1996
View-Sharing and KWIC Filtering Achieves High Spatio-Temporal Resolution in 32-Fold Accelerated Real-Time Cardiac Cine with Radial Sampling1Department of Biomedical Engineering, Northwestern University, Evanston, IL, United States, 2Department of Radiology, Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 3Department of Pediatric, Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 4Division of Cardiology, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States, 5Department of Medical Imaging, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States
Synopsis
Keywords: Cardiovascular, Image Reconstruction
Highly-accelerated real-time cine MRI is a rapid technique that is particularly useful for patients with arrhythmia, dyspnea, and/or pediatric patients who may not be able to follow breath-hold instructions. Incorporating view-sharing (VS) and k-space weighted image contrast (KWIC) filtering into a compressed sensing (CS) reconstruction framework improves spatio-temporal resolution in our 32-fold accelerated real-time free-breathing cine MRI using radial k-space sampling. Resulting biventricular volumetric parameters are relatively accurate, which may eliminate the need for sedation/anesthesia in pediatric patients.
Introduction
Highly-accelerated real-time cine MRI is a rapid technique that is particularly useful for patients with arrhythmia, dyspnea, and/or pediatric patients who may not be able to follow breath-hold instructions. Our previous study demonstrated that radial k-space sampling and compressed sensing achieves 12 to 16-fold acceleration and relatively accurate left ventricular functional parameters in adults1. Imaging pediatric patients is technically challenging because their hearts are smaller and beat much faster. We sought to develop and evaluate a 32-fold accelerated real-time free-breathing cine MRI using radial k-space sampling with view-sharing (VS) and k-space weighted image contrast (KWIC) filtering2, for the purpose of achieving high spatio-temporal resolution and accurate biventricular volumetric parameters in pediatric patients.Methods
Human Subjects & Pulse Sequence: We retrospectively identified 14 pediatric patients with congenital heart disease (CHD) (mean age = 9±2 years, 13/1 males/females) who underwent a standard breath-hold cine acquisition and real-time free-breathing cine using radial k-space sampling pattern with tiny golden angle sequence = 32.04° (N = 5) 1. To achieve high temporal resolution for pediatric patients, we reconstructed each time frame using 6 radial spokes, which achieves 32-fold acceleration. Relevant image parameters were summarized in Table 1.Image reconstruction: Figure1a illustrates three different image formation schemes: default CS with 6 radial spokes per frame; CS with VS 18 (9 before and after native) adjacent radial spokes, and CS with VS and KWIC filtering to exclude the center of k-space in VS radial spokes. To accelerate image reconstruction, coil compression was used to produce eight virtual coils 3, and gpuNUFFT was applied throughout the reconstruction pipeline 4. We used temporal total variation (TTV) and temporal PCA (TPCA) as the two orthogonal sparsifying transforms using empirically derived optimal regularization weights.
Image quality analysis: For quantitative evaluation, we calculated the blur metric 5 and bi-ventricular volumetric parameters (EDV, ESV, SV and EF). For blur metric calculation, we limited the analysis to the heart region by manually cropping the FOV. Cardiac contours were segmented using the automatic AI tools followed by manual correction in Circle CVI42. For qualitative evaluation, two clinical readers independently graded the images using a 5-point Likert scale (See Table 2). We tested for parameter normality using the Shapiro-Wilk test. We compared the blur metric calculated from the clinical standard cine, real-time cine with CS alone, CS with VS, and CS with VS and KWIC filtering using one-way ANOVA with Bonferroni correction as the post hoc test. We compared visual scores and biventricular volumetric parameters between clinical standard cine and real-time cine - the group with the smallest blur metric (i.e., winner) - using two-tailed, paired t-test (Wilcoxon signed-rank, if not normally distributed). In addition, linear-regression and Bland-Altman analyses were conducted on biventricular volumetric parameters to determine the coefficient of determination (R2) and levels of agreement. A p < 0.05 was considered statistically significant for each statistical test.
