2020
Validation of respiratory correlated 4D-MRI for radiotherapy planning, using a motion phantom and comparing to 4D-CT.
Joan Chick1, Evanthia Kousi1, Andreas Wetscherek1, Julie Hughes2, Georgina Hopkinson2, Jessica Gough2,3, Rosalyne Westley2,3, Radhouene Neji4, Alex Dunlop1, Simeon Nill1, Henry Mandeville2,3, Katharine Aitken2,3, Dow-Mu Koh2,3, and Uwe Oelfke1
1Joint Department of Physics, The Institute of Cancer Research and Royal Marsden Hospital, London, United Kingdom, 2Royal Marsden Hospital, London, United Kingdom, 3The Institute of Cancer Research, London, United Kingdom, 4MR Research Collaborations, Siemens Healthcare, Frimley, United Kingdom
1Joint Department of Physics, The Institute of Cancer Research and Royal Marsden Hospital, London, United Kingdom, 2Royal Marsden Hospital, London, United Kingdom, 3The Institute of Cancer Research, London, United Kingdom, 4MR Research Collaborations, Siemens Healthcare, Frimley, United Kingdom
Synopsis
Keywords: Data Acquisition, Radiotherapy, Respiratory Correlated MRI
Respiratory correlated 4D-MRI has the potential to be a valuable tool in radiotherapy. This work aims to optimise and validate a 4D-MRI golden angle stack of stars radial sequence for measuring respiratory motion of abdominal organs. A 4D motion phantom is used to compare 4D-MRI against 4D-CT. For craniocaudal movement, motion is underestimated in 4D-MRI but motion estimation improves for non-axial acquisitions. This could be due to the alignment of the motion direction with the cartesian phase encoding direction for axial stack of stars acquisitions.Introduction
Respiratory-correlated 4D-MRI has the potential to be a valuable tool for Radiotherapy (RT) planning, enabling the characterisation of 3D motion for both targets and organs at risk1. The advantages of using 4D-MRI over 4D-CT include improved soft tissue contrast and lack of ionising radiation. The aim of this work was to optimise and validate a 4D-MR golden angle stack-of-stars radial sequence against known motion in a 4D motion phantom, and compare against matched 4D-CT. Radial acquisitions will only be robust to motion within the radial plane, and hence the effect of acquisition orientation and slice thickness were explored.Methods
Figure 1 shows the QUASAR MRI4D phantom (Modus Medical Devices, Ontario, Canada) with a sphere insert, the motion of which was programmed for either 1D or 3D motion. 4D-CT were acquired on a Siemens Confidence CT scanner with the Varian respiratory gating system using the clinical protocol with 10 bins (time binning) and 1D motion only.4D-MRI data were acquired on a 1.5T scanner (MAGNETOM Sola, Siemens Healthcare, Erlangen, Germany) using a free-breathing 3D T1 weighted gradient echo stack of stars radial sequence with golden angle increment (StarVIBE)2. Acquisitions were performed for both 1D and 3D motion, with slice thickness as provided by the vendor, and repeated with different slice thickness and orientation (see Table 1). In each case isotropic voxels were reconstructed. For the adjusted protocols, radial views were determined by the equation (2 x base resolution x number of bins) to ensure adequate data sampling. All 4D-MR data were reconstructed in 5 respiratory phases (amplitude binning with equal number of radial views per phase/bin).
The 4D-MR and 4D-CT data were imported into RayStation Treatment Planning system (RaySearch, Stockholm, v11B), and the sphere outlined on each MR image using the threshold tool at 50% of the maximum intensity value. For CT images, the sphere was outlined using the region growing tool and a lower -200HU threshold limit. Motion was assessed by analysing the centre of mass (COM) coordinates of the sphere. 4D-MR data were also obtained for one healthy volunteer after giving written informed consent (approved by an Institutional Review Board), and the dome of diaphragm motion measured in RayStation by clinical oncologists.
