1860
High-resolution PROPELLER T2-weighted imaging of the prostate with deep learning reconstruction: a phantom and clinical preliminary study
Atsushi Nakamoto1, Hiromitsu Onishi1, Takahiro Tsuboyama1, Takashi Ota1, Hideyuki Fukui1, Keigo Yano1, Kengo Kiso1, Toru Honda1, Shohei Matsumoto1, Mitsuaki Tatsumi1, Hiroyuki Tarewaki2, Yoshihiro Koyama2, Tetsuya Wakayama3, Xinzeng Wang4, and Noriyuki Tomiyama1
1Osaka University Graduate School of Medicine, Suita, Japan, 2Osaka University Hospital, Suita, Japan, 3GE Healthcare, Hino, Japan, 4GE Healthcare, Houston, TX, United States
1Osaka University Graduate School of Medicine, Suita, Japan, 2Osaka University Hospital, Suita, Japan, 3GE Healthcare, Hino, Japan, 4GE Healthcare, Houston, TX, United States
Synopsis
Keywords: Prostate, Image Reconstruction, Deep learning reconstruction
The image quality of high-resolution PROPELLER T2WI combined with deep learning reconstruction (DLR) in prostate MRI was evaluated by the phantom and clinical studies. In the phantom study, noise reduction was achieved by DLR, and spatial resolution was remarkably improved in PROPELLER T2WI compared to Cartesian T2WI. In the clinical study, DLR showed a significant improvement in signal-to-noise ratio, and the qualitative analyses showed reduced image noise and improved spatial resolution, with PROPELLER T2WI DLR images showing the highest overall image quality. PROPELLER T2WI with DLR would be promising technique to improve the image quality of T2WI in prostate MRI.Introduction
T2-weighted imaging (T2WI) is an essential sequence for the morphological evaluation of the prostate and a dominant sequence in the diagnosis of transitional zone (TZ) cancers1. Although Prostate Imaging Reporting and Data System (PI-RADS) recommends a slice thickness of 3 mm and in-plane resolution of ≤0.7 × ≤0.4 mm for T2WI1, it might be difficult to maintain a sufficient signal-to-noise ratio (SNR) depending on the performance of the scanner. Recently, deep learning reconstruction (DLR) has been introduced into clinical practice, and its usefulness in improving SNR and reducing acquisition time has been reported in prostate MRI2, 3. DLR has been newly available for periodically rotated overlapping parallel lines with enhanced reconstruction (PROPELLER) sequences. The purpose of this study was to evaluate the image quality of high-resolution PROPELLER T2WI combined with DLR in prostate MRI.Methods
Phantom study:A phantom (Magphan® 170, The Phantom Laboratory, NY, USA) was scanned with a 3-Tesla scanner (SIGNA Architect, GE Healthcare, Waukesha, WI). T2WI was scanned using two acquisition methods (Cartesian and PROPELLER) with various matrix settings (512 × 512, 448 × 448, and 384 × 384). For Cartesian T2WI only, an additional 448 × 280 matrix images were obtained, which are used in our daily clinical practice. Other parameters are as follows: TR/TE, 5400/81.9–82.5 msec; Echo train length, 14 (Cartesian)/32 (PROPELLER); Band width, 62.5 Hz; FOV, 20 × 20 cm; Slice thickness/gap, 3/0 mm; NEX, 1 (Cartesian)/1.5 (PROPELLER); Slice number, 24. Both T2WI were reconstructed with conventional method (original image) and DLR. A radiologist evaluated images of the high-resolution test plate, which contains rectangular slots forming a test pattern which ranges from one to eleven line pairs per cm (5mm to 0.45mm resolution), and assigned scores regarding the spatial resolution using a 6-point scale (6, could completely separate 11 lines/cm; 5, 10 lines/cm; 4, 9 lines/cm; 3, 8 lines/cm; and 2, 7 lines/cm; 1, < 7 lines/cm). Circular regions of interest (ROIs) were placed on homogeneous areas within the phantom, and the standard deviation (SD) of the signal was measured and employed as the index of image noise.
