2060
Evaluation of urethral sphincter complex after LRP based on 3.0T pelvic floor magnetic resonance imaging combined with DTI and fiber tractography1the First Affiliated Hospital of Zhengzhou University, Zhengzhou, China
Synopsis
Keywords: Prostate, Diffusion Tensor Imaging, Radical prostatectomy; Urethral sphincters complex; Urinary incontinence
The anatomical-morphological and functional characteristics of the urethral sphincter complex, a key structure in the mechanism of urinary continence, have been studied mostly based on cadaveric dissection or animal experiments. In this study,we qualitatively and quantitatively evaluated the morphology and function of the urethral sphincter complex in patients after laparoscopic radical prostatectomy (LRP) using pelvic floor MRI combined with DTI and fiber tractography, and to investigate the anatomical factors affecting PPI.Purpose
This study aimed to qualitatively and quantitatively analyze the morphology and function of the urethral sphincter complex in patients after laparoscopic radical prostatectomy (LRP) using pelvic floor MRI combined with diffusion tensor imaging (DTI) and fiber tractography, and to investigate the anatomical factors affecting postprostatectomy incontinence (PPI).Methods
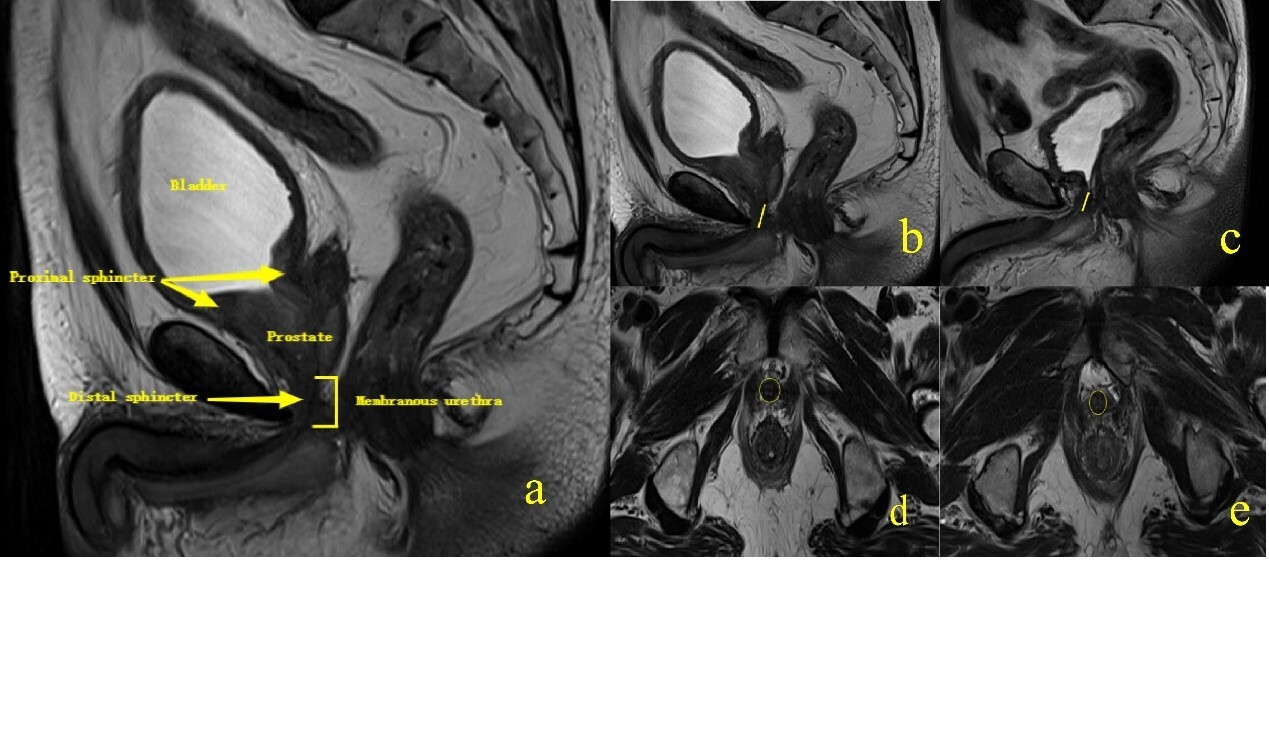
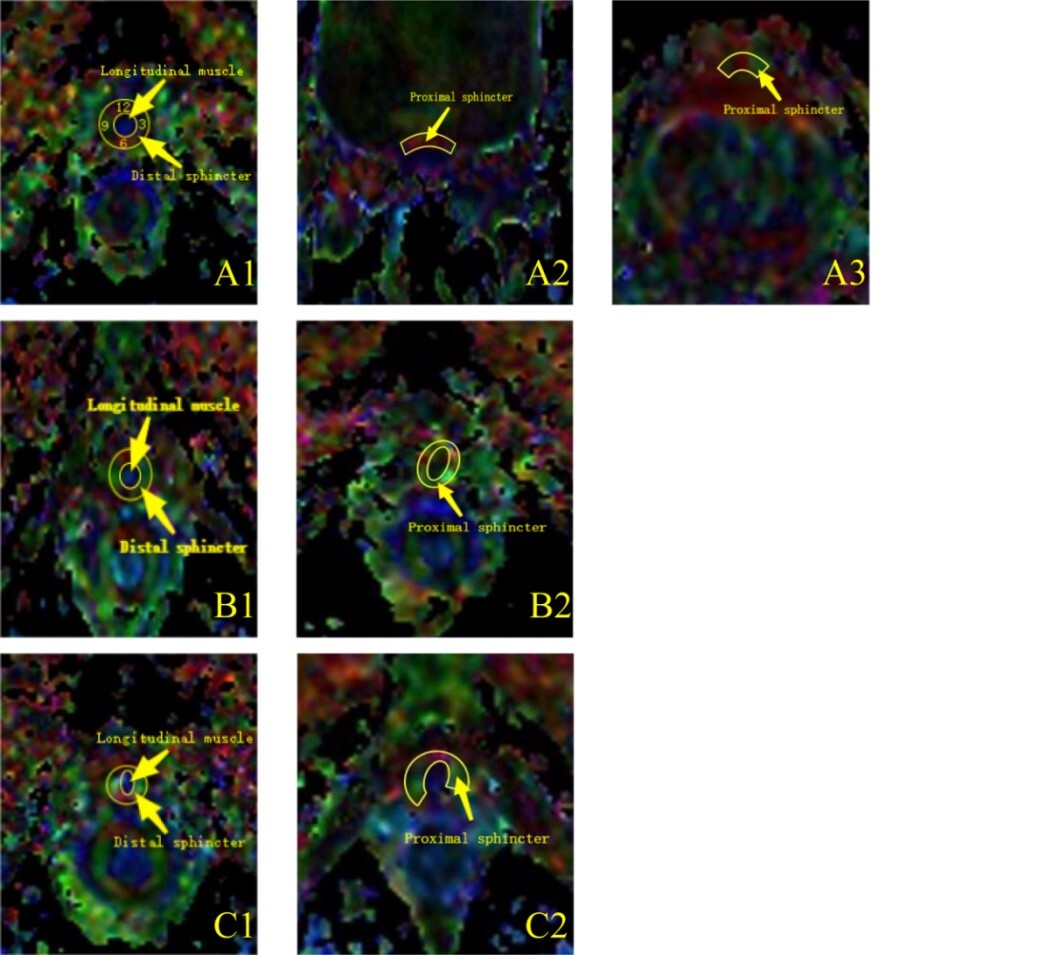
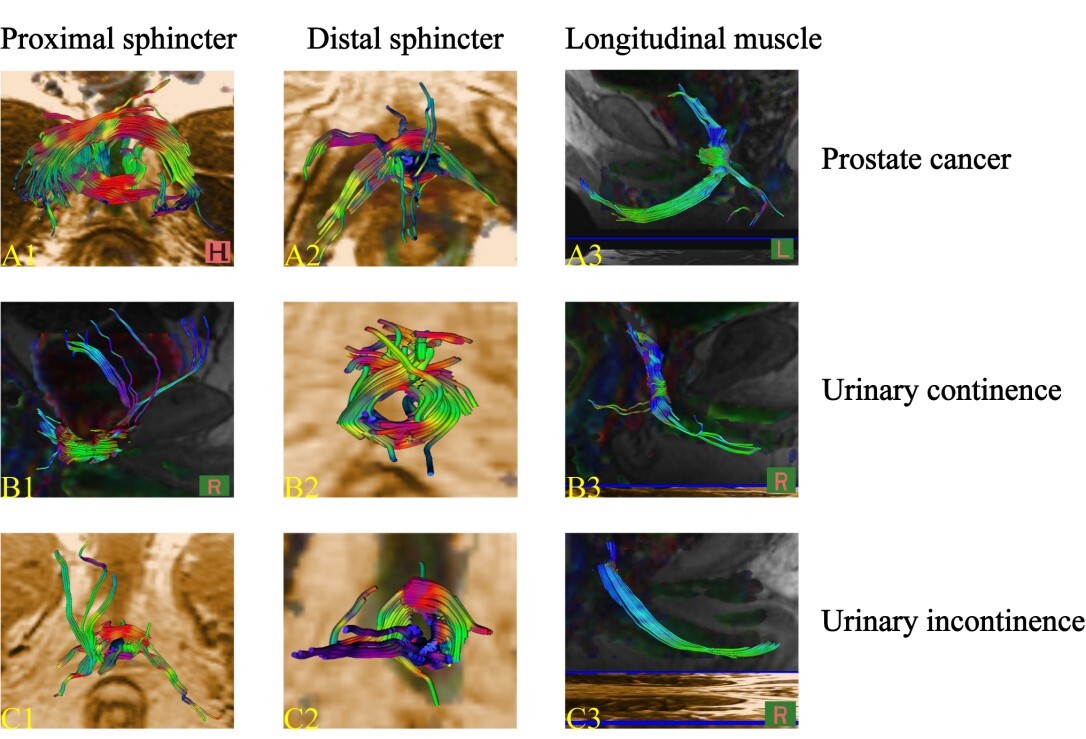
This prospective study included 38 patients who underwent LRP for prostate cancer, the patients were divided into urinary continence group (n=21) and urinary incontinence group (n=17). Membranous urethral length (MUL) and membranous urethral thickness (MUT) were measured on pelvic sagittal and axial T2 weighted images respectively. Fiber tractography of each analyzed structure of the urethral sphincter complex was performed. DTI-derived metrics, including fractional anisotropy (FA), apparent diffusion coefficient (ADC) and the three eigenvalues (λ1, λ2, λ3) were calculated. And the correlations between FA and ADC values of two-group urethral sphincter complex and the score of International Consultation Incontinence Questionnaire-Short Form (ICIQ-SF) were evaluated.Results
Regarding pelvic MRI parameters, both preoperative and postoperative urinary continence groups had greater MUL than in the incontinence group, while the differences of MUT was not significant. As for DTI-derived metrics, the proximal and distal sphincters of postoperative patients showed significant decrease in FA value, increase in ADC value and the three eigenvalues, and FA values of the proximal sphincter and intermediate longitudinal muscle were higher in the urinary continence group compared to the incontinence group. In addition, the ICIQ-SF score was negatively correlated with FA value of proximal sphincter in continence group and with FA value of intermediate longitudinal muscle in incontinence group.Conclusions
Pelvic floor MRI combined with DTI and fiber tractography is an effective and reliable non-invasive tool to assess the urethral sphincter complex. We found that the anatomical injury of proximal sphincter and intermediate longitudinal muscle is an important factor leading to the occurrence of postprostatectomy incontinence (PPI).Acknowledgements
NoneReferences
[1] S. Sandhu, C.M. Moore, E. Chiong, H. Beltran, R.G. Bristow, S.G. Williams, Prostate cancer, The Lancet 398(10305) (2021) 1075-1090.
