1982
Cardiac Magnetic Resonance Imaging at 3T Characterizes the Myocardium for Pediatric Cardiac Transplant Recipients: New Biomarker Development
Margaret M Samyn1, Adam M Gordon2, Ke Yan3, Jian Zhang4, Aspen M Duffin5, Jonathan H Soslow6, Bruce Damon7, Jennifer M Gerardin1, Benjamin M Goot8, Joseph R Cava1, and Steven J Kindel1
1Pediatrics, Medical College of Wisconsin/ Herma Heart Institute at Children's Wisconsin, Milwaukee, WI, United States, 2Medical College of Wisconsin, Milwaukee, WI, United States, 3Pediatrics, Medical College of Wisconsin/ Quantitative Health Sciences, Milwaukee, WI, United States, 4Quantitative Health Sciences, Medical College of Wisconsin/ Quantitative Health Sciences, Milwaukee, WI, United States, 5Herma Heart Institute, Children's Wisconsin, Milwaukee, WI, United States, 6Pediatrics, Vanderbilt Univesity Medical Center, Nashville, TN, United States, 7Bioengineering, Carle Foundation Hospital/University of Illinois, Urbana, IL, United States, 8Pediatrics (Cardiology), Medical College of Wisconsin/ Herma Heart Institute at Children's Wisconsin, Milwaukee, WI, United States
1Pediatrics, Medical College of Wisconsin/ Herma Heart Institute at Children's Wisconsin, Milwaukee, WI, United States, 2Medical College of Wisconsin, Milwaukee, WI, United States, 3Pediatrics, Medical College of Wisconsin/ Quantitative Health Sciences, Milwaukee, WI, United States, 4Quantitative Health Sciences, Medical College of Wisconsin/ Quantitative Health Sciences, Milwaukee, WI, United States, 5Herma Heart Institute, Children's Wisconsin, Milwaukee, WI, United States, 6Pediatrics, Vanderbilt Univesity Medical Center, Nashville, TN, United States, 7Bioengineering, Carle Foundation Hospital/University of Illinois, Urbana, IL, United States, 8Pediatrics (Cardiology), Medical College of Wisconsin/ Herma Heart Institute at Children's Wisconsin, Milwaukee, WI, United States
Synopsis
Keywords: Cardiovascular, Tissue Characterization, Cardiac transplant; 3Tesla; Parametric Imaging
Pediatric heart transplant recipients undergo frequent invasive cardiac catheterization with endomyocardial biopsy for routine allograft surveillance. Risks associated with catheterization and sampling error call into question this accepted “gold standard.” Cardiac magnetic resonance imaging (CMR), with parametric imaging, may advance myocardial surveillance in this population. Fifty-two pediatric patients (transplanted at ≤18 years old) underwent CMR (September 2016 to June 2019) at 3T to evaluate myocardial health using MOLLI sequence. Healthy transplant recipients had normal global biventricular function, native T1 higher than published values for healthy children at 3T with similar extracellular volume (ECV) despite history of treated rejection.Introduction
Pediatric heart transplant recipients undergo frequent invasive cardiac catheterization with endomyocardial biopsy for routine allograft surveillance. Risks associated with catheterization and sampling error call into question this accepted “gold standard.” Cardiac magnetic resonance imaging (CMR), with parametric imaging, may advance myocardial surveillance in this population.1 This prospective study aimed to systematically review and establish a range of normal myocardial native T1 and myocardial extracellular volume (ECV) values for a large, healthy pediatric heart transplant population undergoing CMR at 3Tesla.Methods
Pediatric patients (transplanted at ≤ 18 years old and ≤ 25 years at study enrollment) underwent CMR (September 2016 to June 2019) at 3T (Siemens Skyra magnet) to evaluate myocardial health. Using a modified Look-Locker (MOLLI) sequence, we assessed myocardial T1 mapping and calculated extracellular volume (ECV) using Circle Cardiovascular (CV42) software.Results
Fifty-two patients (30 males, 58%), median age 2.05 years (IQR 0.43 - 7.16) at transplantation, underwent CMR scanning at 11.94 years of age (IQR 8.77 - 16.45). The donor ischemic time was 225 minutes (IQR 201 - 254). Patients were healthy 7.32 years (IQR 6.24 -10.25) after transplant. While 33% (17 subjects) had at least one episode of acute rejection requiring treatment, only five patients (10%) had coronary vasculopathy diagnosed at catheterization angiography. No patients had clinical rejection at the time of the CMR. Traditional ventricular volumetric assessment showed preserved function with RV EF 60% (IQR 55 - 64) and LV EF 63% (IQR 59 - 68).Our healthy cardiac transplant group had higher native T1 values at 3T than published pediatric normative data acquired at 3T (1223 ms, p<0.0001).2 While basal LV native T1 was significantly higher for those with history of treated rejection versus without rejection (1318 ± 60 vs. 1265 ± 46, p=0.001), the mid and apical T1 were no different. Basal native T1 (1293 ± 80 vs. 1281 ± 54, p=0.66), as well as mid and apical native T1, were similar for those with and without coronary vasculopathy.