Clinical Study:
This study included fourteen patients who underwent prostate MRI including conventional Cartesian T2WI (C-T2WI) and PROPELLER T2WI (P-T2WI). The written informed consent was obtained from all patients. The matrix sizes of C-T2WI and P-T2WI were 448 × 280 and 512 × 512, respectively, and other parameters were the same as those used in the phantom study. The acquisition times for C-T2WI and P-T2WI were 4 min 9 sec and 3 min 58 sec, respectively. A radiologist placed ROIs on the peripheral zone (PZ) and TZ of the prostate, and the signal and SD of the signal were measured. The SNR was calculated by dividing the signal by SD, and compared among 4 images (C-T2WI original, C-T2WI DLR, P-T2WI original, and P-T2WI DLR) using Friedman’s test followed by post hoc Wilcoxon signed rank test with Bonferroni correction (n = 6). As a qualitative analysis, a radiologist who was blinded to the acquisition and reconstruction methods reviewed images and assigned scores regarding the noise, sharpness, spatial resolution, and overall image quality using a 5-point scale.
Results
Phantom study:For both acquisition methods, the larger the matrix size, the more image noise was present, and noise was reduced by using DLR (Figure 1, 2). The spatial resolution of P-T2WI was obviously improved with DLR, and 11 lines/cm could be separated in the 512 and 448 matrices, while C-T2WI showed mild improvement in spatial resolution with DLR.
Clinical Study:
The results of the quantitative analysis are summarized in Figure 3. DLR images showed improved SNR compared to original images, with significant differences in PZ and TZ for C-T2WI and TZ for P-T2WI (P < 0.01). The results of the qualitative analysis are summarized in Figure 4. Regarding noise, scores for both C-T2WI and P-T2WI were significantly increased with DLR (i.e., image noise was reduced) (P < 0.01). Regarding sharpness and spatial resolution, scores for P-T2WI were higher than for C-T2SWI, with the highest scores for P-T2WI DLR. P-T2WI DLR had the highest score for overall image quality, followed by C-T2WI DLR (Figure 5).
Discussion
Our results showed that DLR reduced image noise and improved SNR in P-T2WI as well as in C-T2WI. Furthermore, in the phantom study, DLR showed a more prominent improvement in spatial resolution in PROPELLER than in Cartesian, and in the clinical study, P-T2WI DLR showed the highest spatial resolution and image quality. Therefore, the combination of PROPELLER and DLR would be a promising technique for simultaneously improving the spatial resolution and image quality of prostate MRI, thereby improving diagnostic performance. This is a preliminary study using a relatively small number of cases, and further evaluation of the clinical usefulness of this technique, including its detectability of prostate cancers, will be needed using a larger number of cases.Conclusion
PROPELLER T2WI combined with DLR resulted in image noise reduction and improved spatial resolution. This technique enables high-resolution T2WI imaging with high image quality and is expected to contribute to the improvement of the quality of prostate MRI.Acknowledgements
No acknowledgement found.References
1. Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019;76(3):340-351.
2. Wang X, Ma J, Bhosale P, et al. Novel deep learning-based noise reduction technique for prostate magnetic resonance imaging. Abdom Radiol (NY). 2021;46(7):3378-3386.
3. Park JC, Park KJ, Park MY, Kim MH, Kim JK. Fast T2-Weighted Imaging With Deep Learning-Based Reconstruction: Evaluation of Image Quality and Diagnostic Performance in Patients Undergoing Radical Prostatectomy. J Magn Reson Imaging. 2022;55(6):1735-1744.
Figures

The
bar graph represents the objective noise level (SD of the signal), and the line
graph represents the 5-point visual score for spatial resolution. The noise was
reduced in the DLR image compared to the original image for all acquisition methods.
Regarding the spatial resolution, Cartesian images did not show an increase in
score with DLR except for the 448 × 280 image, while PROPRLLER images showed an
increase in score for all matrix settings.