[2] R.M. Bauer, C. Gozzi, W. Hubner, V.W. Nitti, G. Novara, A. Peterson, J.S. Sandhu, C.G. Stief, Contemporary management of postprostatectomy incontinence, Eur Urol 59(6) (2011) 985-96.
[3] C.A. Anderson, M.I. Omar, S.E. Campbell, K.F. Hunter, J.D. Cody, C.M. Glazener, Conservative management for postprostatectomy urinary incontinence, Cochrane Database Syst Rev 1 (2015) CD001843.
[4] Y.D. Dubbelman, J. Groen, M.F. Wildhagen, B. Rikken, J.L. Bosch, Urodynamic quantification of decrease in sphincter function after radical prostatectomy: relation to postoperative continence status and the effect of intensive pelvic floor muscle exercises, Neurourol Urodyn 31(5) (2012) 646-51.
[5] C. von Bodman, K. Matsushita, C. Savage, M.P. Matikainen, J.A. Eastham, P.T. Scardino, F. Rabbani, O. Akin, J.S. Sandhu, Recovery of urinary function after radical prostatectomy: predictors of urinary function on preoperative prostate magnetic resonance imaging, J Urol 187(3) (2012) 945-50.
[6] M. Kim, M. Park, S. Pak, S.K. Choi, M. Shim, C. Song, H. Ahn, Integrity of the Urethral Sphincter Complex, Nerve-sparing, and Long-term Continence Status after Robotic-assisted Radical Prostatectomy, Eur Urol Focus 5(5) (2019) 823-830.
[7] M.M. Koraitim, The male urethral sphincter complex revisited: an anatomical concept and its physiological correlate, J Urol 179(5) (2008) 1683-9.
[8] X.D. Wang, S. Liu, L.X. Xiong, P.Y. Sun, X.S. Wang, Normal anatomy of urethral sphincter complex in young Chinese males on MRI, Int Urol Nephrol 46(8) (2014) 1469-76.
[9] Y.D. Dubbelman, J.L. Bosch, Urethral sphincter function before and after radical prostatectomy: Systematic review of the prognostic value of various assessment techniques, Neurourol Urodyn 32(7) (2013) 957-63.
[10] Y.-T. Wang, Y.-C. Li, W.-F. Kong, L.-L. Yin, H. Pu, Diffusion tensor imaging beyond brains: Applications in abdominal and pelvic organs, World Journal of Meta-Analysis 5(3) (2017).
[11] S. Sinha, U. Sinha, V. Malis, V. Bhargava, K. Sakamoto, M. Rajasekaran, Exploration of male urethral sphincter complex using diffusion tensor imaging (DTI)-based fiber-tracking, J Magn Reson Imaging 48(4) (2018) 1002-1011.
[12] A.S.C. Verde, J. Santinha, E. Carrasquinha, N. Loucao, A. Gaivao, J. Fonseca, C. Matos, N. Papanikolaou, Diffusion tensor-based fiber tracking of the male urethral sphincter complex in patients undergoing radical prostatectomy: a feasibility study, Insights Imaging 11(1) (2020) 126.
[13] C. Roy, M. Ohana, A. Labani, T. Tricard, C. Saussine, P. Leyendecker, Evaluation of the female bladder neck and urethra using MRI with fiber tractography: Prospective study on a large cohort of continent women, Neurourol Urodyn 40(6) (2021) 1441-1449.
[14] C. D'Ancona, B. Haylen, M. Oelke, L. Abranches-Monteiro, E. Arnold, H. Goldman, R. Hamid, Y. Homma, T. Marcelissen, K. Rademakers, A. Schizas, A. Singla, I. Soto, V. Tse, S. de Wachter, S. Herschorn, I.C.S. Standardisation Steering Committee, I.C.S.W.G.o.T.f.M.L.U.T. the, S. Pelvic Floor, Dysfunction, The International Continence Society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction, Neurourol Urodyn 38(2) (2019) 433-477.