Results
According to the Shapiro-Wilk test, the blur metric and biventricular volumetric parameters were normally distributed (statistic: [0.1, 1]), whereas the visual scores were not normally distributed (p < 0.05). Figure 1b shows representative cine images: clinical standard, real-time with CS alone, CS with VS, and CS with VS and KWIC filtering. Among real-time reconstructions, incorporating VS+KWIC produced the best image quality as shown. As summarized in Table 2, VS with KWIC filtering significantly (p<0.05) reduced the blur metric (0.39±0.03) compared with VS alone (0.44±0.03) and default CS (0.51±0.03). Thus, we used CS with VS+KWIC for visual and biventricular volumetric parameters comparison with clinical standard cine. The median conspicuity of endocardial border, temporal fidelity of wall motion, and artifact scores were not significantly different, whereas the noise score was significantly different. Nonetheless, all scores were above the clinically acceptable (3.0) cut point. There were no significant differences in biventricular volumetric parameters (p>0.05) except for the RV EDV and RV SV (p<0.05). As shown in Figure 2, linear regression showed a strong correlation (R2>0.85) between clinical standard cine and real-time cine with VS and KWIC filtering for all categories. Bland-Altman analysis (Figure 3) showed the following results: LV ventricular volumetric parameters (absolute mean-difference ≤ 0.38 ml for EDV, ESV and SV, absolute mean-difference = 0.34% for EF), RV ventricular volumetric parameters (absolute mean-difference ≤ 4.81ml for EDV, ESV and SV, absolute mean-difference = 0.73% for EF).Conclusion
32-fold accelerated real-time free-breathing cine MRI with radial k-space sampling, VS, and KWIC filtering produces good image quality and relatively accurate biventricular volumetric parameters in pediatric patients, which may eliminate the need for sedation/anesthesia.Acknowledgements
This work is supported by National Institutes of Health (R01HL116895, R21AG055954, R01HL151079, R21EB030806A1) and American Heart Association (19IPLOI34760317, 949899, 903375).References
1. Haji-Valizadeh H, Rahsepar AA, Collins JD, Bassett E, Isakova T, Block T, Adluru G, DiBella EVR, Lee DC, Carr JC and Kim D. Validation of highly accelerated real-time cardiac cine MRI with radial k-space sampling and compressed sensing in patients at 1.5T and 3T. Magn Reson Med. 2018;79:2745-2751.
2. Song HK and Dougherty L. k-space weighted image contrast (KWIC) for contrast manipulation in projection reconstruction MRI. Magn Reson Med. 2000;44:825-32.
3. Huang F, Vijayakumar S, Li Y, Hertel S and Duensing GR. A software channel compression technique for faster reconstruction with many channels. Magn Reson Imaging. 2008;26:133-41.
4. Knoll F, Schwarzl A, Diwoky C and Sodickson DK. gpuNUFFT-an open source GPU library for 3D regridding with direct Matlab interface. In: Proceedings of the 22rd Annual Meeting of ISMRM, Melbourne, Australia 2014. Abstract No. 4297.
5. Crete F DT, Ladret P, Nicolas M. The blur effect: perception and estimation with a new no-reference perceptual blur metric. SPIE. 2007.
Figures
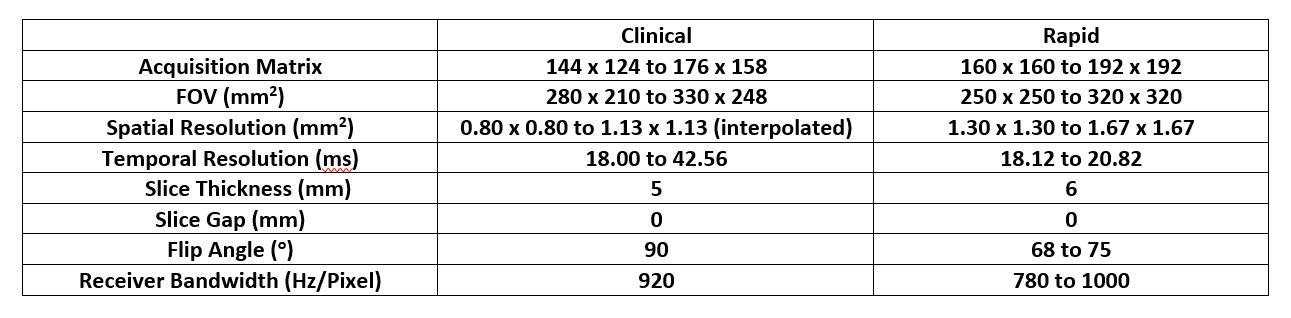
Table 1 Summary of relevant pulse sequence parameters.
