2044
Repeatability and reliability of liver quantitative maps in differentiation of hepatic fibrosis stage
Tianzhu Liu1, Lesheng Huang1, Weiyin Vivian Liu2, and Jun Chen1
1Guangdong Hospital of Traditional Chinese Medicine, Zhuhai, China, 2MR Research China, GE Healthcare, Beijing, China
1Guangdong Hospital of Traditional Chinese Medicine, Zhuhai, China, 2MR Research China, GE Healthcare, Beijing, China
Synopsis
Keywords: Liver, Data Analysis
Grading liver fibrosis using intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI) have been shown inconsistent results possibly for differences between liver segments and recruited types of patients. We systematically evaluated all measurements retrieved based on liver segments and classified by stage of liver fibrosis, and inconsistent repeatability and reliability of IVIM-derived values were found, attributing to inter- and intra- manual measurement bias and inhomogeneous distribution of tissue components such as fibrosis. ROC curve analysis showed moderate diagnostic efficiency between early hepatic fibrosis (EHF) and advanced HF (AHF), but not HCs from EHF based on IVIM-derived parameters with acceptable repeatability and reliability.Introduction
Intravoxel incoherent motion (IVIM) is a single-shot spin echo–based DWI technique that utilizes multiple b values, enabling the two-component (pure molecular diffusion and perfusion) analysis of random water motion in organic tissues and yielding pure molecular diffusion coefficient (D), pseudo-diffusion coefficient (D*), and perfusion fraction (f). [1] Despite the increase in applications for quantitative measurement of liver lesions, studies have yielded inconsistent results of parameters relevant to diagnosis and fibrosis grading; [2, 3, 4] however, they found positive, negative, or nonlinear correlation between IVIM measures and liver fibrosis grading. Most studies have performed ROI measurements on the right lobe segments because the left lobe is smaller and more susceptible to breathing artifacts and cardiac impulse movements. [5] Thus, we aimed to systematically evaluate the repeatability and reliability of ROI-based measurements for each liver segment and its correlation with hepatic fibrosis (HF) in participants with hepatic fibrosis (HF) and healthy volunteers (HV), and also assess the diagnostic efficiency in HV and HF groups based on IVIM-derived parameters of liver segments.Materials and methods
Methods: This prospective study was approved by the institutional review board and ethics committee of our hospital. Participants with hepatitis B and hepatic fibrosis (HF), and healthy controls (HCs) (aged > 18 years) were consecutively recruited between 11 June 2020 and 1 September 2022. Participants with early hepatic fibrosis (EHF) or advanced hepatic fibrosis (AHF) and HV were recruited. In the EHF and AHF groups, needle biopsy or laparoscopic biopsy was conducted as the gold standard reference and the inclusion criterion was a history of hepatitis B. MRI examinations were performed on a 3.0-T scanner (Signa Discovery 750w; GE Healthcare, MA, USA) equipped with a 16-channel abdominal coil. The DWI protocol for all participants included the acquisition of 12 b values (at 0, 25, 50, 75, 100, 150, 200, 300, 400, 500, 600, and 800 s/mm2). Ordinal logistic regression analysis was applied to explore the potential influencing factors of repeatability and reliability, and collinearity diagnosis was applied to eliminate the highly correlated independent variables; age, sex, hepatitis severity, IVIM-derived parameters, segments, and groups were included as independent variables. Two examiners measured and analyzed IVIM data using mono-, bi-exponential and stretched exponential models and one of them repeated the procedure. The intra- and inter-examiner repeatability (coefficients of variation, CV) and reliability (intraclass correlation coefficients, ICC) of IVIM-DWI. Receiver operating characteristic (ROC) curve analysis was performed to assess the diagnostic efficacy.Results
