1801
Does simultaneous multi-slice technique affect quantitative measurements of diffusion-weighted MR imaging in hepatocellular carcinoma?1Department of Radiology, West China Hospital, Sichuan University, Chengdu, China, 2MR collaborations, Siemens Healthcare Ltd., Shanghai, China, 3MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Keywords: Quantitative Imaging, Diffusion/other diffusion imaging techniques
Although diffusion weighted MR imaging is of great importance in the diagnosis and evaluation of hepatocellular carcinoma (HCC), it is limited by long acquisition times. Simultaneous multi-slice (SMS) technique can reduce scan time and has been proved to be feasible in liver imaging. Our study included twenty patients with HCC, and acquired conventional and SMS-accelerated diffusion data with different models (DWI, DKI and IVIM). By analyzing quantitative parametric maps, we found SMS technique did not affect the quantitative measurements of HCC. However, the difference of mean kurtosis between conventional and SMS-accelerated DKI in liver parenchyma should be noted.Introduction
Diffusion weighted imaging (DWI) plays an essential role in the detection and diagnosis of hepatocellular carcinoma (HCC)1. In addition, previous studies have shown that quantitative diffusion parameters can predict tumor aggressiveness and evaluate treatment response of HCC2,3. Despite the great clinical potential, liver DWI still suffers from many practical problems4. Notably, the relatively long acquisition time of DWI with multiple b-values or advanced diffusion models, such as diffusion kurtosis imaging (DKI) and intravoxel incoherent motion (IVIM), may hamper its widespread application in clinical practice. With recent advances in MR imaging, simultaneous multi-slice (SMS) acceleration technique has been developed to reduce scan time5. The feasibility of SMS technique has been demonstrated in abdominal DWI with shortened acquisition time and comparable image quality6,7. However, the impact of SMS technique on quantitative measurements in different diffusion models, especially in diseased tissues, remains unknown.Purpose
To investigate whether SMS technique affects the quantitative measurements of diffusion weighted MR imaging sequences in HCC and liver parenchyma.Materials and Methods
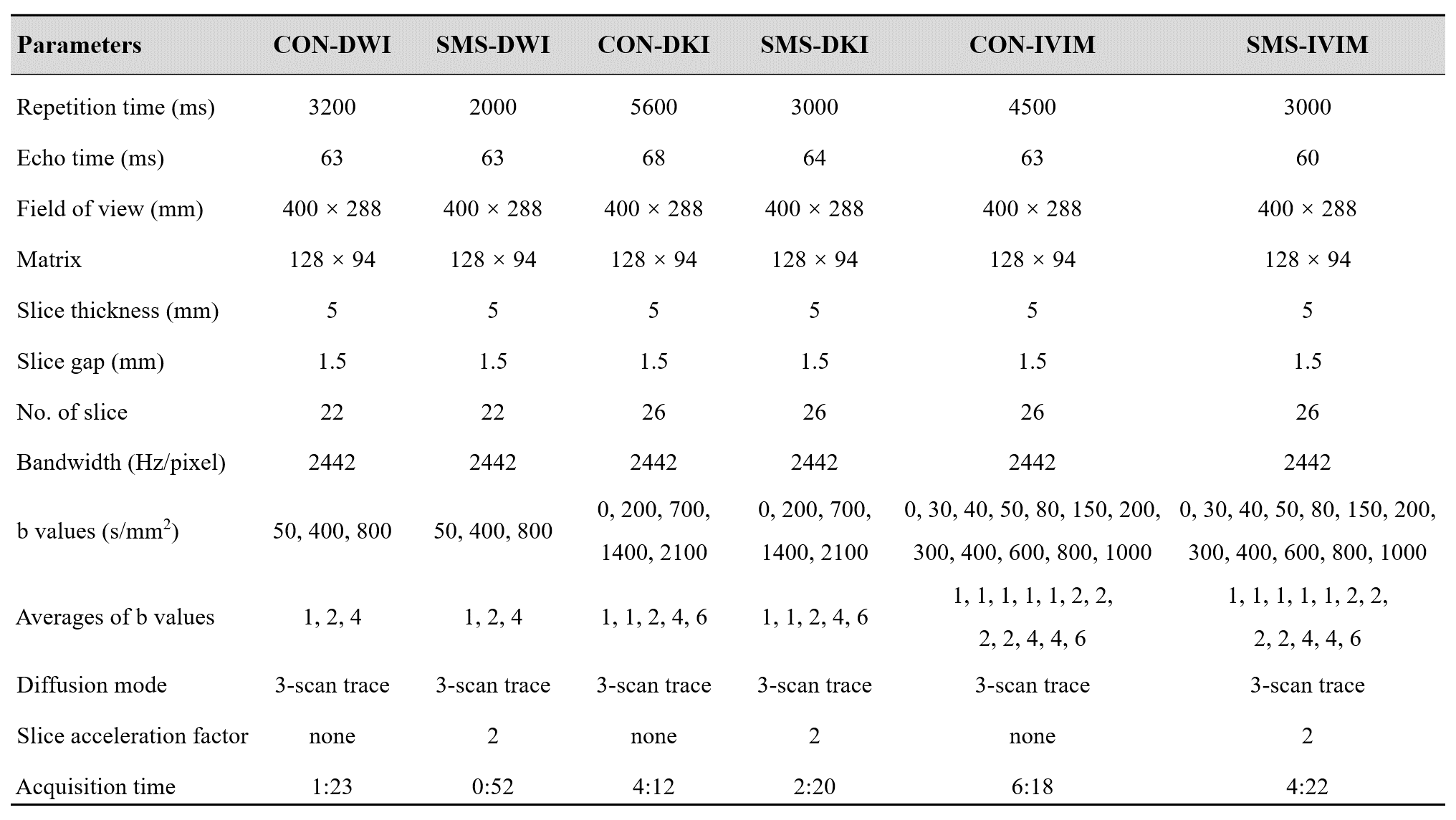
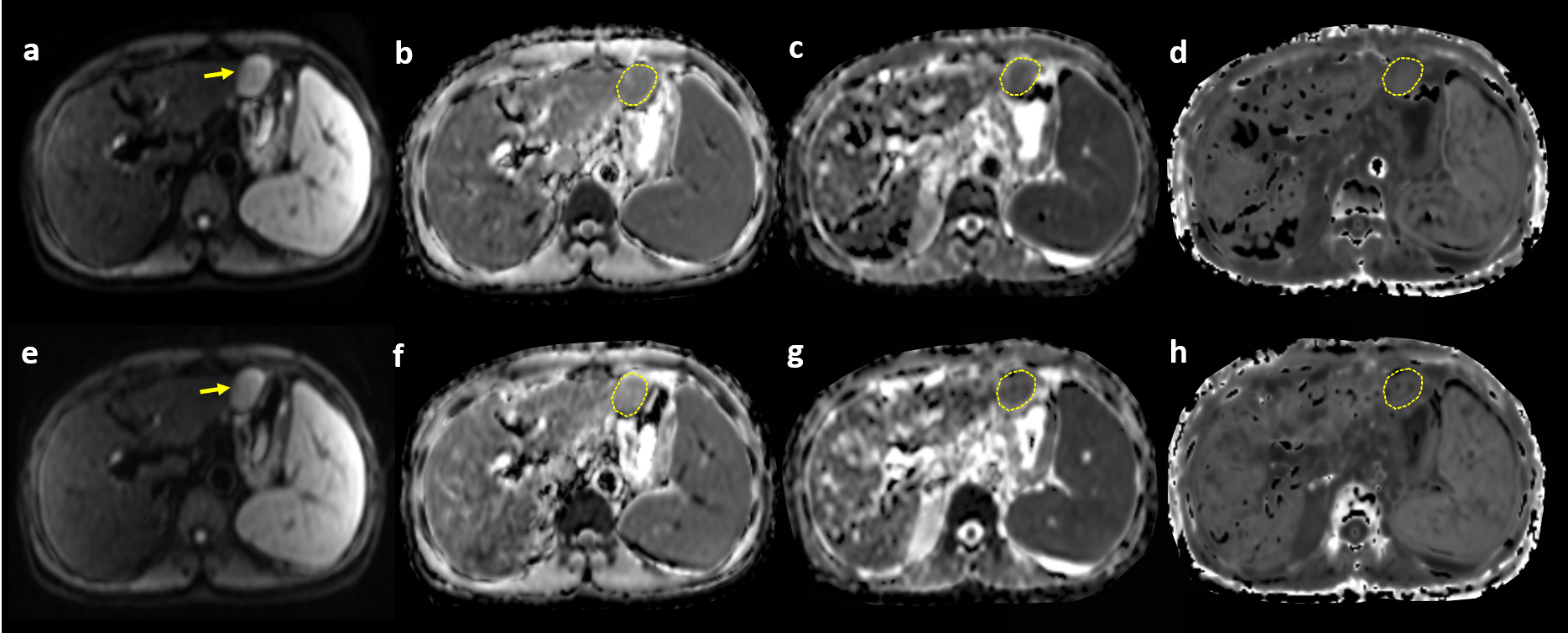
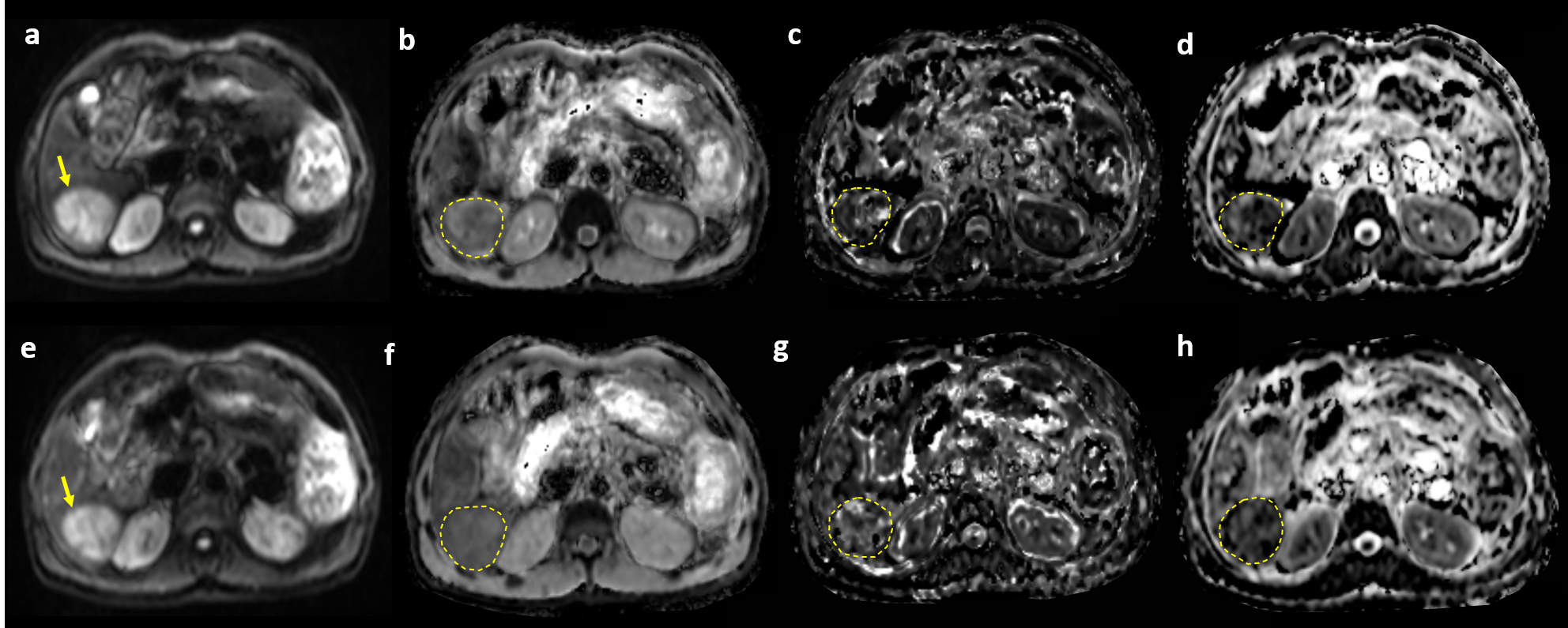
Institutional review board approved this prospective study and all participants provided written informed consent. A total of twenty patients (sixteen men and four women; mean age ± standard deviation [SD], 55.15 years ± 11.47) with pathology-proven HCC were included from June 2021 to October 2021. Preoperative MR examinations were performed on a 3 T scanner (MAGNETOM