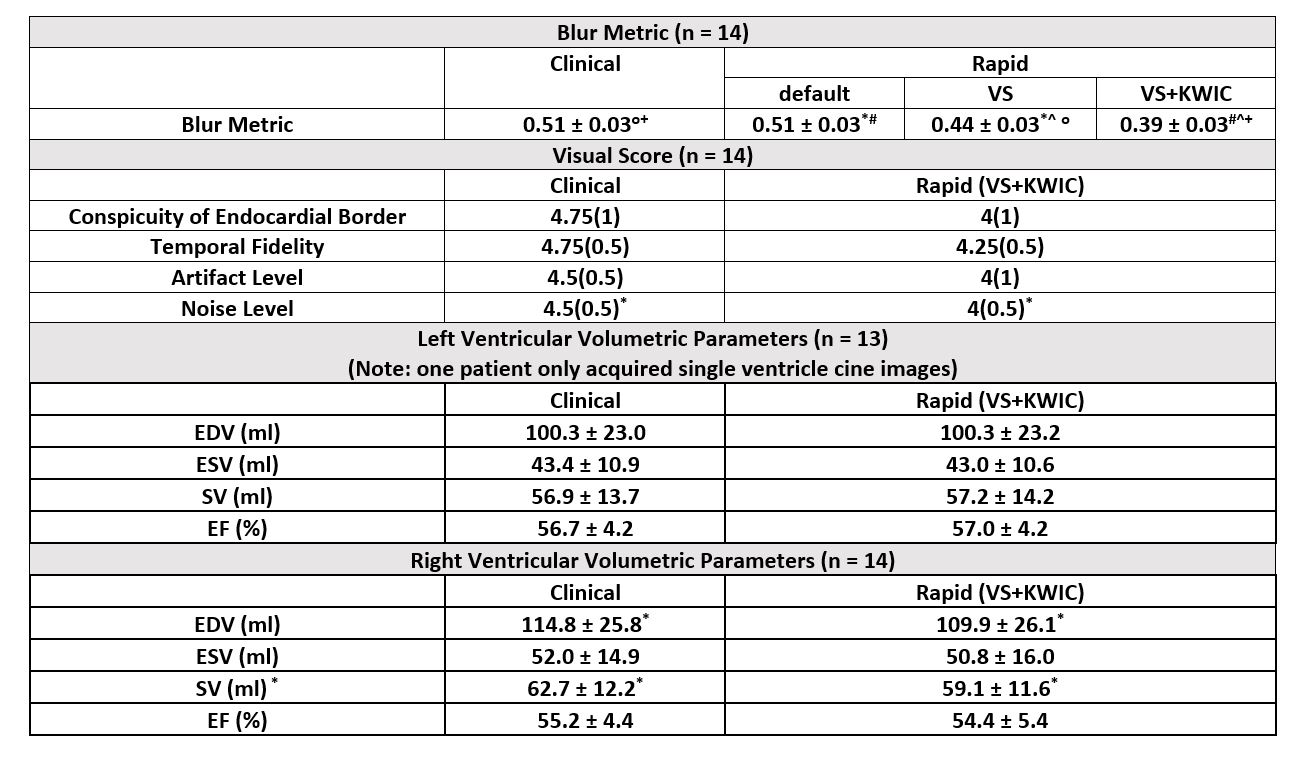
Table 2 Summary of the blur metric, visual scores and biventricular volumetric parameters. The blur metric and biventricular volumetric parameters are presented as means ± standard deviations. The visual scores are presented as medians (interquartile ranges [IQR]). The conspicuity of endocardial border and temporal fidelity: 1 = nondiagnostic; 2 = poor; 3 = clinically acceptable; 4 = good; 5 =excellent. Noise and artifact levels: 1 = nondiagnostic; 2 = severe; 3 = moderate; 4 = mild; 5 = minimal. O+*#^P < 0.05 was considered statistically significant.