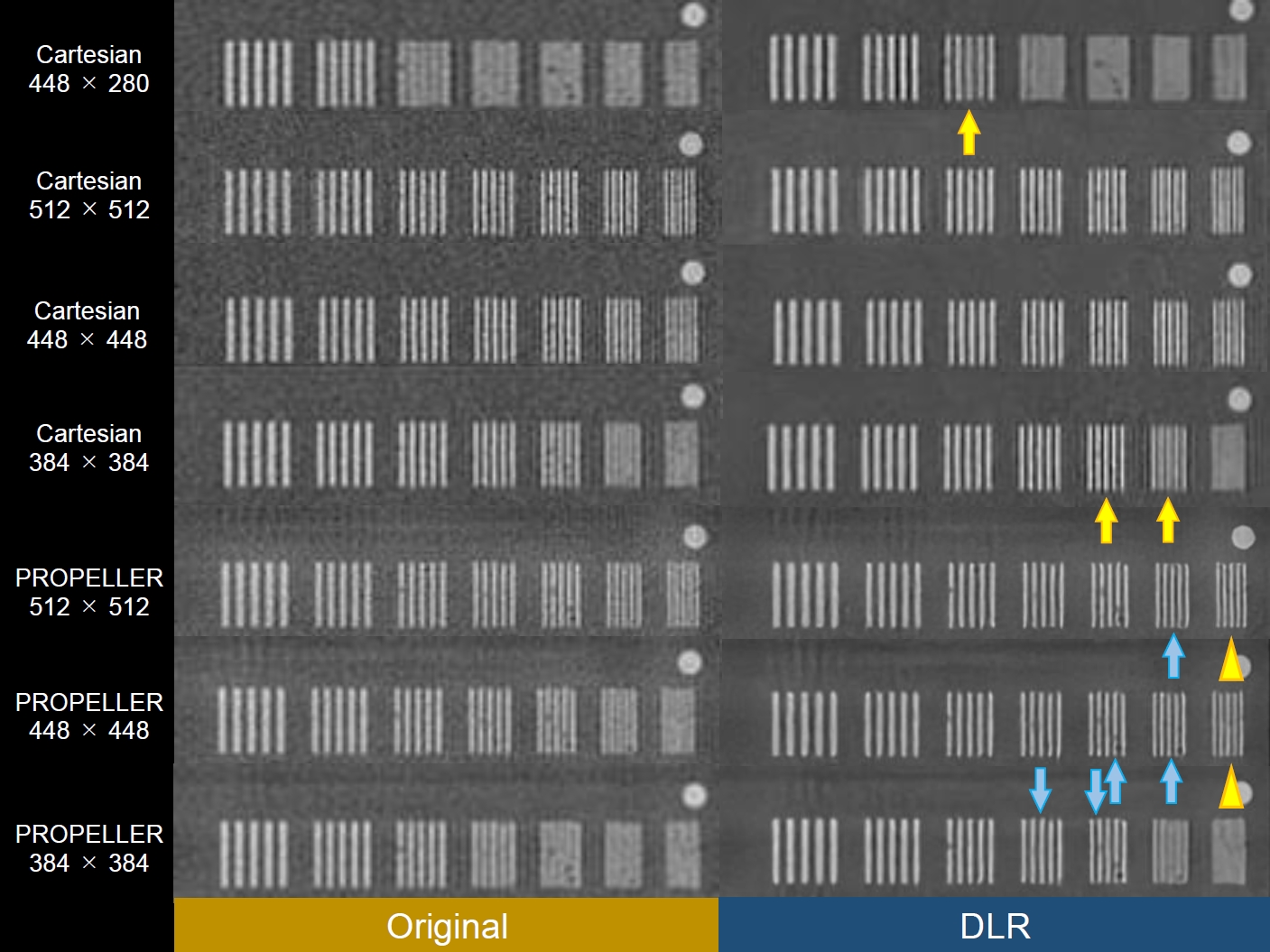
Figure 2: Images
of high-resolution test plate reconstructed with the conventional method (original)
and DLR. PROPRLLER shows improved spatial resolution with DLR, allowing 11
lines/cm slots to be separated in the 512- and 448-matrix DLR images
(arrowheads). Although Cartesian also shows improvement in spatial resolution
with DLR in some images (yellow allows), the improvement in spatial resolution
with DLR is more noticeable in PROPELLER (blue allows).
