1956
The Feasibility of a Rapid Stroke Protocol of Acute Ischemic Stroke at 3T MRI
Hang Yin1, junbang feng2, fei yu2, Meining chen3, lei xue3, wei yu3, and chuanming li2
1Department of Radiology, Chongqing Emergency Medical Cente, Chongqing, China, 2Chongqing Emergency Medical Center, chongqing, China, 3MR Scientific Marketing, SIEMENS Healthcare, shanghai, China
1Department of Radiology, Chongqing Emergency Medical Cente, Chongqing, China, 2Chongqing Emergency Medical Center, chongqing, China, 3MR Scientific Marketing, SIEMENS Healthcare, shanghai, China
Synopsis
Keywords: Stroke, Stroke
Shortening MR scan time to diagnosis of acute ischemic stroke helps to perform intravenous thrombolysis more quickly and accurately for patients, thus improving the patients’ prognosis. A rapid stroke protocol was evaluated. With about 10 minutes of scanning, we achieved T1 flash, T2 TSE, T2 flair, high-resolution isotropic DWI, TOF and ASL. This protocol improved the detection rate of cerebral infarct lesions without compromising image quality, which help to make thrombolysis of patients with acute ischemic stroke earlier and more accurate.Introduction
The rapid delivery of intravenous thrombolytics within 4.5h of the time of onset has been the most important treatment goal in patients with acute ischemic stroke. MRI enables multiple contrast images and a variety of functional imaging, which plays an important role in acute ischemic stroke, but the main limitation is the long scanning time1. However, with the improvement of MRI hardware and the development of various fast imaging techniques, it is now possible to perform fast MR scans in acute ischemic stroke. Diffusion-weighted MR imaging (DWI) is highly sensitive in diagnosing acute ischemic stroke2, especially sagittal DWI ,which can reduces the probability of false-negative diagnoses3. In our study, we proposed a rapid stroke protocol, that includes high-resolution isotropic DWI.Methods
MRI Protocol: MRI exams were performed on a 3.0-T scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with a phasedarray 64-channel body coil. For MRI examinations of the 3 patients, conventional stroke MRI protocol and proposed rapid stroke protocol were used in the study, and the detailed acquisition parameters of MRI sequences are summarized in Table 1. The proposed rapid stroke protocol included the following core sequences: localizer with three orthogonal orientations in one breath-hold; axial T1-weighted flash; axial T2-weighted turbo-spin echo (TSE) with 5 times grappa; T2-weighted fluid attenuated inversion recovery (flair) TSE; time-of-flight MRA (TOF-MRA)with four subvolumes; and isotropic simultaneous multislice(SMS) Echo-planar-imaging (EPI) diffusion-weighted sequence with b =1000 s/mm2; and fast arterial spin labeling (ASL).Reconstruction: Motsa images from conventional stroke protocol and rapid stroke protocol send to post-processing workstations (Syngo.via, Siemens Healthcare, Erlangen, Germany) to realize 3-dimensional visualization in all directions. ASL can automatically output rCBV images with pseudo-color. Isotropic DWI realized high-resolution reconstruction in sagittal and coronal positions through post-processing workstations.
Data Analysis: The images from the conventional and rapid stroke protocol were respectively sent to the picture archiving and communication system (PACS) system, which were read by randomly assigned radiologist and made a diagnostic report for each case, including infarct location and number of infarcts. An experienced radiologist compared two reports on the same patient and pointed out the differences between the two reports.
