1868
Accelerated diffusion-weighted imaging of the prostate employing Echo Planar Imaging with Compressed SENSE based reconstruction (EPICS)
Yannik Christian Layer1, Petra Muertz1, Leon Bischoff1, Christoph Katemann2, Kilian Weiss2, Julian Luetkens1, Ulrike Attenberger1, and Claus Christian Pieper1
1Department of Diagnostic and Interventional Radiology, University Hospital Bonn, Bonn, Germany, 2Philips GmbH Market DACH, Hamburg, Germany
1Department of Diagnostic and Interventional Radiology, University Hospital Bonn, Bonn, Germany, 2Philips GmbH Market DACH, Hamburg, Germany
Synopsis
Keywords: Prostate, Tumor
The aim of this single-center, prospective study was to evaluate an accelerated diffusion-weighted imaging sequence of the prostate using Echo Planar Imaging with Compressed SENSE based reconstruction and assess its performance in comparison to conventional DWI. The evaluated sequences considerably reduced the total DWI acquisition time by 43% and achieved overall good image quality without significant differences compared to the conventional DWI sequence. The reduced scan time allows for an increase of the overall number of scanned patients as well as increased patient convenience with less potential of motion artifacts and therefore benefits care of patients with suspected prostate cancer.Introduction
Multiparametric MRI of the prostate has become diagnostic standard for detection of prostate lesions1. The combination of T2-weighted images with diffusion-weighted imaging (DWI) and dynamic contrast-enhanced sequences has proven to achieve high sensitivity for the detection of prostate cancer2, 3. As the number of patients suspected of prostate cancer increases especially in ageing societies, there is a strong need for dependable but accelerated MRI sequences4, 5. Therefore, the aim of this single-center, prospective study was to evaluate an accelerated DWI sequence of the prostate using Echo Planar Imaging with Compressed SENSE based reconstruction (EPICS, SmartSpeed Diffusion, Philips Healthcare, Best, The Netherlands) and assess its performance in comparison to conventional, SENSE (Sensitivity Encoding) based, DWI.Methods
Data was collected from 35 male patients (mean age: 67 years; range: 52 – 81 years) with clinically suspected prostate cancer undergoing a MRI-examination of the prostate on a 3T-scanner (Ingenia Elition X, Philips Healthcare, Best, The Netherlands). The institutional review committee approved this study and all participants gave written informed consent prior to the examination.A total of 4 different DWI sequences were acquired in each patient: A 3 b-value scan (b=100, 400, 800s/mm²) for ADC calculation and a DWI sequence with b=1500s/mm². Both scans were acquired conventionally with SENSE and with EPICS. Due to the denoising capabilities of compressed SENSE, acceleration of the DWI-EPICS scans is achieved by reducing the number of averages per b-value.
Two blinded radiologists (2 years and 11 years’ experience) qualitatively rated both sequences on 5-point-Likert-items from 1 (non-diagnostic) - 5 (excellent) for artifacts, lesion conspicuity, and overall image quality. Additionally both independently rated the Prostate Imaging Reporting and Data System (PIRADS 2.1) for DWI. Furthermore, regions-of-interest (ROIs) were drawn in prostate lesion and normal appearing peripheral zone of the prostate by a single radiologist (2 years’ experience). Mean and standard deviation values were determined for each ROI. For quantitative assessment, based on image intensity distribution (mean, standard deviation (SD)), the apparent contrast-to-noise ratio of lesion (L) / regular peripheral zone of the prostate (PZ) (aCNRLesion=( SIL- SIPZ)/SDPZ) and apparent signal-to-noise ratio (aSNRLesion= SIL/SDPZ) were calculated. For patients without prostate lesions aSNRPZ was calculated separately for the peripheral zone (aSNRPZ= SIPZ/SDPZ). Mean ADC and coefficient of variation (CV) of ADC were compared. Statistical analysis was performed using Wilcoxon signed-rank test and paired sample t-test. Interrater reliability of qualitative image assessment was evaluated using intraclass correlation coefficient (ICC) estimates.