Skyra, Siemens Healthineers, Erlangen, Germany) with an 18-channel body coil. Conventional (CON) and SMS-accelerated diffusion weighted sequences, including CON-DWI, SMS-DWI, CON-DKI, SMS-DKI, CON-IVIM, SMS-IVIM, were conducted sequentially in free-breathing manner (Figure 1). All images were transferred to syngo.via frontiers workstation and analyzed by a prototype MR Body Diffusion toolbox (v1.4.0), yielding apparent diffusion coefficient (ADC) for DWI, mean kurtosis (MK) and mean diffusivity (MD) for DKI, as well as true diffusion coefficient (D), perfusion-related diffusion (D*) and perfusion fraction (f) for IVIM. Two experienced researchers independently performed region of interest (ROI) analysis for quantitative measurements (Figure 2 and Figure 3). For HCC lesion, a free-hand ROI was drawn along the tumor margin at the slice of largest tumor diameter, excluding necrotic and hemorrhage areas. For liver parenchyma, three circle ROIs were placed on the right liver lobe, avoiding major vessels, tumor, and artifact. Statistical differences between conventional and SMS-accelerated diffusion parameters of HCC and liver parenchyma were assessed using pair t test or Wilcoxon signed rank test, where appropriate. Bland-Altman method was used to evaluate the distribution and concordance of quantitative parameters of HCC between conventional and SMS-accelerated sequences.Results