48 HCs, 57 participants with EHF, and 38 with AHF were included. The repeatability of D* (CV: 26.62–41.47%) and DDC (distributed diffusion coefficient) (CV: 18.01–34.40%) were poor, while that for ADC (apparent diffusion coefficient) (CV: 4.95–9.76%), D (CV: 7.09–15.52%), f (CV: 9.35–17.15%), and α (CV: 7.48–13.81%) were better. The intra- and inter-reader CV of all measurements on IVIM-derived paramter maps was respectively shown in Figure 2 and 3. ICC for IVIM-derived parameters in liver segments Ⅴ–Ⅷ of participants for intra- and inter-readers was respectively shown in Table 1 and 2. In the ordered logistic regression model, ADC, D*, f, and DDC showed statistically significant (p < 0.001) intra- and inter-examiner repeatability but not reliability. ROC curve analysis showed moderate diagnostic efficacy on differentiating EHF from AHF with AUC of 0.768 (0.676-0.860), 0.744(0.645-0.842) and 0.783(0.693-0.874) for the first and second measurement by the first reader as well as the measurement by the second reader, but not EHF from HCs.Discussion
Our findings showed that the IVIM-derived parameters, especially D*, f, and DDC, were the most important factors in measurement of hepatic fibrosis based on measurement repeatability. For reliability of IVIM-derived parameters, especially D, D*, and DDC, groups and segments of right liver affect measurements mostly. We found that the increase in hepatic fibrosis may reduce the reliability and measured hepatic segments, especially the right lobe, presented significantly low intra- and inter-examiner agreement. This may attribute that participants with EHF and AHF present more heterogeneity in hepatic tissue than HCs. Previous studies have shown poor repeatability with 2 samples from the same participants; the inflammation grade and fibrosis stage of the right lobe differed by 45% based on the Knodell score, [6, 7] indirectly increasing the heterogeneity of hepatitis and development of liver fibrosis. With respect to hepatic segments, the inconsistent statistic differences in reliability may result from physiological or pathological heterogeneity of segments, including but not only blood flow volume, perfusion volume, and the uneven development of hepatic fibrosis; [8] moreover, the partial heterogeneous hepatic areas may be smaller than segments, leading to measurement bias.Conclusions
Overall, IVIM-derived parameters α with the best repeatability and reliability in diagnosis of HF should be measured on segment VI, while amount of hepatic fibrosis and hepatic segments may influence reliability of IVIM-derived parameters.Acknowledgements
No acknowledgement found.References
- Le Bihan D. What can we see with IVIM MRI? Neuroimage. 2019;187:56-67.
- Tosun M, Onal T, Uslu H, Alparslan B, Cetin Akhan S. Intravoxel incoherent motion imaging for diagnosing and staging the liver fibrosis and inflammation. Abdom Radiol (NY). 2020;45:15-23.
- Ren H, Liu Y, Lu J, An W, Wang W, Yan T, et al. Evaluating the clinical value of MRI multi-model diffusion-weighted imaging on liver fibrosis in chronic hepatitis B patients. Abdom Radiol (NY). 2021;46:1552-61.
- Li T, Che-Nordin N, Wang YXJ, Rong PF, Qiu SW, Zhang SW, et al. Intravoxel incoherent motion derived liver perfusion/diffusion readouts can be reliable biomarker for the detection of viral hepatitis B induced liver fibrosis. Quant Imaging Med Surg. 2019;9:371-85.
- Lee Y, Lee SS, Kim N, Kim E, Kim YJ, Yun SC, et al. Intravoxel incoherent motion diffusion-weighted MR imaging of the liver: effect of triggering methods on regional variability and measurement repeatability of quantitative parameters. Radiology. 2015;274:405-15.
- Guido M, Rugge M. Liver biopsy sampling in chronic viral hepatitis. Semin Liver Dis. 2004;24:89-97.
- Schiano T, Azeem S, Bodian C, Bodenheimerjr H, Merati S, Thung S, et al. Importance of Specimen Size in Accurate Needle Liver Biopsy Evaluation of Patients With Chronic Hepatitis C. Clinical Gastroenterology and Hepatology. 2005;3:930-5.