Results
The average acquisition time of the 3-b-value EPICS DWI-sequence (125 seconds) was 42% shorter than that of the conventional DWI-sequence (215 seconds; p<0.001) and average acquisition time of the EPICS DWI-b1500-sequence (139 seconds) was 44% shorter than that of conventional DWI-b1500 (250 seconds; p<0.001), leading to a total scantime reduction of approximately 43%.17/35 patients (48.6%) showed prostate lesions. Quantitative analysis (Table 1) revealed for both sequences no significant differences between parameters obtained conventionally and with EPICS, neither for aCNRLesion, nor for aSNRLesion or aSNRPZ. A tendency towards higher aSNRLesion values on DWI with b400 was found for EPICS (15.59 ± 10.89 vs. 13.45 ± 6.92, p=0.08). Mean ADC and CV of ADC also showed no significant differences (Table 2).
There was no significant difference in the rating of artifacts, lesion conspicuity, overall image quality and PIRADS-score (Table 3, Figure 1). Interobserver reliability for overall qualitative scoring was good (ICC=0.82; (95% CI: 0.786; 0.849)). Figure 2 shows representative DW images and ADC maps of a patient.
Discussion
The new diffusion-weighted imaging sequence with Echo Planar Imaging and Compressed SENSE based reconstruction (EPICS) shows only minor quantitative differences and no significant qualitative differences compared to conventional DWI while significantly reducing the total acquisition time by 43%. The differences in aSNR and aCNR for the b-values can be explained by the different impact of the averaging of each b-value.As PIRADS-score-rating was identical between both sequences, the scanning/reconstruction technique had no impact on clinical decisions. Therefore, the evaluated diffusion-weighted imaging sequence with EPICS offers a potential to accelerate diffusion-weighted images in MRI. Further studies on a larger patient cohort are needed to show the full potential of the sequences in clinical routine.
Conclusion
The evaluated accelerated diffusion-weighted imaging sequence employing Echo Planar Imaging with Compressed SENSE based reconstruction (EPICS) shows comparable results to the conventional sequence used in clinical routine while significantly reducing the acquisition time. The reduced scan time allows for a considerable increase of the overall number of scanned patients, increased patient convenience with less potential of motion artifacts and therefore benefits care of patients with suspected prostate cancer.Acknowledgements
The present work was supported by Philips Healthcare.References
- Weiss J, Martirosian P, Notohamiprodjo M, et al. Implementation of a 5-Minute Magnetic Resonance Imaging Screening Protocol for Prostate Cancer in Men With Elevated Prostate-Specific Antigen Before Biopsy. Investigative Radiology: March 2018 - Volume 53 - Issue 3 - p 186-190
- Purysko AS, Bittencourt LK, Bullen JA, et al. Accuracy and interobserver agreement for Prostate Imaging Reporting and Data System, Version 2, for the characterization of lesions identified on multiparametric MRI of the prostate. AJR Am J Roentgenol. 2017;209:339–349.
- Scheenen TW, Rosenkrantz AB, Haider MA, et al. Multiparametric magnetic resonance imaging in prostate cancer management: current status and future perspectives. Invest Radiol. 2015;50:594–600.
- Pernar CH, Ebot EM, Wilson KM, Mucci LA. The Epidemiology of Prostate Cancer. Cold Spring Harb Perspect Med. 2018 Dec 3;8(12): a030361.
- Bischoff LM, Katemann C, Isaak A, et al. T2 Turbo Spin Echo With Compressed Sensing and Propeller Acquisition (Sampling k-Space by Utilizing Rotating Blades) for Fast and Motion Robust Prostate MRI: Comparison With Conventional Acquisition. Invest Radiol. 2022 Sep 1.