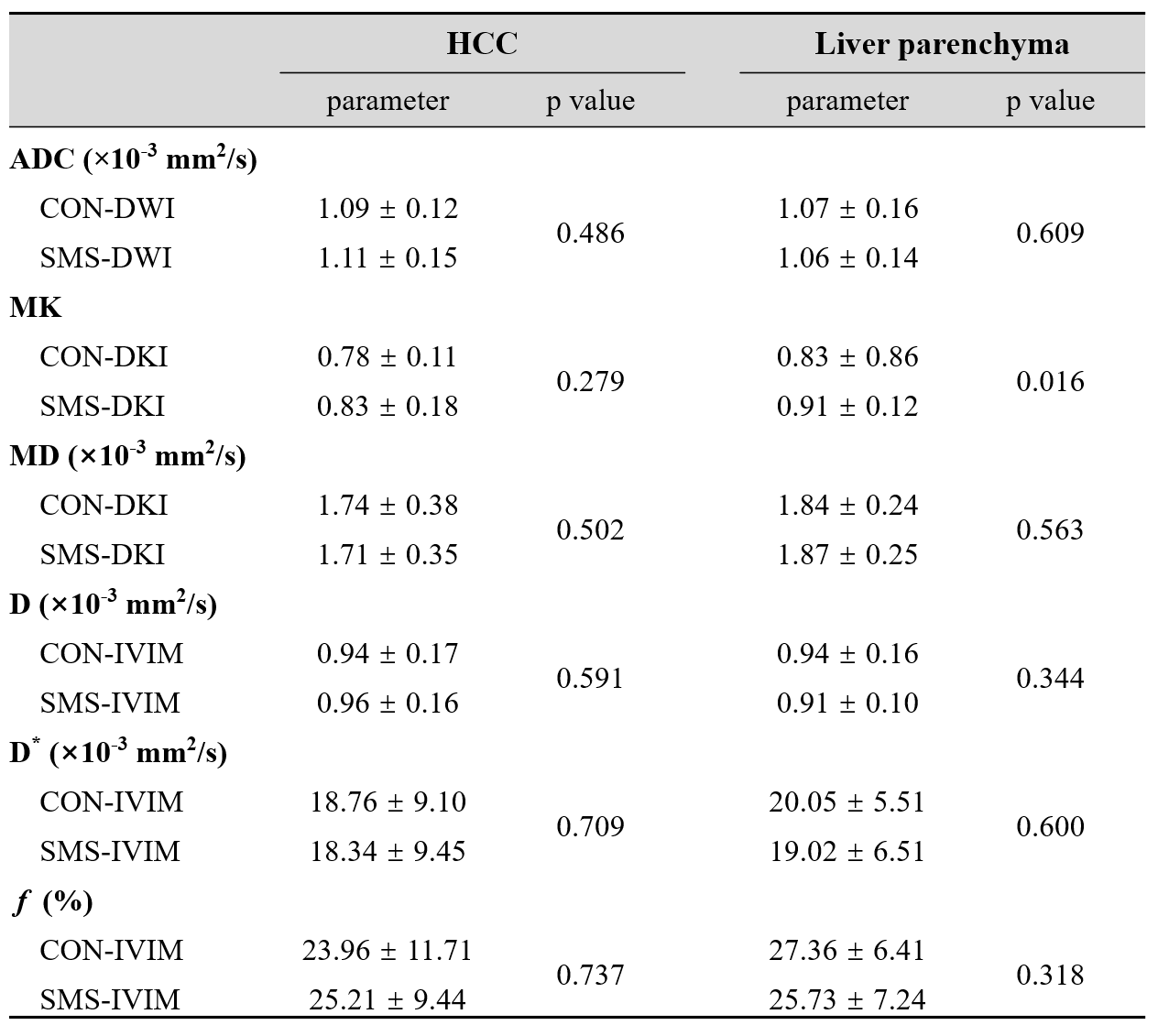
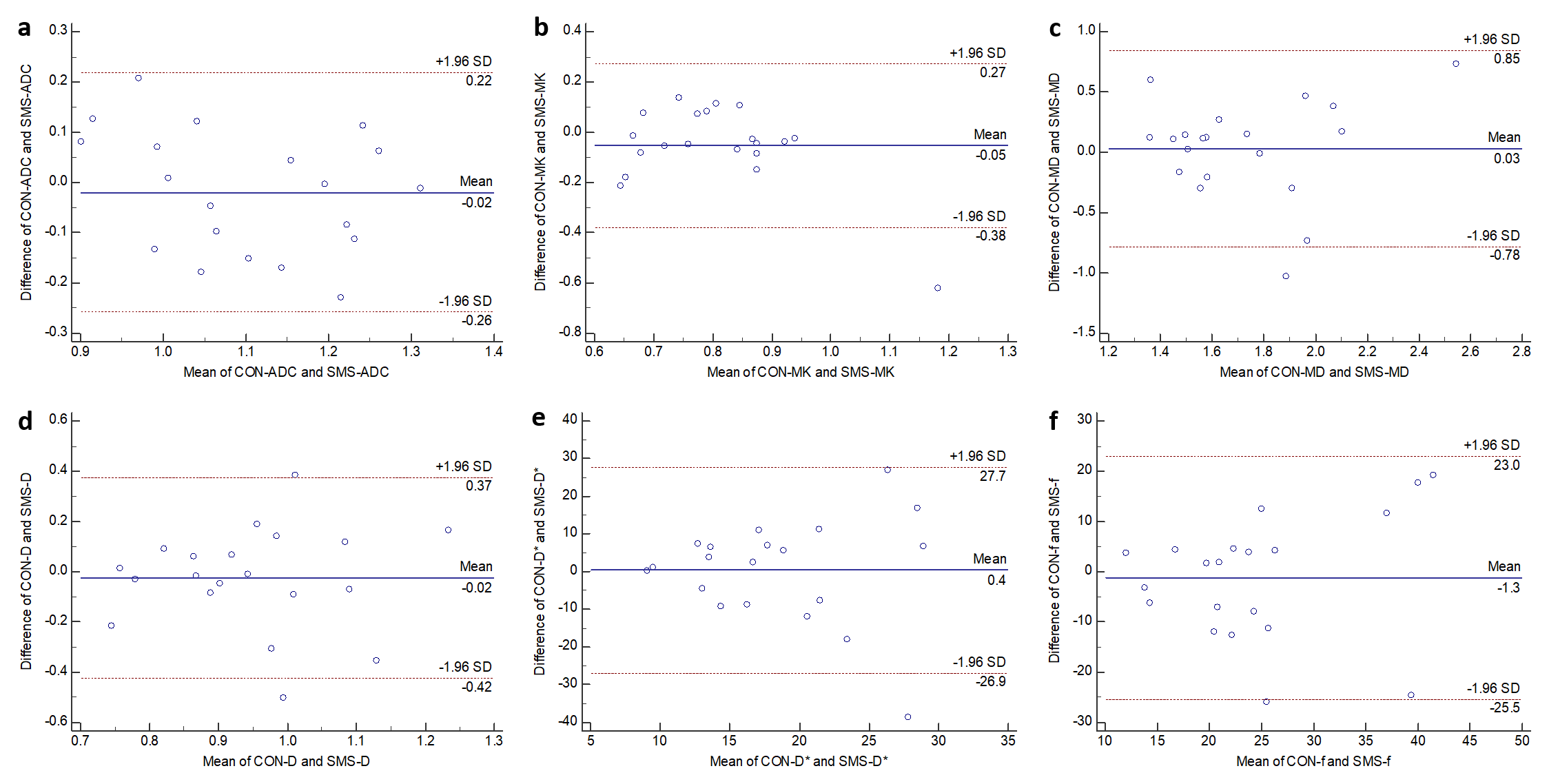
The acquisition times of SMS-DWI, SMS-DKI and SMS-IVIM were approximately 37.35%, 44.44% and 30.69% faster than that of the conventional sequences, respectively. As shown in Figure 4, there was no significant difference of quantitative measurements between conventional and SMS- accelerated diffusion-weighted sequences in HCC (all p value > 0.05). For liver parenchyma, the MK value from CON-DKI was significantly lower than that of SMS-DKI (0.83 ± 0.86 versus 0.91 ± 0.12, p = 0.016), while other quantitative diffusion parameters did not differ significantly between conventional and SMS-accelerated sequences (all p value > 0.05). As shown in Figure 5, Bland-Altman plots demonstrated good agreement of quantitative parameters in HCC between conventional and SMS-accelerated diffusion sequences, with acceptable absolute mean biases and most measurements within the limits of agreement (LOA).Discussion
Thanks to the specialized multiband radiofrequency (RF) pulse and the information from coil sensitivity, SMS technique can simultaneously excite multiple slices and acquire image data at the same time. Recently, Xu et al. found SMS technique provided considerable scan time reduction for abdominal DWI with equivalent quantitative parameters compared with the nonaccelerated sequences, which was in good accordance