1994
Comparison of SAR Distributions around Epicardial and Endocardial Electrodes in Growing Pediatric Patients with Cardiac Pacemakers1Tokai University, Kanagawa, Japan, 2GE Healthcare, Waukesha, WI, United States, 3Department of Pediatrics, The University of Tokyo Hospital, Tokyo, Japan
Synopsis
Keywords: Safety, Safety
RF-induced SAR distributions around epicardial lead were compared with endocardial lead in the 29-month-old and 6-year-old pediatric anatomical models with cardiac pacemakers. Numerical simulations were performed with a 1.5-T birdcage coil and the pacemaker models segmented from the age-matching patient CT data. In both pediatric models, the simulation with the endocardial lead overall showed lower SAR values compared to that with the endocardial lead. The screw-like electrode attached to the endocardial lead may have resulted in much higher SAR values, compared to the tined-type electrode of the epicardial lead.Introduction
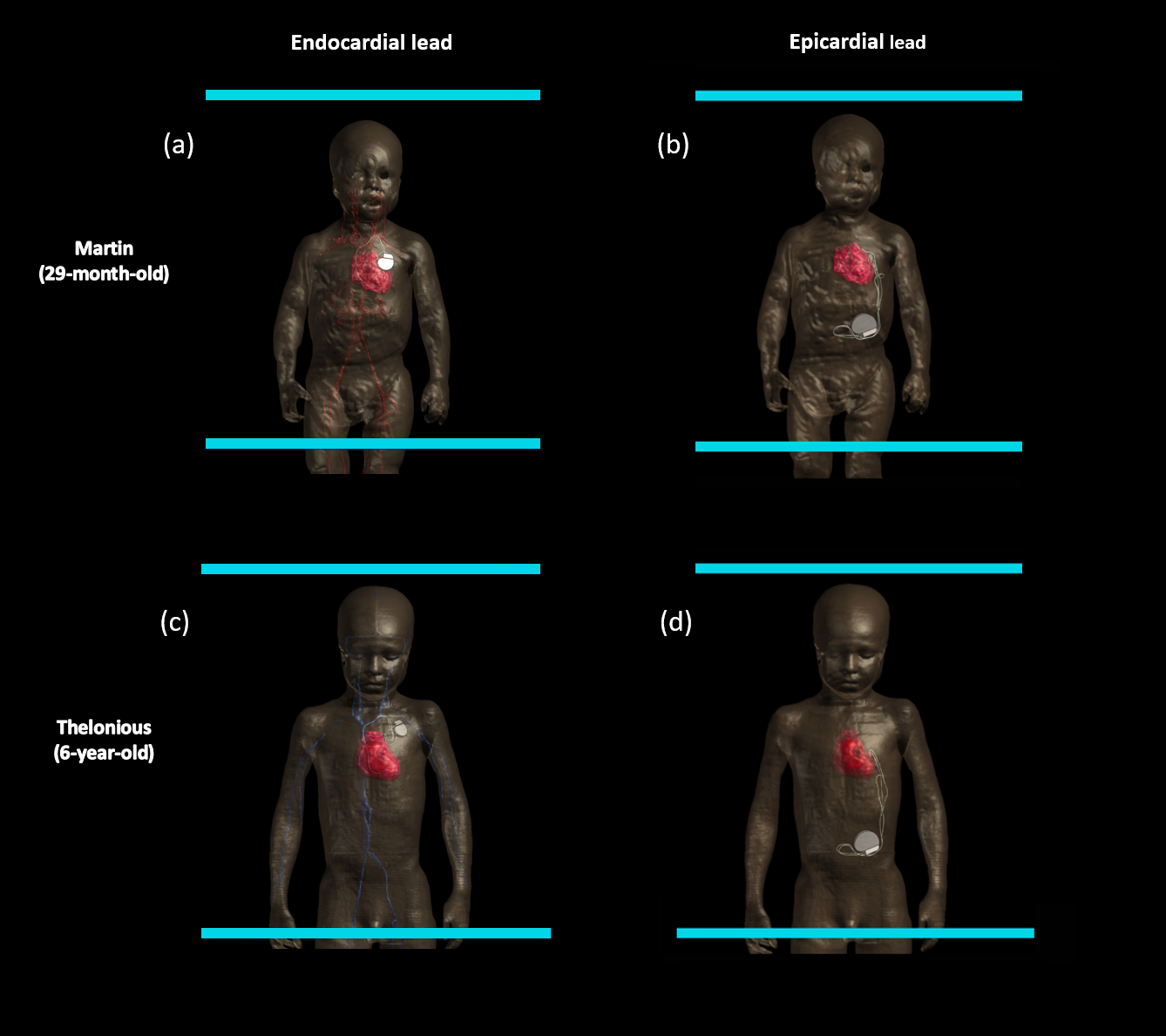
Pacemakers with endocardial leads are often used for adult patients with cardiac dysfunction. The endocardial leads have screw-type electrodes that are implanted in the myocardium via the subclavian vein. For pediatric patients, this approach may not be optimal as it can block the narrow vessels. Instead, epicardial leads with tined-type electrodes are sewn on the epicardium and the pacemaker generators are placed in the abdominal cavity to leave some space for the body growth. Jiang et al. showed the RF-induced heating of the epicardial leads with a 29-month-old anatomical human model at 1.5 T1; however, heating effect is