Figures
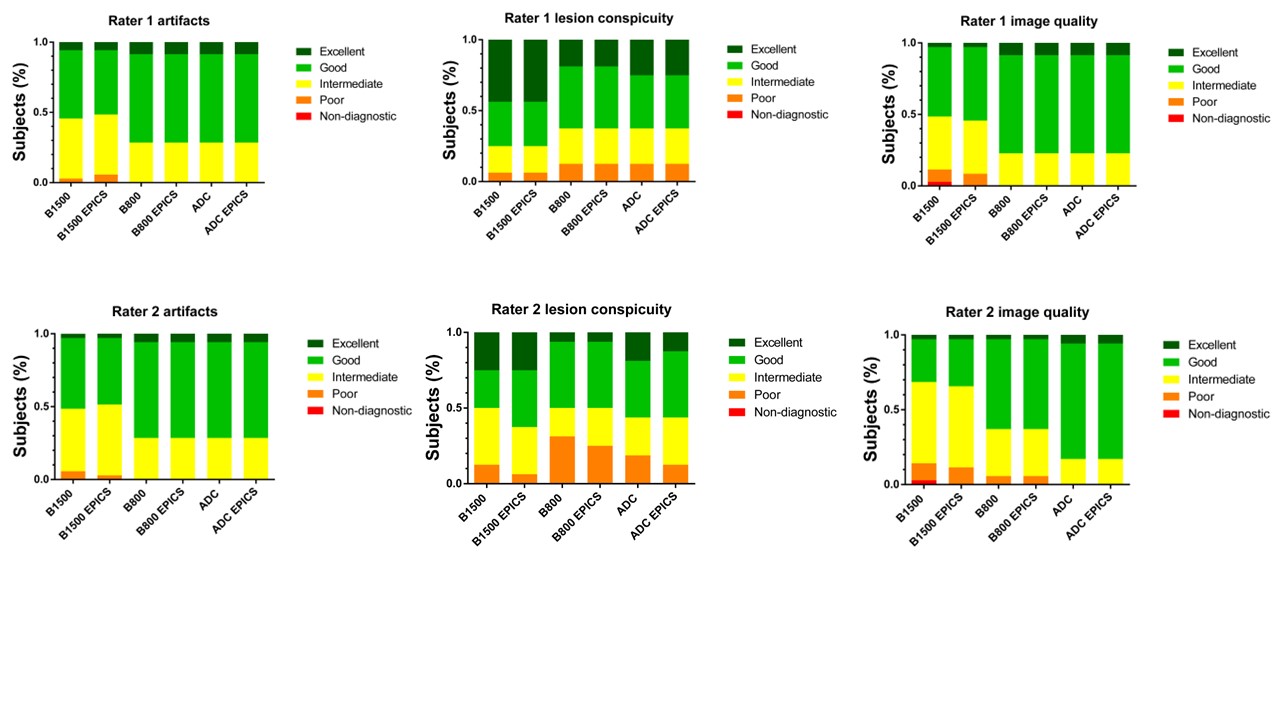
Figure 1: Bar plots show distribution of
artifacts, lesion conspicuity and overall image quality rating of conventional
DWI and EPICS DWI with b1500, b800 and ADC.
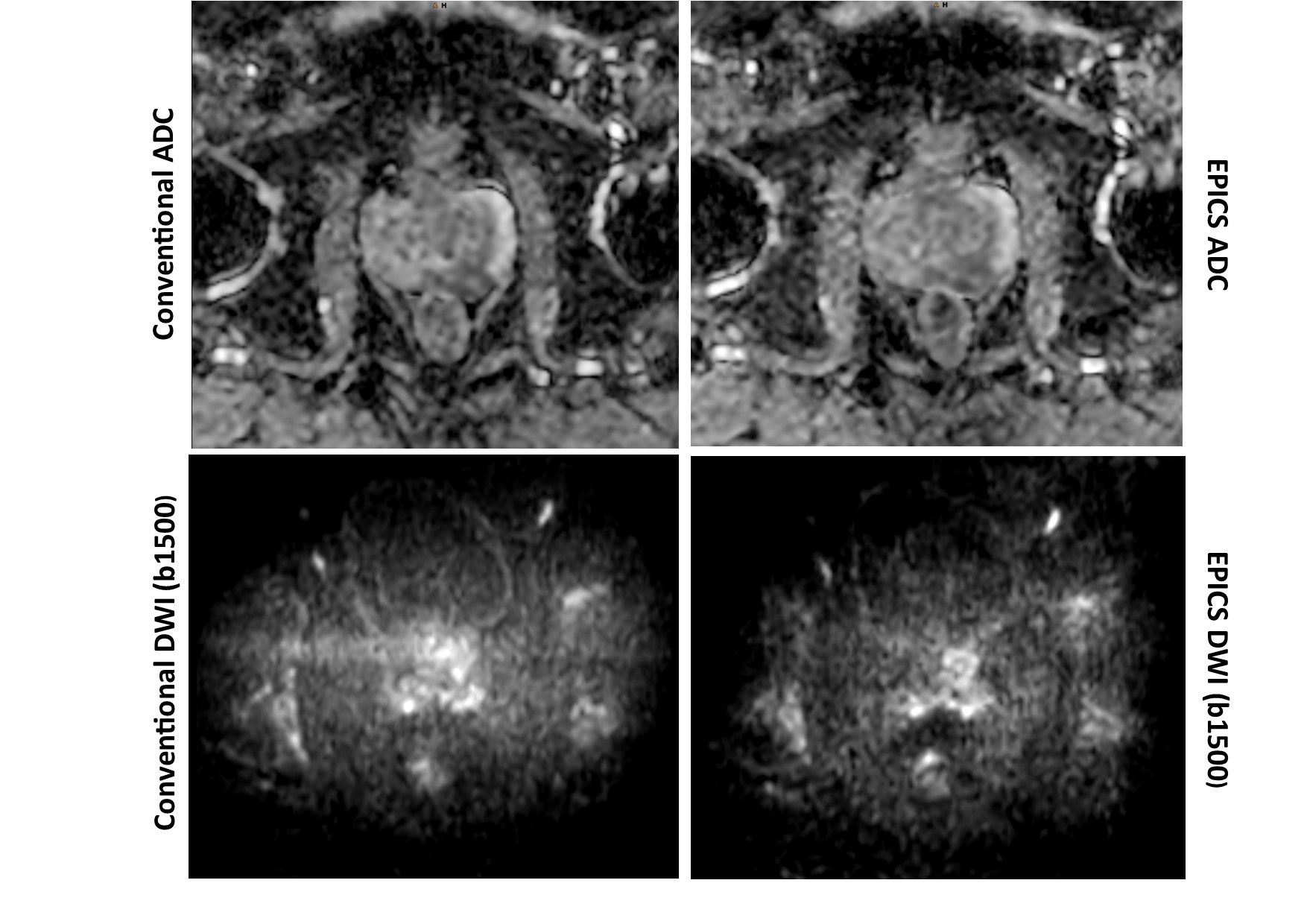
Figure 2: DWI
b1500 images and ADC maps obtained from conventional DWI and DWI with EPICS. In
this example artifacts are reduced in EPICS DWI (b1500) compared to conventional
reconstruction. No significant changes are seen in the ADC maps.

Table 1: Summary of aSNR and aCNR for patients
with and without prostate lesions and their corresponding p-values in
conventional DWI and accelerated DWI sequence of the prostate with Echo Planar
Imaging and Compressed SENSE based reconstruction (EPICS).
