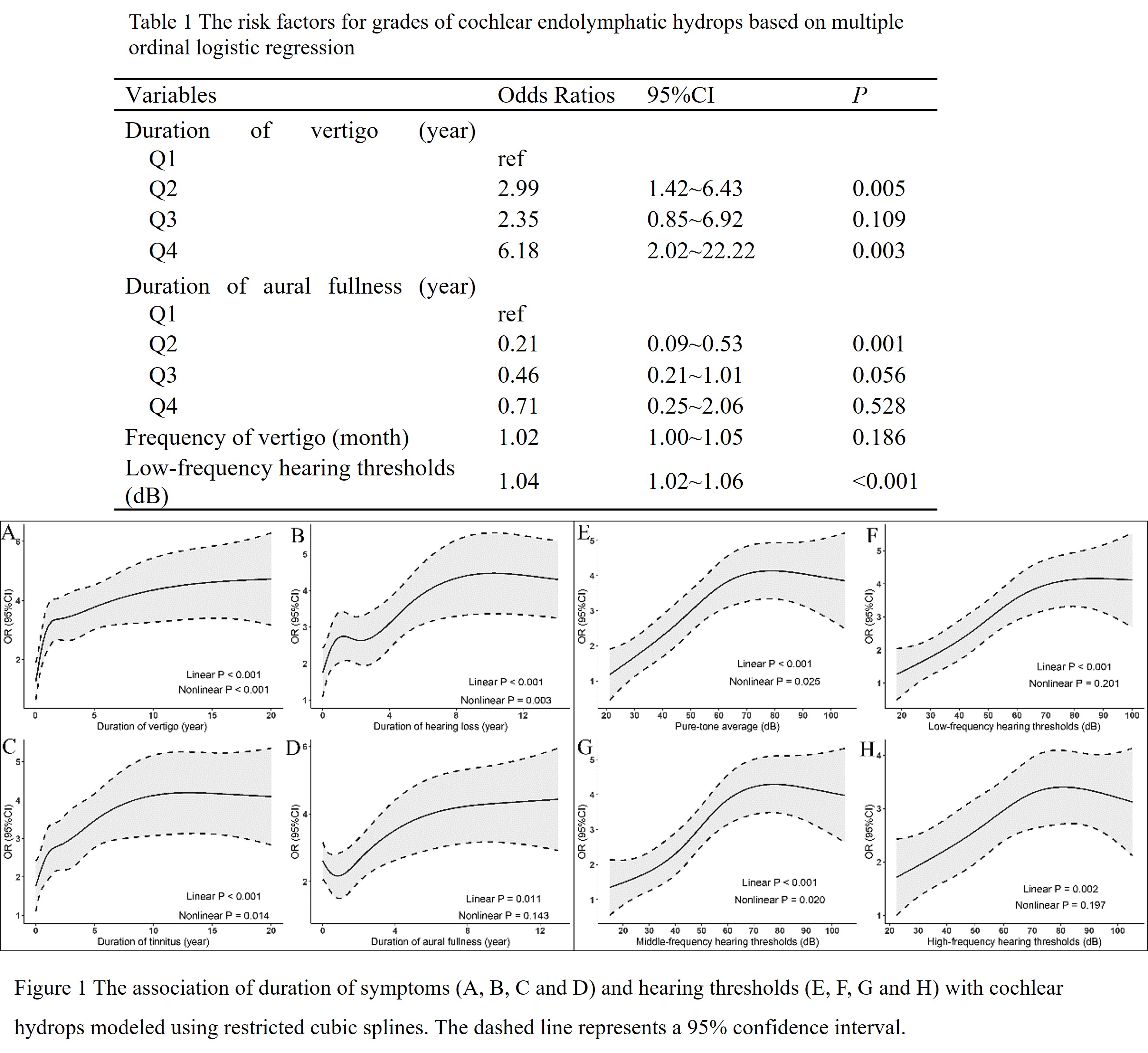
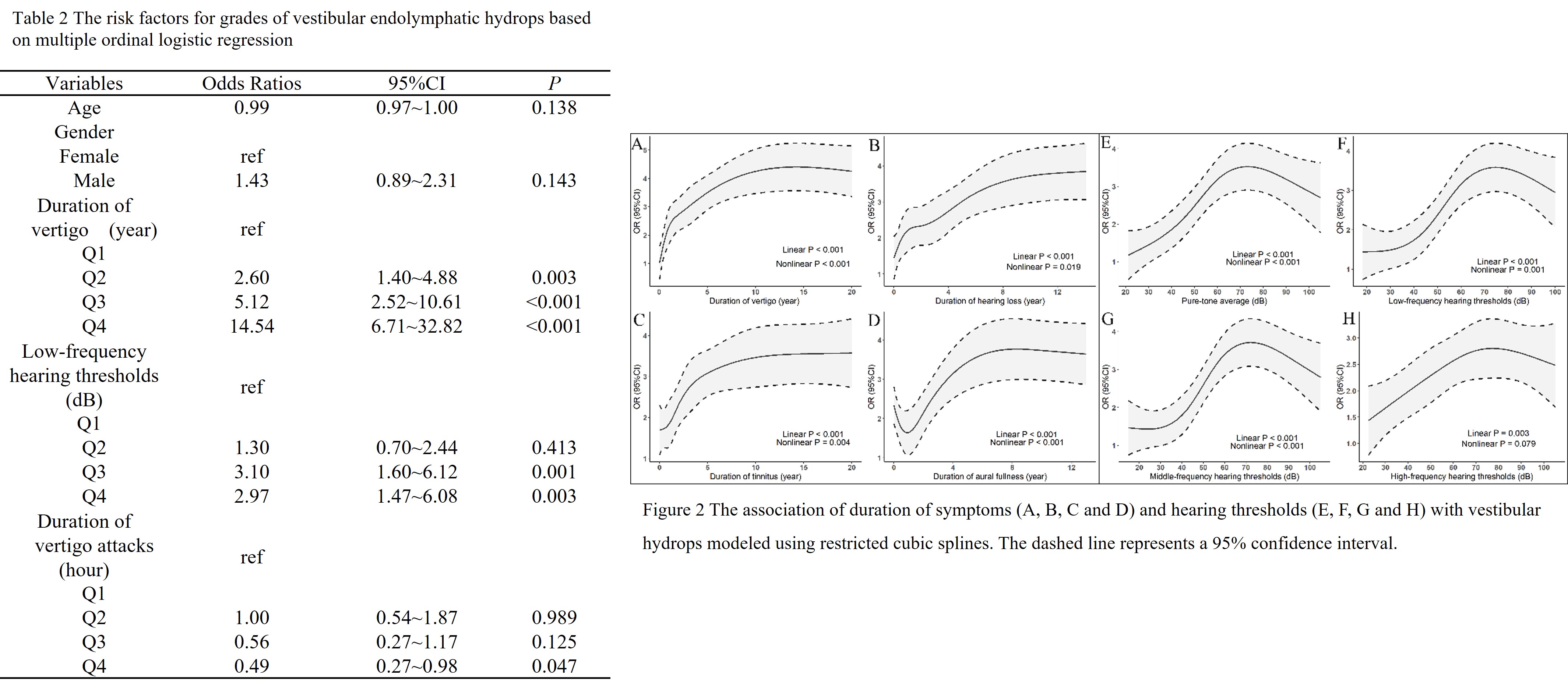
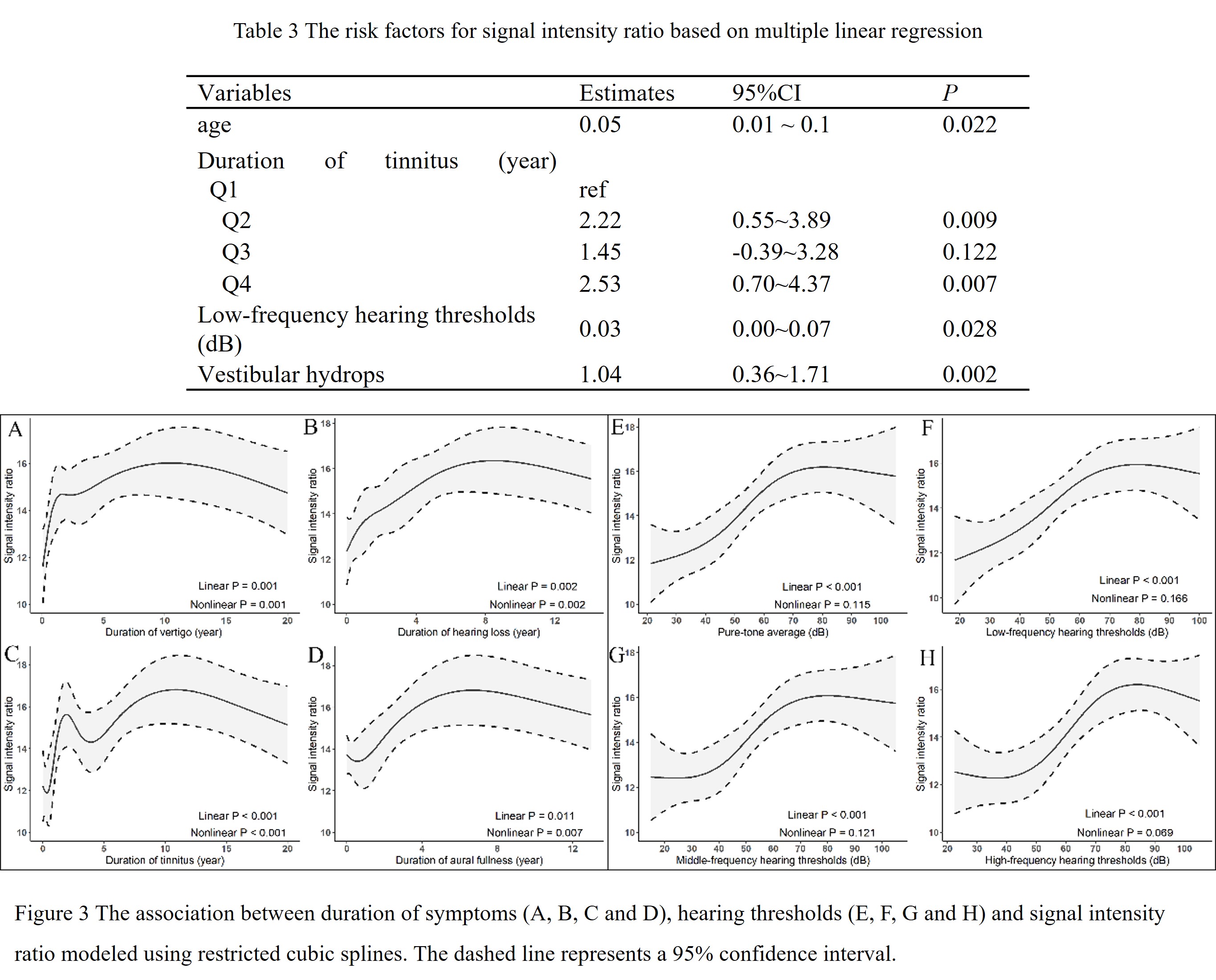
A nonlinear or linear correlation of EH grade and SIR with some clinical features and hearing thresholds (Fig. 1-3). Based on ordinal logistic regression models, the higher duration of vertigo was associated for being a higher grade of cochlear EH, whereas duration of aural fullness was a protective factor for cochlear EH (Table 1). Additionally, the higher duration of vertigo was associated with a higher grade of vestibular EH, whereas the duration of vertigo attacks is a protective factor for the grade of vestibular EH (Table 2). Moreover, the age and duration of tinnitus and vestibular EH are risk factors for SIR by multiple