- Rousselet MC, Michalak S, Dupre F, Croue A, Bedossa P, Saint-Andre JP, et al. Sources of variability in histological scoring of chronic viral hepatitis. Hepatology. 2005;41:257-64.
Figures
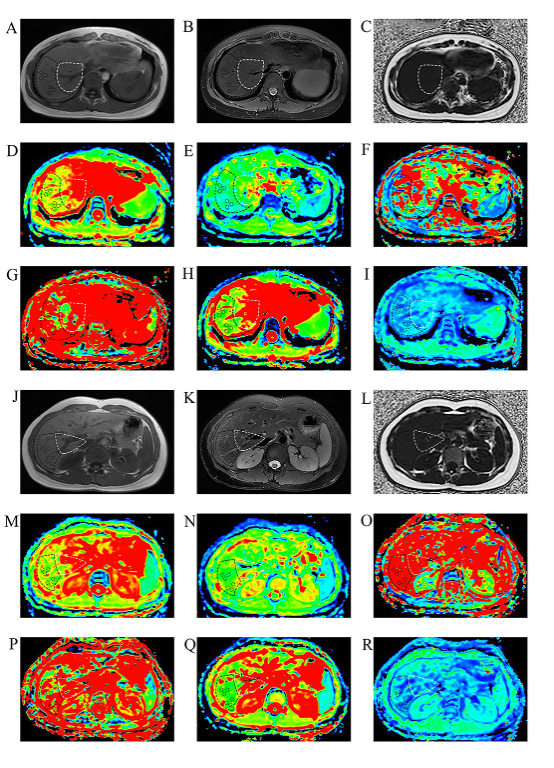
Figure 1 The IVIM and conventional MRI scan from a 45-year-old participant with early liver fibrosis. A-I are the T1WI image, T2 fat