Results
Figure 2 compares respiratory phase images from the 4D-MR and 4D-CT for the 1D breathing trace. Figure 3 shows the COM motion, extracted from all 4D data sets for the 1D trace.The 4D-CT data shows a peak-to-peak range of 29.3mm, an underestimation of 2.4%, 0.7mm. The 4D-MR data shows greater motion underestimation, ranging between 13-25% (4-7.5mm) for the 1D trace, greater than the theoretical 6% underestimate expected due to the intra-bin motion. Figure 4(a) summarises the results for the 1D trace, and figure 4(b) shows the results for the 3D trace. For all motion directions, the non-axial acquisitions show the least motion underestimation, between 5 and 25%.
The diaphragm motion estimated from the volunteer data, showed greater motion for coronal compared to axial acquisitions (11.6mm and 8.4mm for the liver dome respectively).
Discussion & Conclusion
A 4D-MRI StarVIBE sequence was investigated using a motion phantom and matched 4D-CT. Results showed that COM phantom motion is generally underestimated in 4D-MRI when compared to known motion and 4D-CT.There are a few potential reasons for the underestimation of motion seen in the 4D-MRI. One component is the residual intra-bin motion, however this was simulated and explains only 6% (see Figure 4a). This component could be reduced by increasing the number of bins, but this leads to increased acquisition times required to satisfy data sampling3. Five bins were chosen for the 4D-MRI experiment which corresponded to a realistic 5min acquisition time and is consistent with published literature3.
Image resolution in the direction of motion is an additional factor, however, no clear improvement was observed with reduced slice thickness.
The improved results seen for the coronal and sagittal acquisitions indicate that for this sequence, the orientation of the acquisition has a large influence. Motion is expected to be predominantly in the craniocaudal plane within the abdomen, this suggests that non-axial planes should be used clinically for robust estimation of motion, if no motion-compensated image reconstruction is available4.
Validation of 4D-MRI is essential for accurate use of the motion information in RT treatment planning. This work has highlighted the difference between the 4D-MRI and 4D-CT reconstructions. It is important to recognise that 4D-CT and 4D-MRI are not directly comparable; the 4D-MRI reconstruction uses data over multiple respiratory cycles, resulting in an estimation of the average breathing motion, whereas the CT reconstruction is a snapshot of motion. The amplitude binning used for 4D-MRI does not distinguish between inhale and exhale, so it cannot capture any hysteresis of the respiration cycle. Moreover, the residual intra-bin motion for all the MRI phases must be recognised if the images are intended to be used directly as mid-ventilation planning, or to create planning structures such as Internal Target Volumes1. Other approaches such as using the 4D deformation vector fields to align other MRI contrasts may improve image quality4. Further work will include matched patient 4D-CT and 4D-MR comparison using the optimised clinical sequence.
Acknowledgements
This abstract represents independent research supported by the National Institute for Health and Care Research (NIHR) Biomedical Research Centre and the Clinical Research Facility in Imaging at The Royal Marsden NHS Foundation Trust and the Institute of Cancer Research, London. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. This work was supported by the Institute of Cancer Research and Cancer Research UK (CRUK) grant number C33589/A28284.References
- Stemkens B et al., 2018, Physics in Medicine & Biology, 63
- Perkins et al., 2021, Physics and Imaging in Radiation Oncology, 17
- Grimm R et al., 2015, Medical Image Analysis, 19
- Freedman et al., 2017 Investigative Radiology, 52
Figures
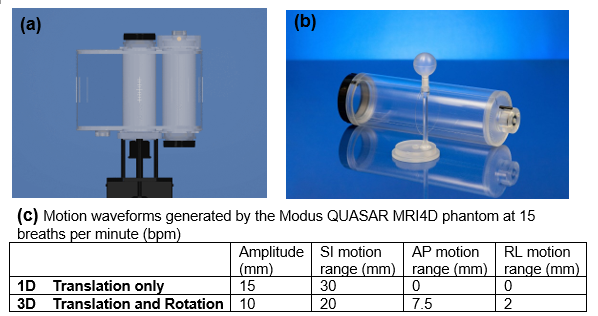
Figure 1: Modus QUASAR MRI4D phantom showing the
body phantom (a) and movable cylindrical insert with offset 3.2cm diameter
sphere (b). The body and cylinder were filled with water, and sphere filled
with CuSO4. (c) motion waveforms used for the experiment to simulate 1D and 3D
motion. Images from website modusqa.com.