unknown when the patient grows up and the lead trajectory changes inside the body. This adds another unknown factor to the RF-induced heating risk that varies depending on the physical characteristics of the patients2. In this study, specific absorption rate (SAR) distributions were compared between two lead types (epicardial and endocardial) in two pediatric models (26 months old and 6 years old).Methods
The Sim4Life platform (V7.0.2.10006, Zurich Med Tech, Switzerland) was used to simulate electromagnetic (EM) fields using the finite difference time domain method (FDTD). The 29-month-old MARTIN model3 (height: 86.1 cm, weight: 13 kg and 86 anatomical structures) and the 6-year-old Thelonious model4 (height: 116 cm, weight: 18.6 kg, and 81 anatomical structures) were placed inside the 1.5T highpass birdcage resonator with the eight legs as current sources. The imaging landmark was set at the heart. The pacemakers and lead trajectories were segmented from the CT data of age-matching patients and modeled into the heart of the pediatric models as shown in Fig. 1. The Huygens’ source was utilized, and the results were scaled with B1+ = 1μT. The SAR values were compared with epicardial and endocardial leads.Results
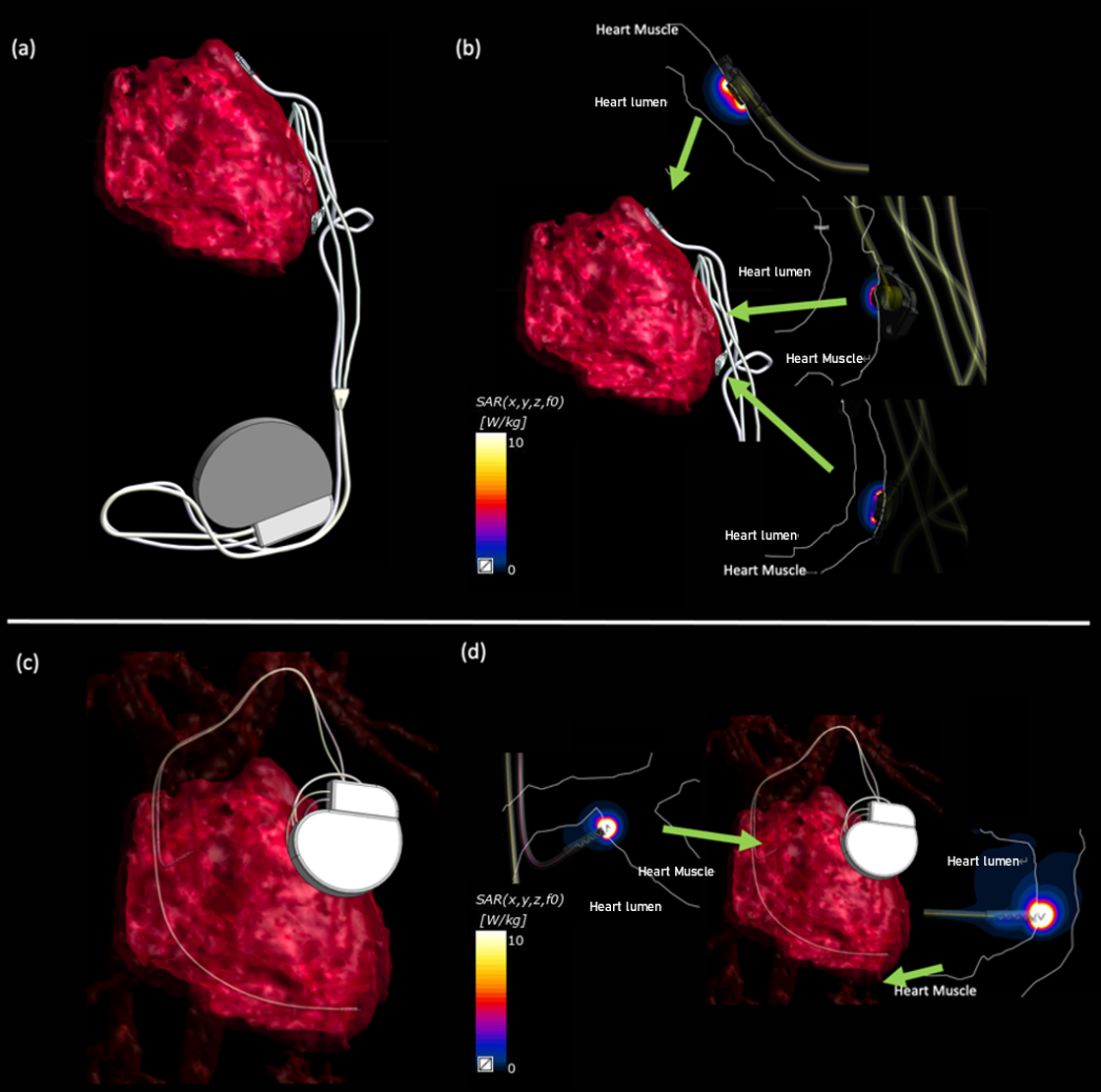
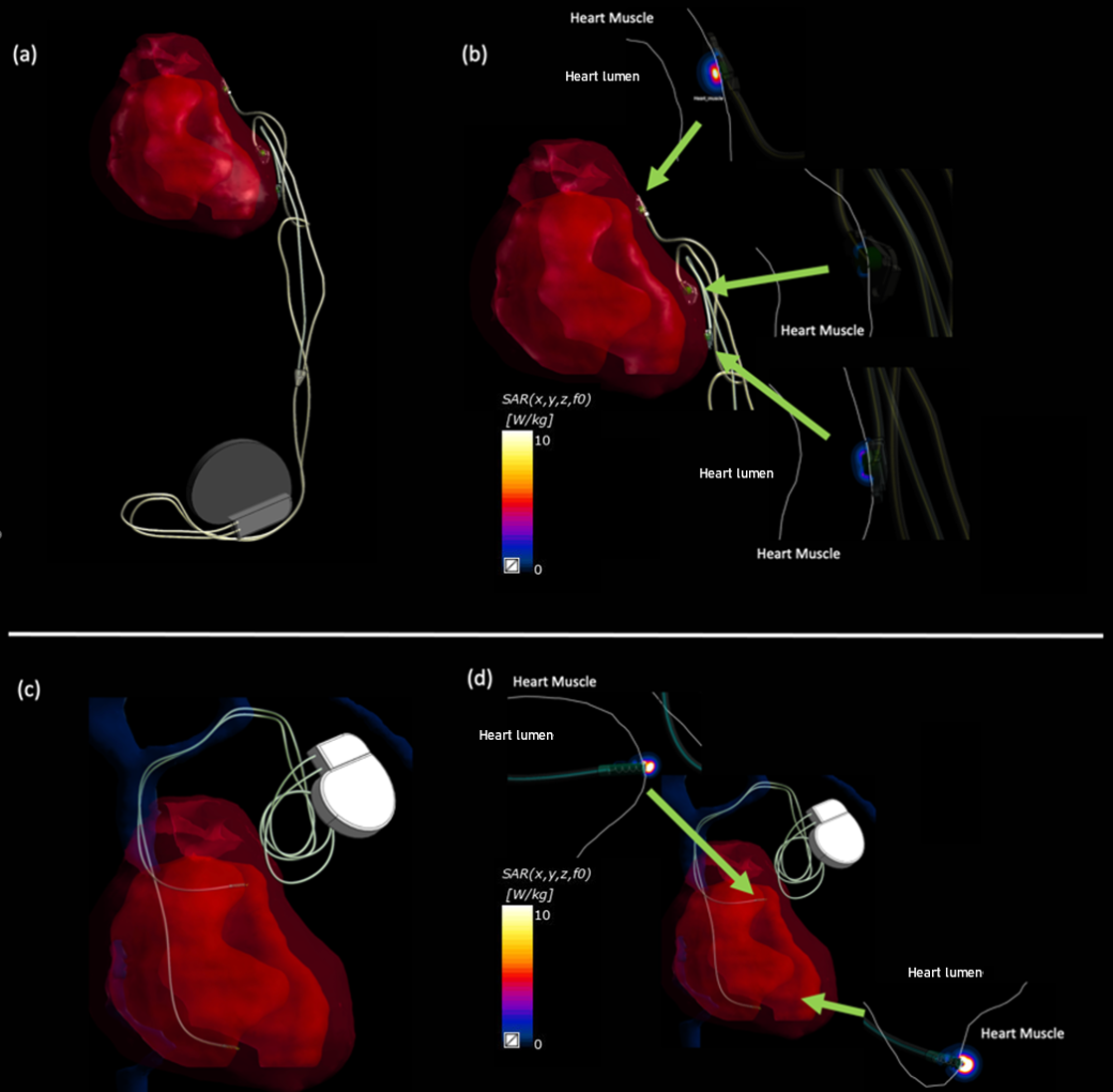
High SAR values were found in heart muscles for both epicardial and endocardial leads with both pediatric models [Fig. 2 and 3]. The highest SAR value was found in the right ventricle of the 29-month-old model with the endocardial lead (105 W/kg). The peak SAR value in the right atrium was approximately 69% lower than