linear regression (Table 3). Furthermore, the low-frequency hearing thresholds (125, 250, and 500 Hz, LFHT) is a risk factor for cochlear EH, vestibular EH and SIR.DISCUSSION
In our study, the grades of EH and the extent of PE have relevance to the clinical features and PTA. The correlations concluded by using the cubic spline models can better show their actual tendency of changing. Moreover, we analyzed the correlation of EH and PE with clinical features and PTA by the use of multivariate analysis which can control for the potential confounding effect of other variables. Consequently, the conclusion is more convincing.CONCLUSIONS
The duration of disease-related symptoms and hearing thresholds can be used to predict the grades of EH and the extent of PE in patients with MD.Acknowledgements
NoneReferences
1.Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Menière's disease. American Academy of Otolaryngology-Head and Neck Foundation, Inc. Otolaryngol Head Neck Surg 1995;113:181-185.https://doi.org/10.1016/S0194-5998(95)70102-8
2.Barath K, Schuknecht B, Naldi AM, et al. Detection and grading of endolymphatic hydrops in Meniere disease using MR imaging. AJNR Am J Neuroradiol 2014;35:1387-1392.https://doi.org/10.3174/ajnr.A3856 3.Bernaerts A, Vanspauwen R, Blaivie C, et al. The value of four stage vestibular hydrops grading and asymmetric perilymphatic enhancement in the diagnosis of Meniere's disease on MRI. Neuroradiology 2019;61:421-429.https://doi.org/10.1007/s00234-019-02155-7
Figures