with our study7. In addition to the good agreement of conventional and SMS-accelerated diffusion parameters in HCC, we also found the MK value in the CON-DKI was significantly lower than that of SMS-DKI in liver parenchyma. Similarly, the trend of increased liver MK with increased acceleration factor was also reported8. Moreover, other studies have shown mixed results regarding the difference between CON-ADC and SMS-ADC in the liver5,9, probably because the scanning protocols were different among these studies.Conclusion
SMS technique can significantly accelerate the acquisition of diffusion weighted sequences, and SMS-accelerated diffusion sequences provide quantitative parameters similar to conventional sequences in HCC, showing great promise in clinical applications.Acknowledgements
None.References
1. Piana G, Trinquart L, Meskine N, et al. New MR imaging criteria with a diffusion-weighted sequence for the diagnosis of hepatocellular carcinoma in chronic liver diseases. Journal of Hepatology, 2011, 55(1): 126-132.
2. Surov A, Pech M, Omari J, et al. Diffusion-weighted imaging reflects tumor grading and microvascular invasion in hepatocellular carcinoma. Liver Cancer, 2021, 10(1): 10-24.
3. Li X, Zhang K, Shi Y, et al. Correlations between the minimum and mean apparent diffusion coefficient values of hepatocellular carcinoma and tumor grade. Journal of Magnetic Resonance Imaging, 2016, 44(6): 1442-1447.
