1990
Volumetric flow assessment in fetal sheep with Cartesian 4D flow MRI and radial slice-to-volume flow MRI with and without blood pool contrast1Translational Medicine, The Hospital for Sick Children, Toronto, ON, Canada, 2Radiology, Nationwide Children’s Hospital, Columbus, OH, United States, 3Center for Regenerative Medicine, Nationwide Children’s Hospital, Columbus, OH, United States, 4Cardiology, Nationwide Children’s Hospital, Columbus, OH, United States, 5The Heart Center, Nationwide Children’s Hospital, Columbus, OH, United States, 6Pediatrics, University Hospitals Rainbow Babies & Children’s Hospital, Cleveland, OH, United States, 7OB/GYN-Maternal Fetal Medicine, University Hospitals Cleveland Medical Center, Cleveland, OH, United States, 8Medical Biophysics, University of Toronto, Toronto, ON, Canada
Synopsis
Keywords: Fetal, Fetus
We compare flow distributions in fetal sheep obtained with Cartesian 4D flow MRI and slice-to-volume multidimensional blood flow imaging using accelerated multislice radial phase contrast MRI. In the latter, stacks of 2D slices are imaged. Real-time reconstructions allow for in-plane motion correction. CINEs are combined into a dynamic flow sensitive volume using slice-to-volume reconstruction with interslice motion correction. Comparison is performed in the presence and absence of contrast agent.Introduction
Fetal development depends on a complex circulatory system [1]. Accurately assessing flow distribution and visualizing the circulatory system are important for understanding pathologies and potential therapies.In this work, we compare Cartesian 4D flow MRI with multidimensional radial slice-to-volume (SVR) phase contrast (PC) MRI in fetal sheep subjects [2]. Fetal MRI faces challenges such as sporadic motion and requires high spatiotemporal resolutions to account for small cardiac structures and high heart rates. Cartesian 4D flow MRI provides volumetric multidimensional flow measurements; however, they are susceptible to motion artifacts and suffer from poor signal-to-noise ratio [3]. There is no information on the ability of blood pool contrast agent to improve image quality in fetuses. Radial SVR PCMRI consists of imaging multiple 2D slices which are combined into an isotropic volume retrospectively. It provides avenues for compensating for fetal motion through intermediate real-time reconstruction and interslice registration [2]. It also provides high signal in vessels owing to in-flow effects, potentially rendering such vessels more conspicuous than in 4D flow MRI.
Methods
Singleton fetuses in 3 pregnant sheep between 108-110 days gestation (150d term) were scanned under free breathing conditions on a clinical 3T MRI system (Prismafit, Siemens Healthineers). One (Sheep 1) had blood pool contrast agent, Feraheme, injected into the umbilical vein prior to the MRI. Dosing was 3 mg/kg, with fetal/placental weight calculated as 3 kg. All sheep were sedated with Fentanyl and Atropine for the procedure.All scans were Doppler ultrasound (DUS) gated (Smart-Sync, Northh Medical). Cartesian 4D flow MRI was performed in Sheep 1 and 3, and not attempted in Sheep 2. Imaging parameters are summarized in Figure 1A. Radial SVR PCMRI was performed in all 3 fetuses, as in [2]. Briefly, real-times frames were first reconstructed for motion compensation. Velocity sensitive CINEs were then reconstructed using the DUS gating log. These CINEs were combined into a volume using SVR with isotropic resolution of 1 mm. This pipeline is summarized in Figure 1B.
Volumetric flows were assessed using prototype software (4D Flow v2.4, Siemens [4]). Particle traces were generated to visualize blood flow. Dynamic angiograms were computed through the product of the magnitude and speed, then visually analyzed for conspicuity of vasculature and adequacy of segmentation of cardiac anatomy. Peak and mean flows from Cartesian 4D flow MRI and radial SVR PCMRI were each compared against reference 2D Cartesian PCMRI acquired from fetal great vessels: inferior vena cava (IVC), superior vena cava (SVC), descending aorta (DAO), ascending aorta (AAO) and main pulmonary artery (MPA). Above comparisons were made in fetuses with and without contrast agent.