compression image, pseudo color map of ADC, D, D*, f, DDC and α of Ⅶ and Ⅷ, respectively; J-R are the T1WI image, T2 fat compression image, pseudo color map of ADC, D, D*, f, DDC, and α of Ⅴ and Ⅵ, respectively.
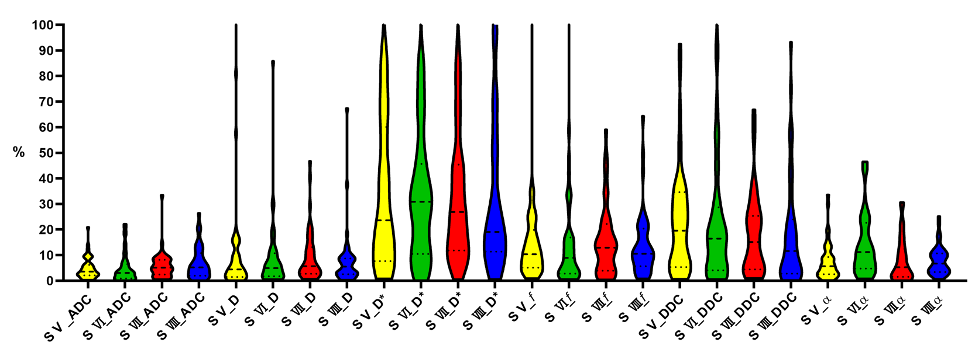
Figure 2 Violin plots for intra-reader coefficient of variance (CV)
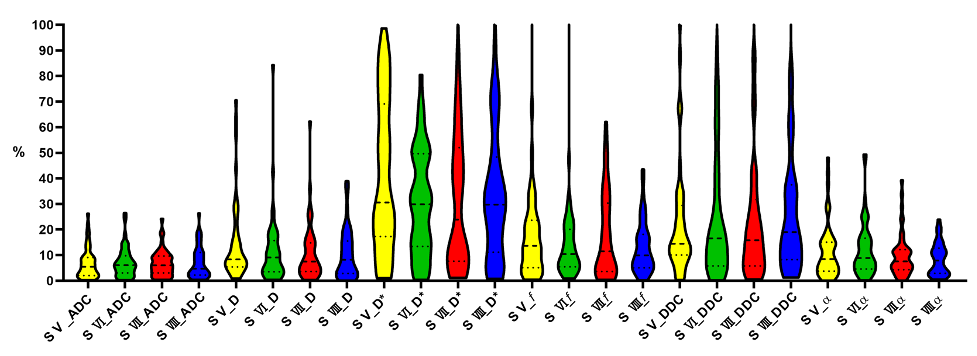