that in the right ventricle. The epicardial lead results showed much lower SAR in the left atrium (89% lower), in the left ventricular apex (84% lower) and in the left ventricle (93% lower) compared to the highest SAR from the endocardial lead simulation. For the simulations with the 6-year-old model, the highest SAR value was found in the right atrium (20 W/kg) with the endocardial lead. The peak SAR value in the right atrium was approximately 40% lower than that in the right ventricle. The epicardial lead results showed lower SAR in the left atrium (35% lower), in the left ventricular apex (93% lower) and in the left ventricle (77% lower) compared to the highest SAR from the endocardial lead simulation.Discussion and Conclusions
For both pediatric models, the higher SAR values were observed with the endocardial lead. The pointed shape of the electrode may have contributed to the result. On the contrary, the epicardial lead electrode has a larger surface area. Although the SAR values were lower, there may be a wider area with high SAR values. More investigations are needed to confirm that there is no thermal damage to the myocardial nervous system.In this study, the idealized coil was used, and the simulation was performed at the heart landmark. SAR values may be different with a realistic resonator such as a quadrature birdcage coil and at different imaging landmarks5. In addition, the lead trajectory was modeled based on the age-matching patient CT data; however, the trajectory patterns vary among patients. Further investigations are needed to confirm the various clinical scenarios.Lastly, growth-accommodating implants have been demonstrated6,7. Although they are not available for pacemakers, the growth-accommodating lead trajectory may enable more scanning of pediatric patients with implantable devices.Acknowledgements