4. Ni P, Lin Y, Zhong Q, et al. Technical advancements and protocol optimization of diffusion-weighted imaging (DWI) in liver. Abdominal Radiology, 2016, 41(1): 189-202.
5. Taron J, Martirosian P, Erb M, et al. Simultaneous multislice diffusion‐weighted MRI of the liver: Analysis of different breathing schemes in comparison to standard sequences. Journal of Magnetic Resonance Imaging, 2016, 44(4): 865-879.
6. Phi Van V D, Becker A S, Ciritsis A, et al. Intravoxel incoherent motion analysis of abdominal organs: application of simultaneous multislice acquisition. Investigative Radiology, 2018, 53(3): 179-185.
7. Xu H, Zhang N, Yang D W, et al. Feasibility study of simultaneous multislice diffusion kurtosis imaging with different acceleration factors in the liver. BMC Medical Imaging, 2021, 21(1): 1-9.
8. Xu H, Zhang N, Yang D W, et al. Scan time reduction in intravoxel incoherent motion diffusion-weighted imaging and diffusion kurtosis imaging of the abdominal organs: using a simultaneous multislice technique with different acceleration factors. Journal of Computer Assisted Tomography, 2021, 45(4): 507-515.
9. Xu J, Cheng Y J, Wang S T, et al. Simultaneous multi-slice accelerated diffusion-weighted imaging with higher spatial resolution for patients with liver metastases from neuroendocrine tumors. Clinical Radiology, 2021, 76(1): 81. e11-e19.
Figures