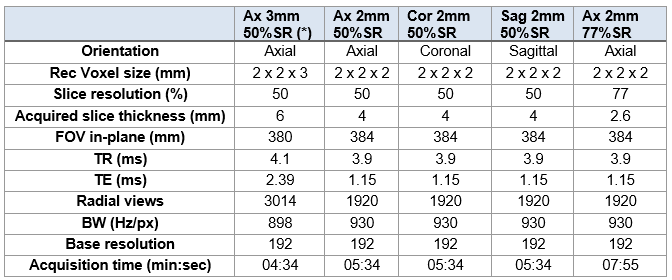
Table 1:
Default and adjusted protocol parameters for self-gated StarVIBE (* denotes the
sequence with the default slice resolution parameters)
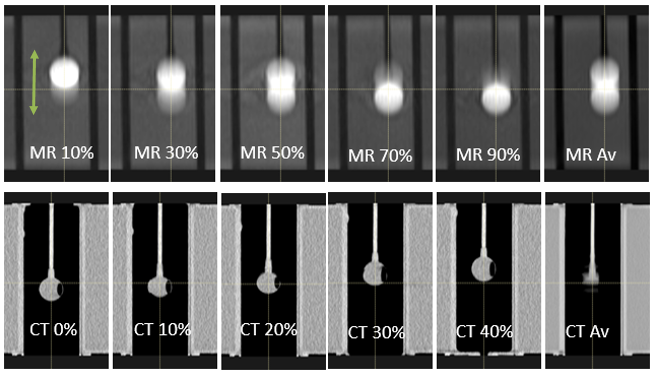
Figure
2: Comparison of respiratory phases in
the coronal view from the 1D motion trace with motion in SI direction (shown
with green arrow). Top row: 4D-MR (5 bins + average. Bottom row: 4D-CT (5 bins
shown from 10 bin reconstruction, + average). The MR bins show artefacts from
the residual motion within each bin. The 4D-MR was acquired axially. Note that the bins are
not directly comparable between MR and CT due to different binning reconstructions. Bins 50%-90% are not shown for the 4D-CT.
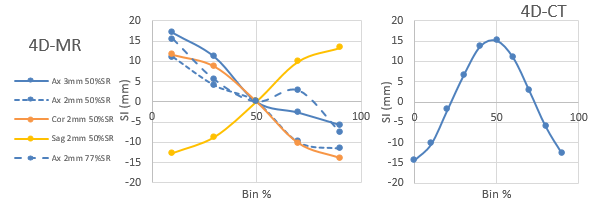
Figure 3: Sphere SI COM for the 4D-MR and 4D-CT
acquisitions with the 1D breathing trace. This illustrates the difference in the binning reconstruction, with 4D-MR
showing an inspiration-expiration cycle, and 4D-CT a complete
expiration-expiration cycle. The 4D-MR
data are referenced to the 50% COM for inter-comparison.
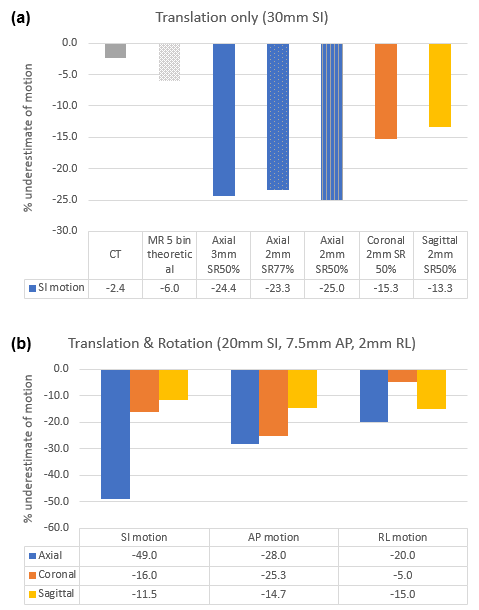
Figure 4: Peak to peak COM motion
underestimation for (a) 1D Trace. (b) 3D Trace. The % underestimate is calculated
in reference to the nominal phantom motion range indicated in the title of each
plot. In (a) the theoretical MR 5 bin
underestimation is from simulation of the average position in each bin for
sinusoidal motion, assuming time binning and equal number of views in each
bin.
DOI: https://doi.org/10.58530/2023/2020