Results
The net measurement time of the conventional stroke and the rapid stroke scan time was 10min 6s and 9 min14 s, respectively. All MRI images for the 6 patients had good image quality and no obvious artifacts. Sample images of the conventional and rapid stroke MRI protocol are shown in Figure 1, which demonstrates the high lesion on the DWI images. The sagittal and coronal DWI image reconstructed by axial DWI showed high SNR, clear display of the lesion, and less distortion of the whole image. By comparing the content of the report from the same case , there were good diagnosis consistency of 2 cases, and 4 case were better in reports from rapid protocol.Discussion
This about 10-minute scanning protocol suggested that the rapid stroke protocol is feasible in clinical practice for acute ischemic stroke, with a shorter exam time and high diagnostic concordance compared to the conventional stroke MRI workflow. We reconstructed high-quality sagittal and coronal DWI images by axial isotropic DWI with SMS technology, which not only contribute to shorten the scanning time but also to improve the detection rate of acute ischemic stroke, which was the reason why in 4 cases when comparing the two reports, the rapid protocol performed better than the conventional. According to previous study, infarctions with a short ventrodorsal length and a small volume were clearly detectable using sagittal DWI3. Minimizing the workflow duration is important for acute ischemic stroke, because the outcome of stroke management strongly depends on the onset-to-recanalization time. SMS and GRAPPA technology played a decisive role in the overall rapid protocol4, optimization of scanning time is noticeable without degrading image quality, allowing us to find a balance between the amount of information obtained from the image and the time spent obtaining the images. This is just a preliminary investigation of rapid stroke protocol in acute ischemic stroke, and we will apply this method to more patients in the next step to show the advantages of this protocol.Conclusion
The results show that the proposed rapid stroke MRI protocol is feasible in clinical practice at 3.0T. This modality could serve to accelerate stroke MRI in daily clinical practice, help to make a more prompt and accurate diagnosis of acute ischemic stroke, which might improve the patient’s prognosis.Acknowledgements
No acknowledgement found.References
1. Sung Y, Byungjun K, Bo K, et al. Fast MRI in Acute Ischemic Stroke: Applications of MRI AccelerationTechniques for MR-Based Comprehensive Stroke Imaging. iMRI. 2021;23(2):81-92.
2. Toi H, Uno M, Harada M,et al. Diagnosis of acute brain-stem infarcts using diffusion-weighed MRI. Neuroradiology. 2003;45:352-356.
3. Nobuyuki T, Takachika A, Kiyohiko S, et al.Sagittal diffusion-weighted imaging in preventing the false-negative diagnosis of acute brainstem infarction: Confirmation of the benefit by anatomical characterization of false-negative lesions. Surg Neurol Int. 2019; 10:180-187.
4. Kozak BM, Jaimes C, Kirsch J, et al. MRI techniques to decrease imaging times in children. Radiographics. 2020; 40:485-502.
Figures
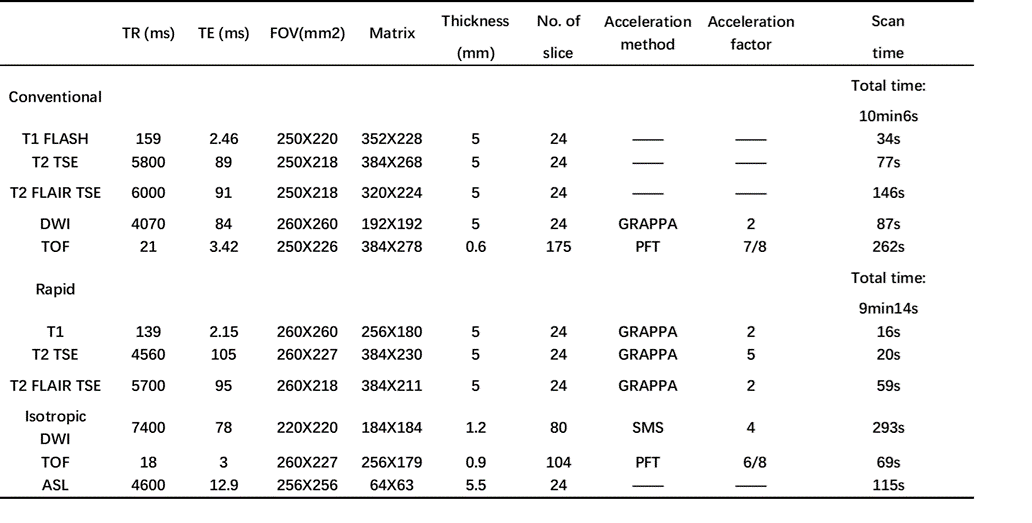
TABLE 1. MRI parameters of rapid stroke MRI
protocol and conventional stroke protocol.