Results and Discussions
Adequate visualization and segmentation of anatomy was achieved using radial SVR PCMRI in all 3 sheep, but using Cartesian 4D flow MRI only in Sheep 1 (with contrast). Segmentation of the Cartesian 4D dataset failed in Sheep 3 (without contrast).Figure 2 depicts hemodynamics in the fetal hearts through particle traces. In Sheep 1, both Cartesian 4D flow MRI and radial SVR PCMRI depict preferential flow from the IVC into the left side of the heart and low flow in the MPA. Particle traces from radial SVR PCMRI in Sheep 2 depict the heart in a top-down view with blood streams from the MPA and AAO merging into the DAO.
Figure 3 depicts particle traces at different timepoints, originating from planes in the SVC and IVC of Sheep 2. Oxygenated ductus venosus blood enters the left side of the heart and feeds the upper and lower body. Deoxygenated blood from the distal IVC and SVC enters the right side of the heart and primarily exits through the MPA en route to the lower body and placenta, as shown in previous studies [2],[5].
Figure 4 shows dynamic angiograms from all volumetric acquisitions. The blood vessels and cardiac anatomy were more conspicuous in the radial SVR PCMRI, which benefited from blood signal enhancement from in-flow effects. For Cartesian 4D flow, the angiogram in Sheep 1 (with contrast agent) had better visualization of the heart and blood vessels than in Sheep 3 (lacking contrast agent).
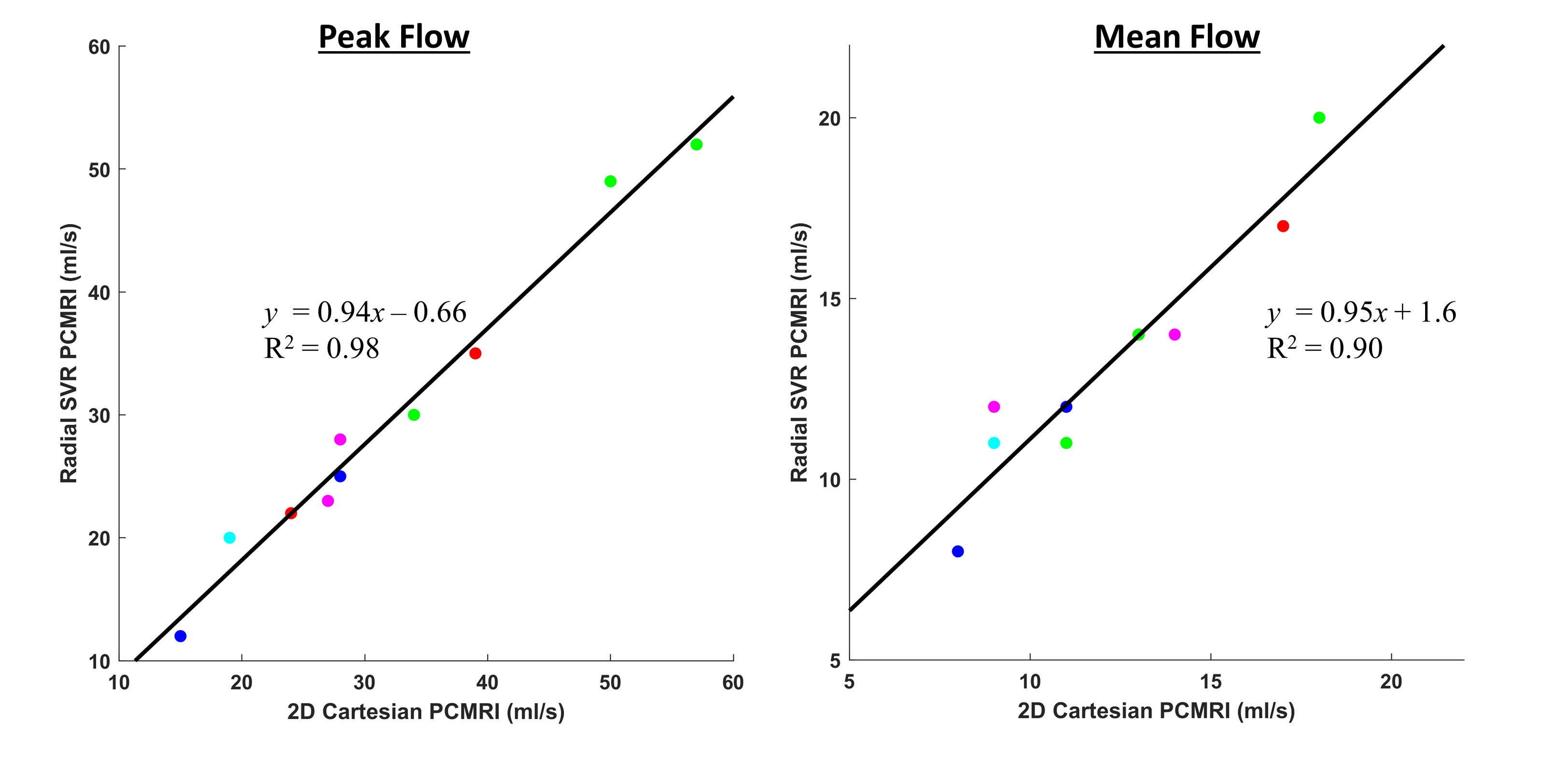
Figure 5 depicts good agreement between the peak and mean flows from radial SVR PCMRI versus the reference 2D Cartesian PCMR, with absolute errors of 9 ± 6 % and 9 ± 11 %, respectively. In the presence of contrast agent, the absolute errors in the peak and mean flows with Cartesian 4D flow MRI, relative to 2D