[15] V. Iacovelli, M. Carilli, M. Sandri, V. Forte, C. Cipriani, R. Bertolo, M. Vittori, F. Petta, F. Maiorino, M. Signoretti, M. Antonucci, A.U. Cavallo, M. Sperandio, E. Finazzi Agro, P. Bove, The role of preoperative prostatic shape in the recovery of urinary continence after robotic radical prostatectomy: a single cohort analysis, Prostate Cancer Prostatic Dis (2022).
[16] M. Sauer, P. Tennstedt, C. Berliner, L. Well, H. Huland, L. Budaus, G. Adam, D. Beyersdorff, Predictors of short and long term urinary incontinence after radical prostatectomy in prostate MRI: Significance and reliability of standardized measurements, Eur J Radiol 120 (2019) 108668.
[17] B. Hoeh, F. Preisser, M. Wenzel, C. Humke, C. Wittler, J.L. Hohenhorst, M. Volckmann-Wilde, J. Kollermann, T. Steuber, M. Graefen, D. Tilki, P.I. Karakiewicz, A. Becker, L.A. Kluth, F.K.H. Chun, P. Mandel, Correlation of Urine Loss after Catheter Removal and Early Continence in Men Undergoing Radical Prostatectomy, Curr Oncol 28(6) (2021) 4738-4747.
[18] S.F. Mungovan, J.S. Sandhu, O. Akin, N.A. Smart, P.L. Graham, M.I. Patel, Preoperative Membranous Urethral Length Measurement and Continence Recovery Following Radical Prostatectomy: A Systematic Review and Meta-analysis, Eur Urol 71(3) (2017) 368-378.
[19] Y. Kadono, T. Nohara, S. Kawaguchi, R. Naito, S. Urata, K. Nakashima, M. Iijima, K. Shigehara, K. Izumi, T. Gabata, A. Mizokami, Investigating the mechanism underlying urinary continence recovery after radical prostatectomy: effectiveness of a longer urethral stump to prevent urinary incontinence, BJU international 122(3) (2018) 456-462.
[20] A. Tienza, J.E. Robles, M. Hevia, R. Algarra, F. Diez-Caballero, J.I. Pascual, Prevalence analysis of urinary incontinence after radical prostatectomy and influential preoperative factors in a single institution, Aging Male 21(1) (2018) 24-30.
[21] T. Sadahira, Y. Mitsui, M. Araki, Y. Maruyama, K. Wada, K. Edamura, Y. Kobayashi, M. Watanabe, T. Watanabe, Y. Nasu, Pelvic magnetic resonance imaging parameters predict urinary incontinence after robot-assisted radical prostatectomy, Low Urin Tract Symptoms 11(3) (2019) 122-126.
[22] D.C. Karampinos, K.F. King, B.P. Sutton, J.G. Georgiadis, Myofiber ellipticity as an explanation for transverse asymmetry of skeletal muscle diffusion MRI in vivo signal, Ann Biomed Eng 37(12) (2009) 2532-46.
[23] Y. Okamoto, G.J. Kemp, T. Isobe, E. Sato, Y. Hirano, J. Shoda, M. Minami, Changes in diffusion tensor imaging (DTI) eigenvalues of skeletal muscle due to hybrid exercise training, Magn Reson Imaging 32(10) (2014) 1297-300.
[24] C. Cui, Y. Zhao, D. Cui, N. Li, J. Pan, W. Shen, In vivo evaluation of the levator ani muscle in primiparous women using diffusion tensor imaging and fiber tractography, Int J Gynaecol Obstet 157(3) (2022) 663-670.
[25] M.A. Mistry, N. Klarskov, J.O. DeLancey, G. Lose, A structured review on the female urethral anatomy and innervation with an emphasis on the role of the urethral longitudinal smooth muscle, Int Urogynecol J 31(1) (2020) 63-71.
Figures