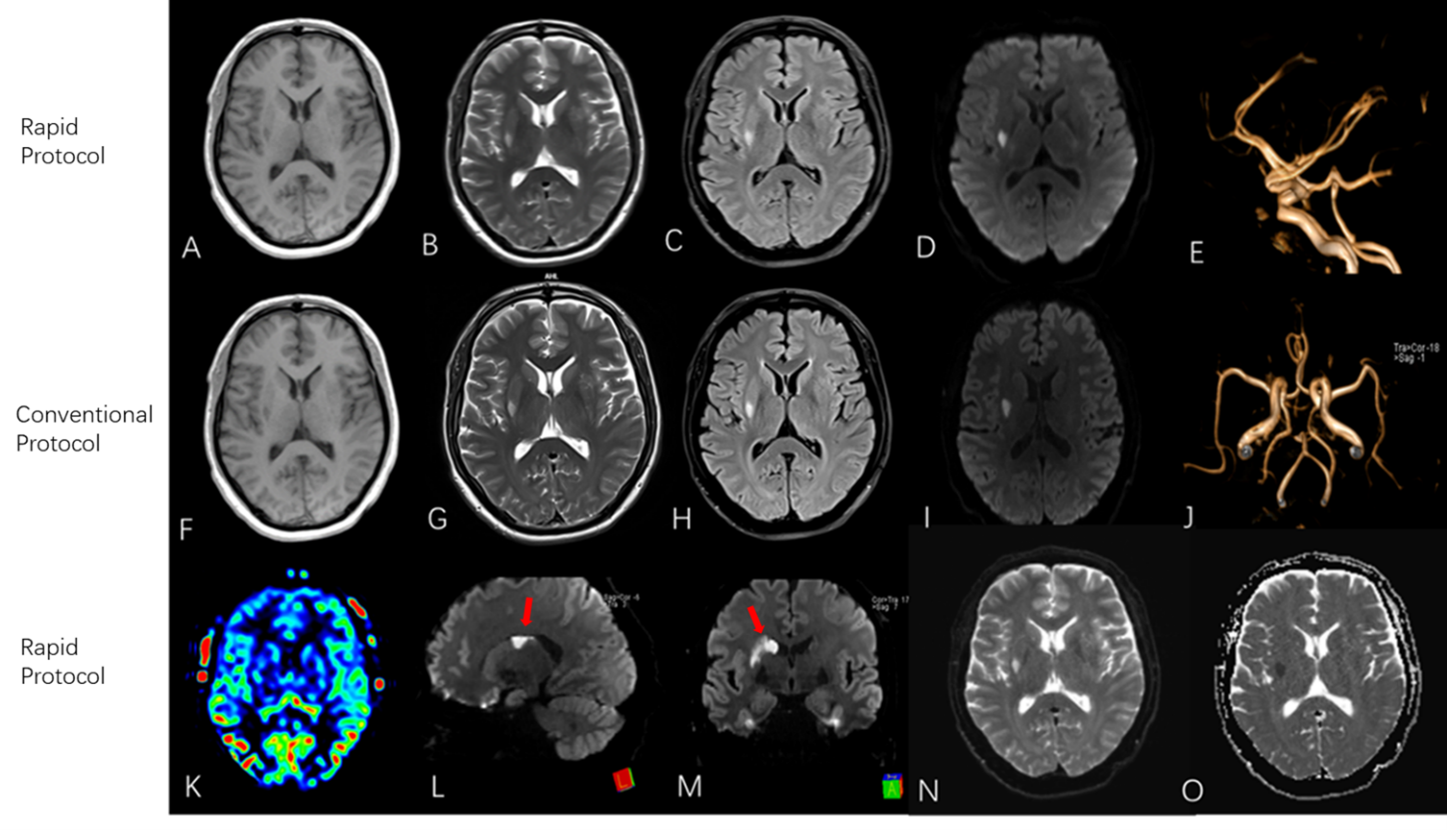
FIGURE 1. Compared images acquired with rapid
stroke MRI protocol (first and third rows) and conventional protocol ( second
row) of a 74-year-old man with acute ischemic
stroke: (A, F) T1 FLASH; (B, G)T2 TSE; (C, H)T2 flair; (D,I)axial DWI with b=1000 s/mm2; (E, F) TOF MRA; (K)ASL; (N, O)
DWI with b=0 s/mm2. Reconstructed
high-quality sagittal(L) and coronal DWI(M) images by axial isotropic DWI with
SMS technology shows a clear hyper-intensity, which is indicated by an arrow.
DOI: https://doi.org/10.58530/2023/1956