ECV for healthy pediatric cardiac transplant recipients was significantly higher (Table, p<0.0001) than ECV from healthy subjects at 3T (ECV 28%), as described by Maforo et al.3 The transplanted patients’ ECV values did not differentiate those with a history of treated rejection from those without rejection. Finally, ECV did not differ between those with and without coronary vasculopathy.
Discussion
Healthy cardiac transplant recipients have myocardial tissue characteristics different from healthy children, possibly due to additive ill-effects of donor ischemic time, long-term exposure to anti-rejection medications, inflammation from past treated rejection and low-grade (untreated) rejection, and vasculopathy. Although this study is limited by the lack of T2 mapping, the data suggest that each transplant recipient has his own unique myocardial characteristics and once treated for rejection, the ECV values return toward the patient’s own baseline. Ideally, subjects would have catheterization with endomyocardial biopsy within days of CMR to verify their healthy status; this was not performed here but is the next step and a focus of our future work (PEACE Trial, NIH R01- HL164995-01. Future, serial CMR surveillance of the cardiac transplant recipient will permit recognition of significant elevations in myocardial native T1 and ECV which may signal acute rejection.Acknowledgements
No acknowledgement found.References
1. Soslow J and Samyn M. Multi-modal imaging of the pediatric heart transplant recipient. Transl Pediatr 2019 Oct;8(4):322-338.
2. Barczuk-Falęcka M, Małek ŁA, Werys K, et al. Normal values of native T1 and T2 relaxation times on 3T cardiac MR in a healthy pediatric population aged 9–18 years. J Mag Reson Imaging 2020 Mar; 51 (3): 912-918.
3. Maforo NG, Magrath P, Moulin K, et al. T1-Mapping and extracellular volume estimates in pediatric subjects with Duchenne muscular dystrophy and healthy controls at 3T. J Cardiovasc Magn Reason 2020 Dec 10;22(1):85.
Figures
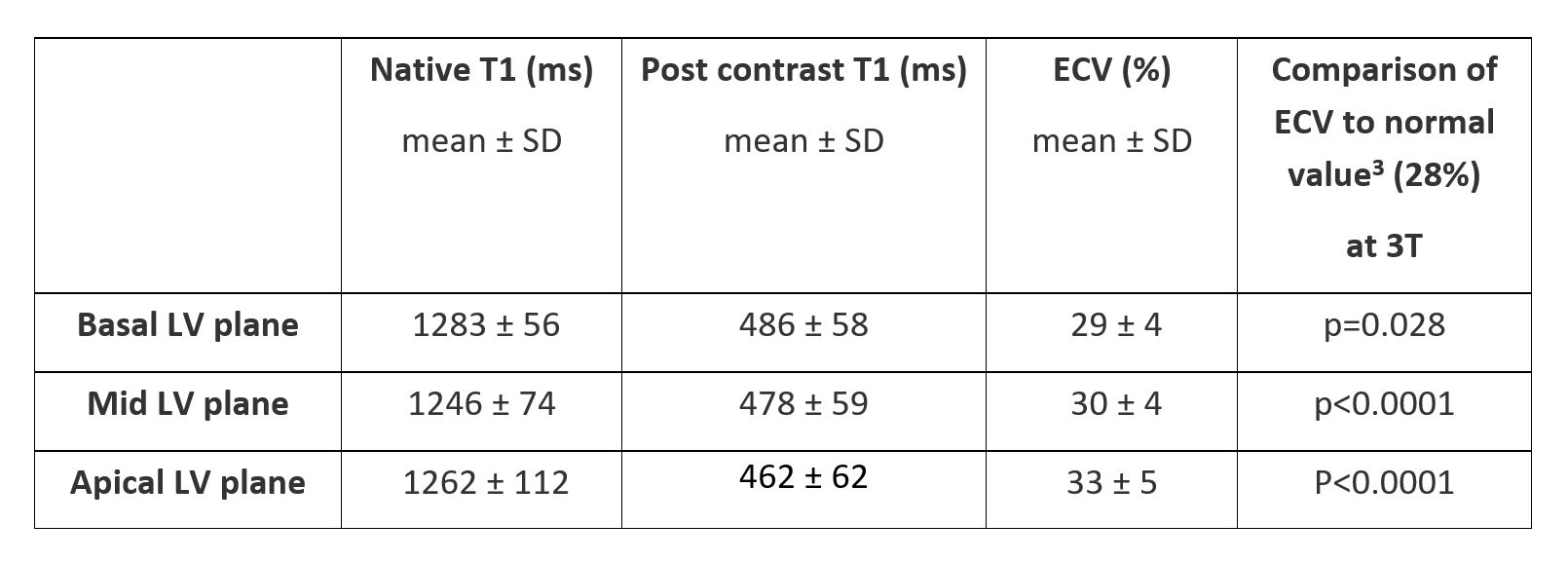
Parametric CMR (3T) Data for Healthy Cardiac Transplant Recipients
DOI: https://doi.org/10.58530/2023/1982