Figure 3 Violin plots for inter-reader coefficient of variance (CV)
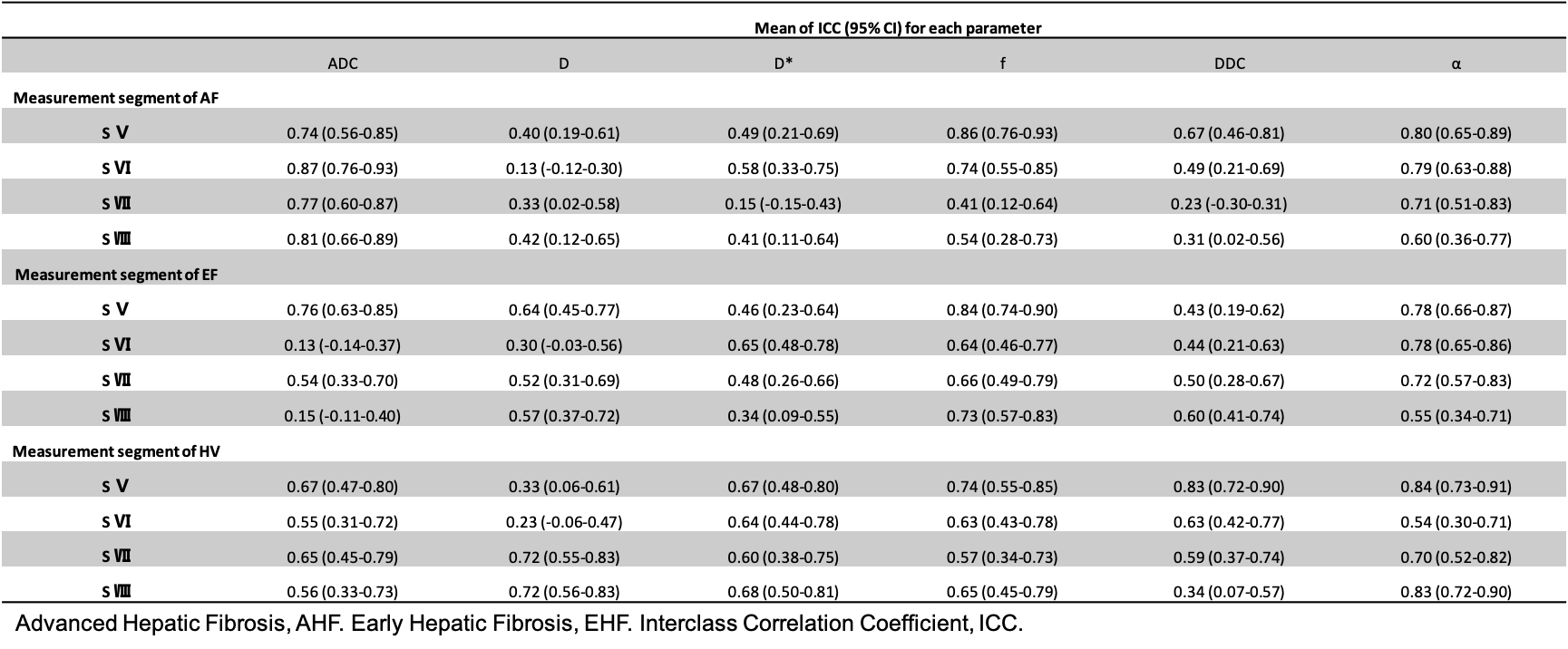
Table 1 ICC for Intra-reader measurements of liver segments Ⅴ–Ⅷ on IVIM-derived quantitative maps
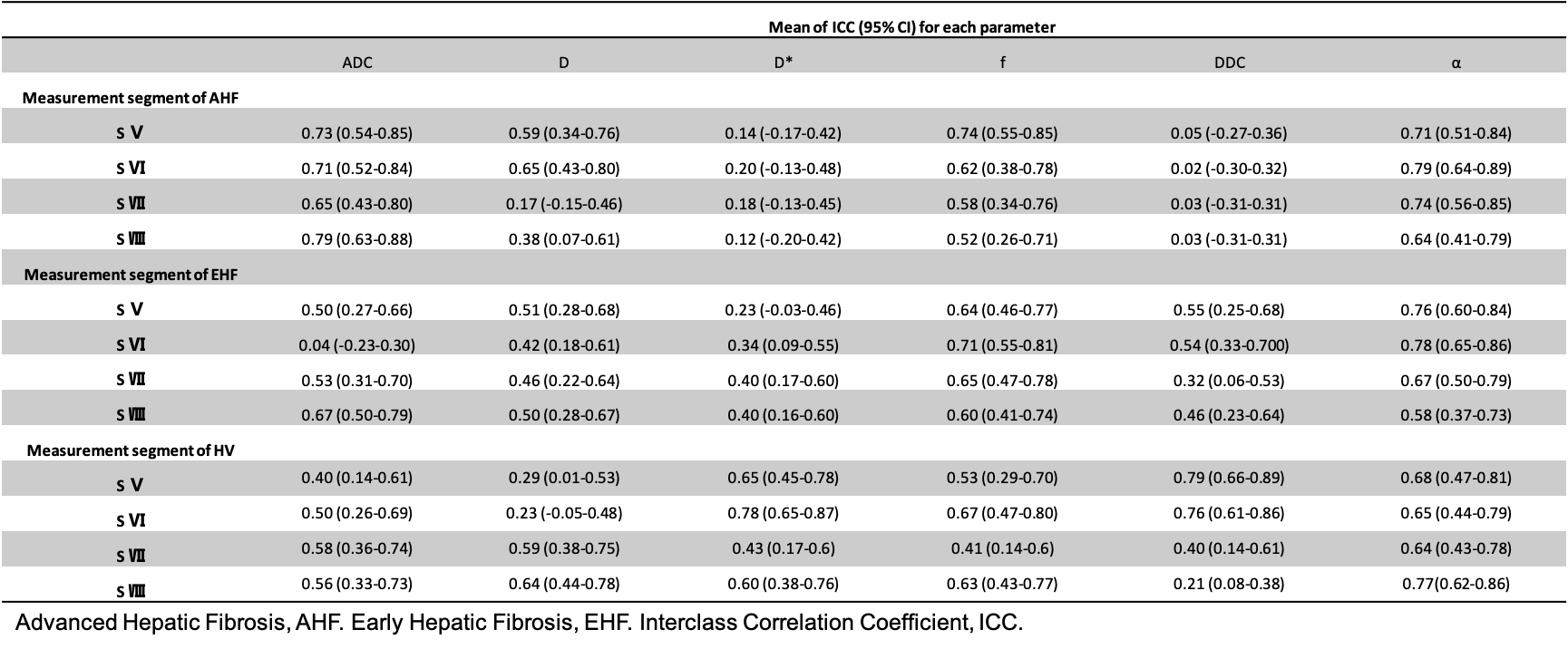
Table 1 ICC for Inter-reader measurements of liver segments Ⅴ–Ⅷ on IVIM-derived quantitative maps
DOI: https://doi.org/10.58530/2023/2044