P-values
below 0.05 were considered significant.

Table 2: Summary of ADC and ADC coefficient of
variation (CV) measurements of DWI and accelerated DWI sequence of the prostate
with Echo Planar Imaging and Compressed SENSE based reconstruction (EPICS). Given
are mean values ± standard deviation together with corresponding P-values. P-values
below 0.05 were considered significant.
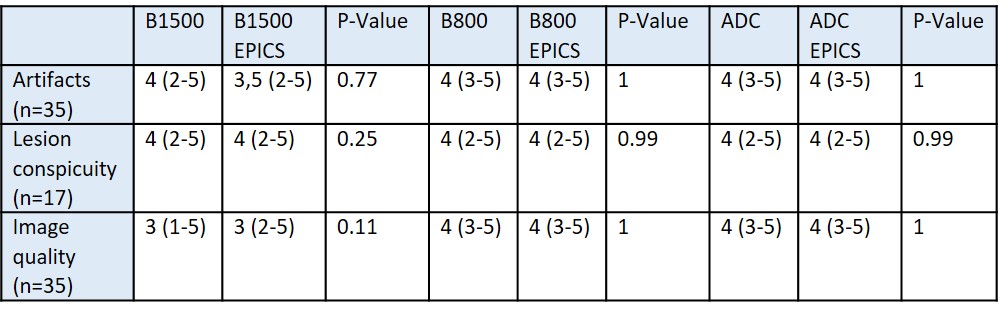
Table 3: Summary of the ratings on 5-point-Likert-items
from 1-5 (non-diagnostic - excellent) for artifacts, lesion conspicuity and
overall image quality. Given are median values and range together with
corresponding P-values. P-values below 0.05 were considered significant.
DOI: https://doi.org/10.58530/2023/1868