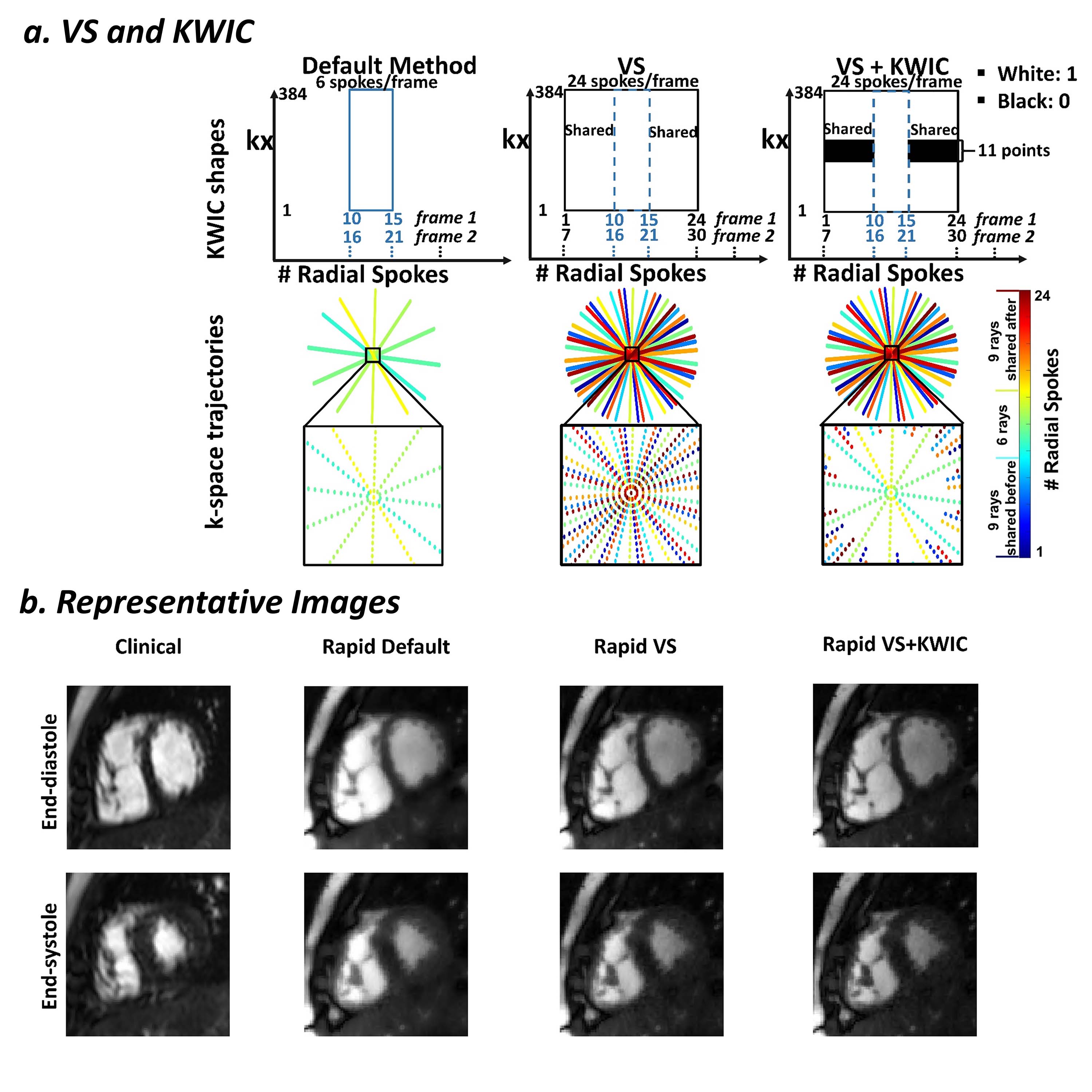
Figure 1 (a) A schematic describing how view-sharing (VS) and k-space weighted image contrast (KWIC) filtering are incorporated into a compressed sensing (CS) framework. (b) Representative images from one patient. From left to right: clinical cine images, rapid cine images reconstructed by default CS, CS with VS and CS with VS+KWIC.