Cartesian measurements, were 9 ± 2 % and 17 ± 6 %, respectively. However, in absence of contrast, vessel localization was challenging with poor signal and the corresponding errors were 65 ± 19 % and 57 ± 13 %. In Sheep 1, Cartesian 4D flow MRI deviated from radial SVR PCMRI in peak and mean flows by 8 ± 8 % and 14 ± 15 %, respectively.
Conclusion
Volumetric flow measurements in fetuses were performed with and without blood pool contrast agent. Cartesian 4D flow performed well only in presence of contrast agent. Radial SVR PCMRI provides robust image quality for volumetric flow measurements, even when intravascular contrast agent administration is not feasible.Acknowledgements
Christopher Macgowan and Rajesh Krishnamurthy have joint senior authorship.
References
[1] A. Rudolph, Congenital Diseases of the Heart: Clinical-Physiological Considerations. John Wiley & Sons, 2011.
[2] D. S. Goolaub, J. Xu, E. M. Schrauben, D. Marini, J. C. Kingdom, J. G. Sled, M. Seed, and C. K. Macgowan, “Volumetric Fetal Flow Imaging with Magnetic Resonance Imaging,” IEEE Transactions on Medical Imaging, pp. 1–1, 2022.
[3] M. Markl, A. Frydrychowicz, S. Kozerke, M. Hope, and O. Wieben, “4D flow MRI,” Journal of Magnetic Resonance Imaging, vol. 36, no. 5, pp. 1015–1036, 2012.
[4] M. A. Gulsun, M.-P. Jolly, J. Guehring, C. Guetter, A. Littmann, A. Greiser, M. Markl, and A. F. Stalder, “A Novel 4D Flow Tool for Comprehensive Blood Flow Analysis,” p. 1.
[5] E. M. Schrauben, B. S. Saini, J. R. T. Darby, J. Y. Soo, M. C. Lock, E. Stirrat, G. Stortz, J. G. Sled, J. L. Morrison, M. Seed, and C. K. Macgowan, “Fetal hemodynamics and cardiac streaming assessed by 4D flow cardiovascular magnetic resonance in fetal sheep,” Journal of Cardiovascular Magnetic Resonance, vol. 21, no. 1, p. 8, Jan. 2019.
Figures