No acknowledgement found.References
1. Jiang F, et al. A small loop makes a big difference: Modifying trajectory of epicardial leads substantially reduces RF heating of CIEDs in children during 1.5T MRI. Proc. ISMRM. Joint Annual Meeting ISMRM-ESMRMB & ISMRT 31st Annual Meeting, 2022.
2. Murbach M, et al. Whole-body and local RF absorption in human models as a function of anatomy and position within 1.5 T MR body coil. Magn Reson Med. 2014; 71:839-845.
3. Jeong, H et al. Development, validation, and pilot MRI safety study of a high-resolution, open source, whole body pediatric numerical simulation model. Plos one. 2021; 16(1), e0241682.
4. Christ, A et al. The Virtual Family—development of surface-based anatomical models of two adults and two children for dosimetric simulations. Physics in Medicine & Biology. 2009; 55(2), N23.
5. Fujimoto K, et al. Effect of Simulation Settings on Local Specific Absorption Rate (SAR) in Different Anatomical Structures. Proc. ISMRM. Workshop on Ensuring RF Safety in MRI: Current Practices & Future Directions, 2017.
6. Feins, EN, et al. A growth-accommodating implant for paediatric applications. Nature biomedical engineering. 2017; 1.10: 818-825.
7. Feins, EN, and Sitaram ME. Expandable valves, annuloplasty rings, shunts, and bands for growing children. Seminars in Thoracic and Cardiovascular Surgery: Pediatric Cardiac Surgery Annual. 2020; Vol. 23.
Figures