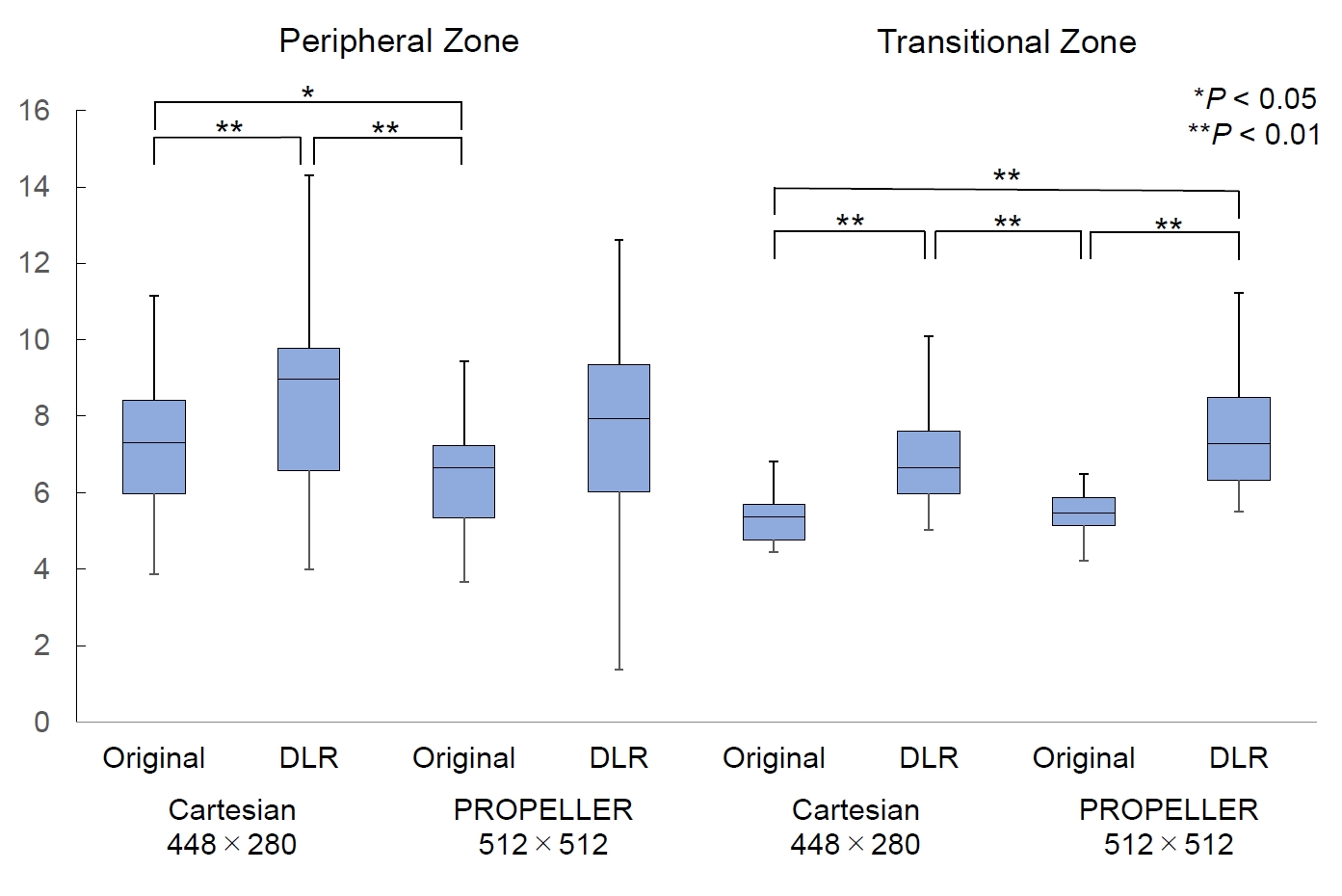
Figure 3: Signal-to-noise
ratios of the peripheral and transitional zones of the prostate measured in
clinical cases. In both zones, SNR was improved by DLR, with significant
differences in PZ and TZ for Cartesian T2WI and TZ for PROPELLER T2WI (P
< 0.01).