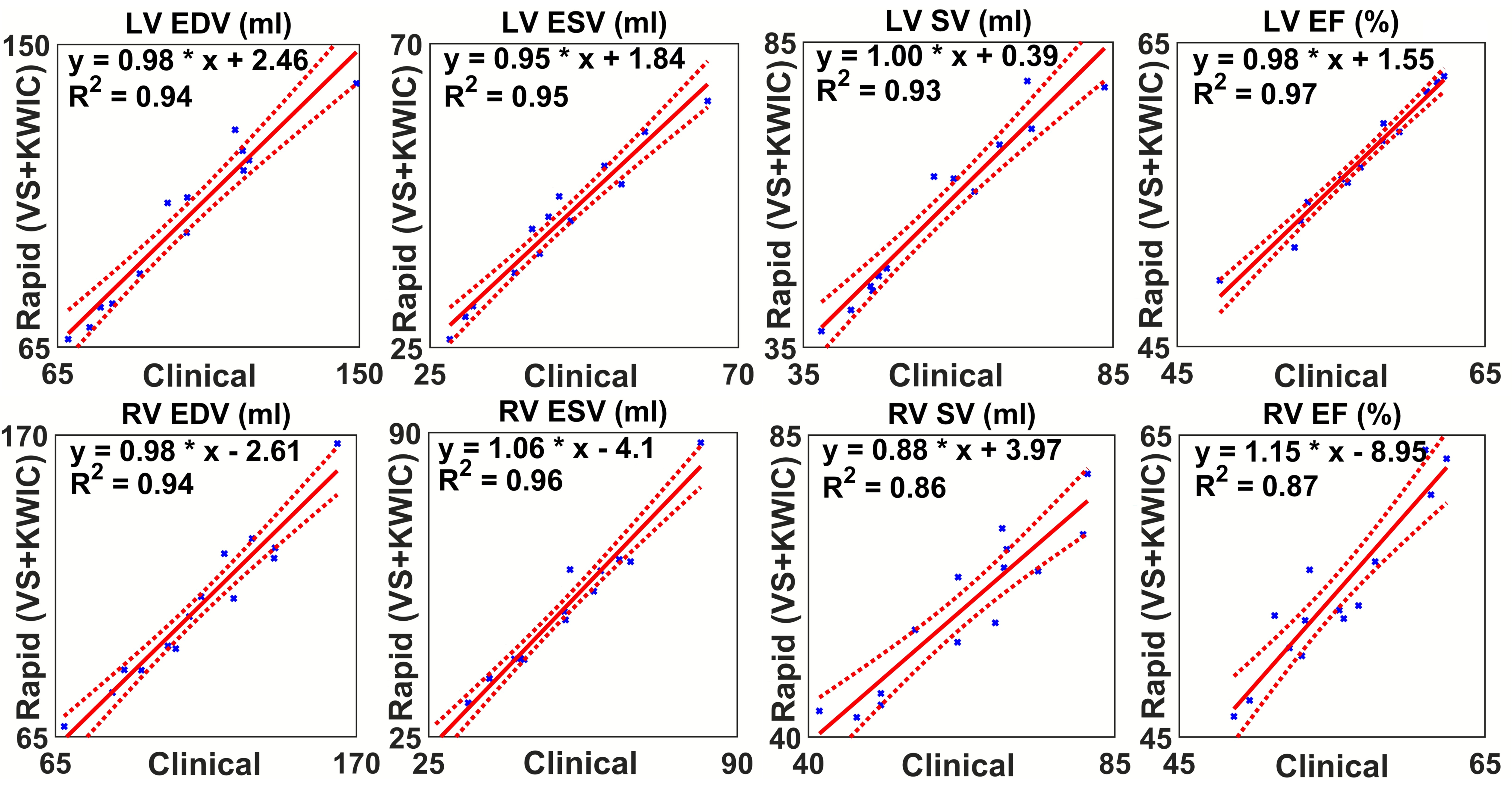
Figure 2 Linear regression results over all cases for 32-fold accelerated real-time free-breathing cine MRI reconstructed with compressed sensing (CS), view-sharing (VS) and k-space weighted image contrast (KWIC) filtering compared to clinical standard breath-hold cine for biventricular volumetric parameters.
Figure 3 Bland-Altman plots for 32-fold accelerated real-time free-breathing cine MRI reconstructed with compressed sensing (CS), view-sharing (VS) and k-space weighted image contrast (KWIC) filtering compared to clinical standard breath-hold cine for biventricular volumetric parameters.