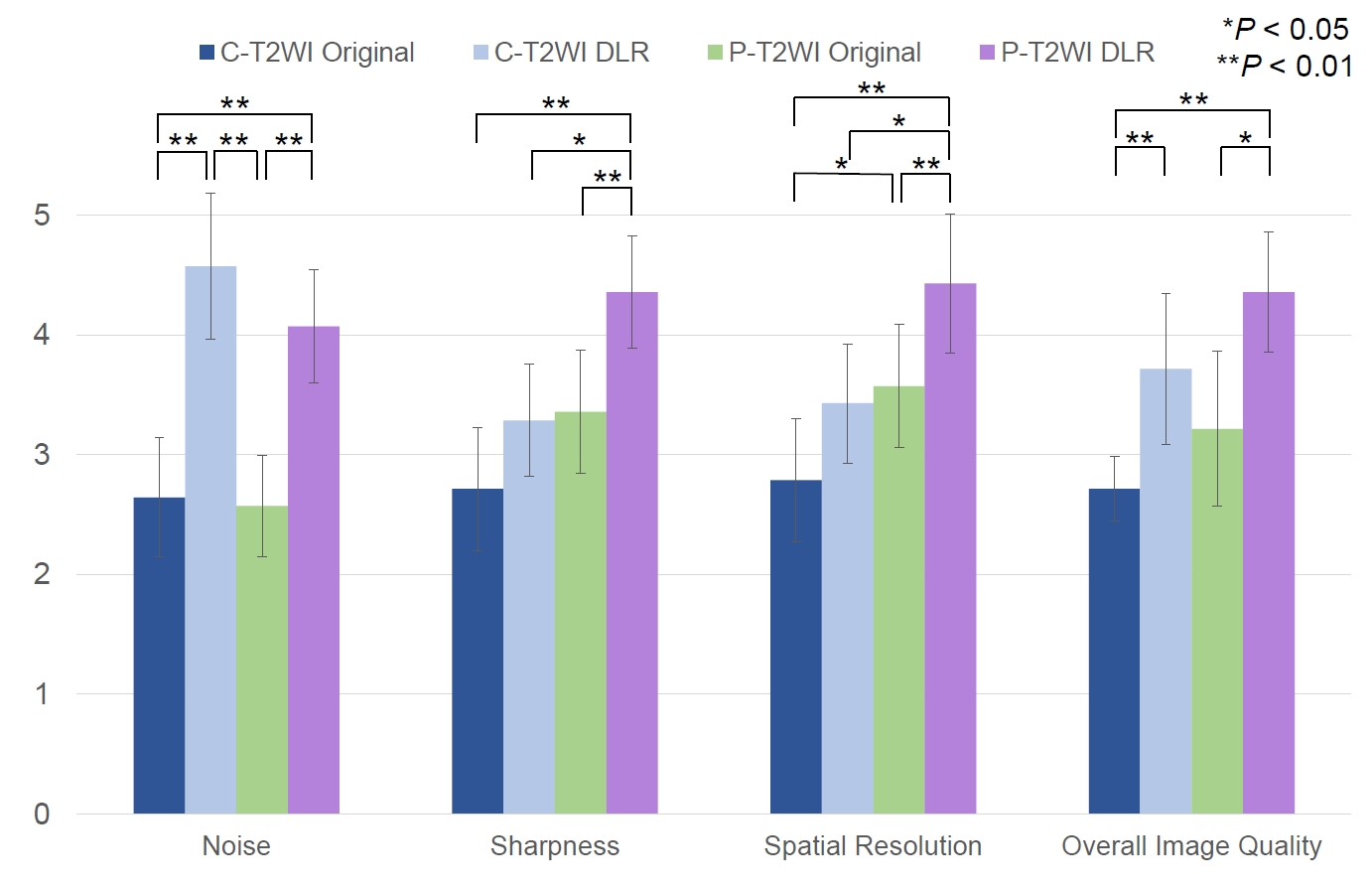
Figure 4: Mean
visual scores of qualitative analyses. Subjective image noise was reduced by
DLR in both Cartesian and PROPELLER T2WI (P < 0.01). The PROPELLER
T2WI DLR had the highest scores for sharpness, spatial resolution, and overall
image quality.
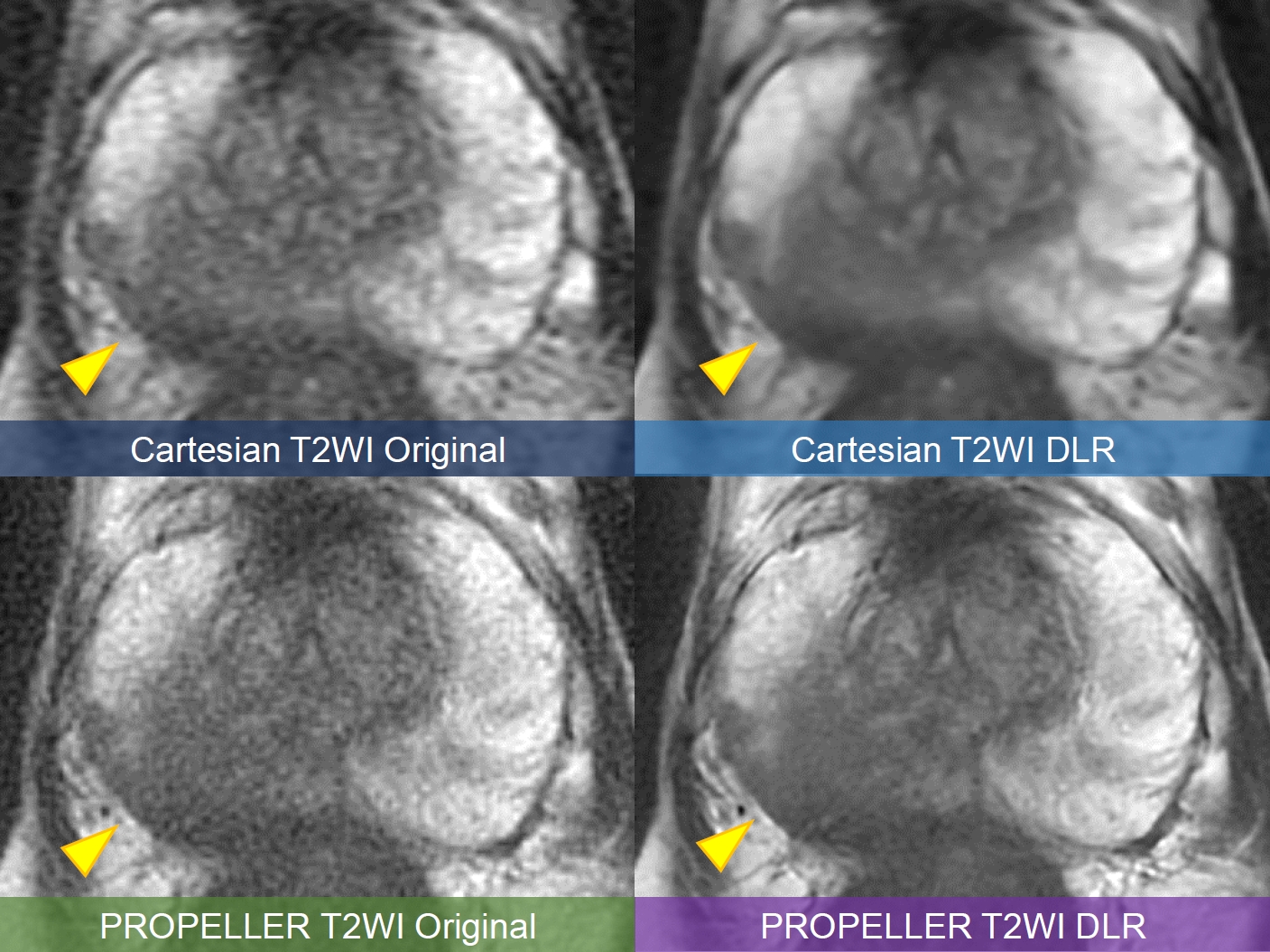
Figure 5: A
male in his 70s. Image noise is reduced by DLR in both Cartesian and PROPELLER
T2WI; the PROPELLER T2WI DLR image is the sharpest and shows more detailed
structures. The tumor in the right peripheral zone (arrowheads) is most clearly
depicted by PROPELLER T2WI DLR. A biopsy performed after MRI revealed prostate
cancer (Gleason score 4+4) in the right lobe.
DOI: https://doi.org/10.58530/2023/1860